Review
ABSTRACT
Since the beginning of medicine, palpation has been the primary semiologic method used to detect abnormalities during clinical examination. The mechanical properties of soft tissues are usually related to changes in stiffness. However, changes in stiffness and echogenicity of soft tissues are not always correlated. Elastography has emerged in the last decade as a new method that, when used in association with ultrasonography, can provide information about the acoustic properties (echogenicity and texture) and mechanical attributes (stiffness) of a region of interest in a specific tissue. The objective of this article is to review the literature on the physical principles of elastography and to describe several features of the elastographic imaging process to provide a better understanding of this new technique and its potential utilization in the veterinary field.
Key words: Ultrasonography, elastography, shear wave, stiffness, tumor.
INTRODUCTION
Since the beginning of medical practice, palpation has been used to detect the presence of abnormalities in tissue consistency that could indicate the presence of pathology. The success of this method rests on the fact that the mechanical properties of diseased tissue are typically different from those of the adjacent normal tissue. However, palpation is of limited usefulness in detecting masses located deeply in relation to the skin surface. The assessment of other properties associated with diseased tissue, including water content, tissue density and acoustic interaction capacity, has prompted the emergence of the diagnostic imaging field, which currently makes possible imaging that offers resolution far beyond the limits of palpation (Konofagou, 2004).
The mechanical attributes of soft tissues depend on their molecular constitution (the presence of fat, collagen fibers, elastin and water, among others) and on the micro- and macroscopic structural organization of the tissues. These attributes include the elasticity, stiffness and mobility shown by a tissue in response to forces applied to it (Konofagou, 2004). Pathological changes are usually correlated with changes in tissue stiffness in many cases, the small size of a lesion and/or its deep location prevents its detection or evaluation by palpation, despite the fact that it differs from normal tissue in stiffness and mobility. In addition, lesions may or may not exhibit acoustic properties that render them detectable by ultrasonography. Because the mechanical attributes and echogenicity of tissues are not always correlated, combining data on these properties is expected to reflect tissue structure and pathology and to provide greater diagnostic accuracy. For example, although harder than adjacent tissue, prostate tumors may be sufficiently small to be not observable by normal ultrasonography. This is also true in the case of diffuse diseases; liver cirrhosis, for example, significantly increases the stiffness of liver tissue, although in early stages of the disease sonographic images may be within normal limits on conventional ultrasonography examination (Konofagou, 2004).
Elastography, which has emerged in the last decade, offers a very promising imaging method when combined with ultrasonography. Used together, these methods provide data on the acoustic properties and mechanical attributes of an area of interest in relation to adjacent tissues (O’Brian and Holmes, 2007). The proper inter-pretation of images generated using this technological resource requires an understanding of the mechanical attributes of the tissue in question, that is, the relationship between stiffness and elasticity, as well as knowledge of the various processing methods that can be used with elastographic images (O’Brian and Holmes, 2007). This study aims to perform a review of the literature published on the physical principles of elastography with the goal of helping practitioners to understand the potential applications of this new diagnostic tool.
TISSUE MECHANICAL PROPERTIES
The responses of tissue to applied mechanical forces (that is, compression, traction, tension and elasticity) are considered their mechanical properties. Depending on the material (live tissue) and temperature, the tension (stress) applied to a medium is approximately proportional to the deformation (strain) on the tissue. The ratio of proportionality between the applied stress and the resulting strain is called the elasticity modulus or Young's modulus (Lai, 2009). Young’s modulus (E) is a measure of a material’s resistance to compressive deformation. Tissue deformations occur in response to stress (σ) applied to the tissues, and this stress is related to the force applied. The deformation that occurs is known as the strain (ε). Tissues with higher Young’s moduli, such as fibrous tissues, are more resistant to deformation than other more compliant tissues such as fat.
To understand the application of these physical principles to the elastographic method and because soft tissues are typically composed of heterogeneous and complex material, it is also important to understand the following:
1. The force applied to the tissue is considered static; that is, the data acquisition time is very short compared to the time during which the force acts to cause changes. Thus, the applied force may be considered constant during data acquisition, reducing the complexity of the resulting dynamic viscoelasticity equation.
2. The tissue axial displacement is very small, on the order of less than 1%; therefore, the resulting equation is considered to describe a linear force (that is, the amount of strain resulting from an applied stress is not a function of the absolute stress applied).
3. The material is elastic (that is, the tissue returns to its non-deformed state when the applied stress is removed, and the deformation state is not dependent on the rate of the applied stress), isotropic (that is, the tissue’s material properties are not orientation-dependent) and incompres-sible (that is, the volume of the tissue remains the same when strained due to its high water content) (Sarvazyan, 1993).
To simplify the analysis and interpretation of elastography, stress and strain can be related to each other by Young’s modulus (that is, stress is a function of strain): σ = Eε.
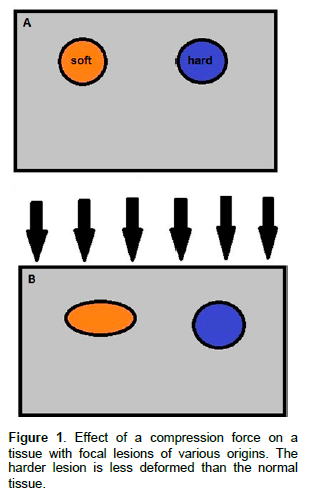
When an elastic medium undergoes compression due to the application of a constant uniaxial force, all points in the medium whose main components are arranged along the axis of compression and motion experience some level of longitudinal displacement. The resulting level of displacement of a given element will be greater or smaller if one or more tissue elements have stiffness parameters that differ from those of other elements (Ophir et al., 1991; Sarvazyan, 1993). A harder tissue element will undergo less deformation when subjected to compression than other elements of lower stiffness (Figure 1).
The longitudinal (axial or lateral) displacement of the elements of a tissue can be estimated through the analysis of ultrasound signals detected using a diagnostic ultrasonography device. If the amount of tension necessary to obtain a certain degree of deformation of the medium is known, the elasticity of the medium being studied can be calculated. The higher the modulus of the medium is, the greater the tension required for deformation of the medium; thus, the stiffer the material. The linear relationship between these quantities is known as Hooke’s law (Sarvazyan, 1993). These data are usually gathered in the following order:
1. A sample of radiofrequency echoes obtained in the region of interest in the tissue under study is collected.
2. A small compression of the tissue is performed using a transducer along the same direction of the sound beam.
3. A second linear echo sample is acquired after compression of the same region of interest (Ophir et al., 1991; Palmieri and Nightingale, 2011).
The data are compared using cross-correlation techniques in which similar linear echoes are subdivided into small time windows and paired, thereby permitting mathematical calculation of the change in the region of interest after compression at several points within the area (Ophir et al., 1991). Tissues may show greater or smaller viscoelastic behavior depending on the presence and quantity of certain components, including fluid flow at the site and the ability of fibers within the tissue to under-go stress relaxation. Thus, most soft tissues appear iso-tropic when a mechanical stress force is applied (Parker et al., 1990; Sarvazyan, 1993; Palmieri and Nightingale, 2011), although there is evidence that some soft tissues, for example, muscles, possess anisotropic mechanical and ultrasonographic properties (Levinson, 1987).
The introduction of viscosity to the tissue description allows tissue stiffness to be analyzed as a function of the excitation frequency (that is, E(f)). Higher frequency exci-tations yield stiffer tissue responses than lower frequency excitations (Sarvazyan,1993). The use of a device that permits results to be obtained in real time, as is the case in ultrasound imaging, is optimal for mathematically describing the mechanical behavior of the analyzed tissues and determining all the factors involved. Elasticity imaging modalities generate images of tissue stiffness (Ophir et al., 1991; Palmieri and Nightingale, 2011). They accomplish this by applying stress to the tissues using an external excitation source, an internal, physiological mo-tion source or an acoustic radiation force and measuring the resulting deformation (displacement) that occurs in response to the applied stress. Based on a known stress/strain relationship, the deformation that occurs in response to the applied stress can be related to the tissue stiffness.
FORCES AND STRESS SOURCES
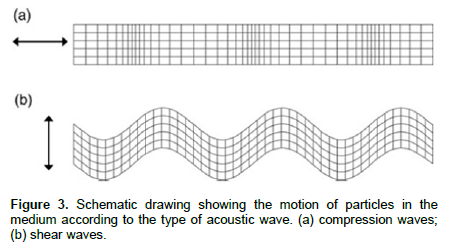
Elasticity imaging requires a source of stress to deform tissue so that relative or absolute responses to that stress can be measured to generate elasticity images. These excitation sources can be external to the body and include mechanical punches, vibrating rods and com-pression plates. We may consider two types of waves resulting from a specific stress source traveling through a medium: compression and shear waves (Figure 2).
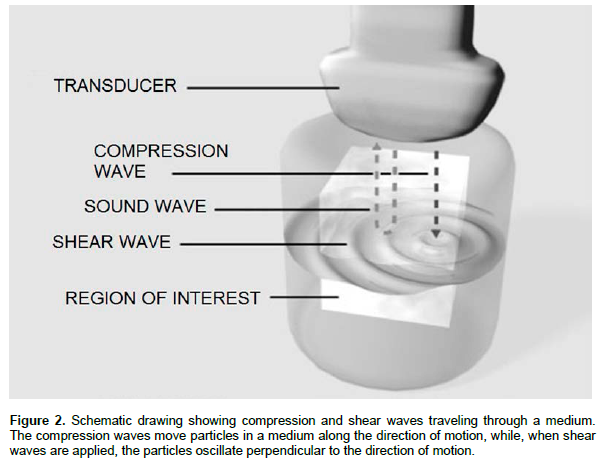
Compression waves
With compression waves, the particles of a medium oscillate in the direction of motion. The tissues of the body have substantially different mechanical properties because their mechanical functions are different. Furthermore, the estimation and imaging of tissue dis-placement is, by definition, a three-dimensional problem. When a tissue is deformed, the apparent proximal non-compressibility of most soft tissues means that stress components are generated in all directions simulta-neously (Levinson, 1987; Han et al., 2003). In ultrasound elasticity imaging, the ultrasound transducer can be used to apply compression to the tissues of interest through the skin surface. The advantage of using this excitation source is that known stresses or strains can be applied to large volumes of tissue, which can be useful when screening for lesions. A potential drawback to external excitation, however, is the limited penetration of these applied stresses into deep organs of interest (example, the liver in an obese patient) due to attenuation of the stress from the skin surface or a physical barrier such as the presence of abdominal ascites.
Shear waves
With shear waves particles oscillate perpendicular to the direction of motion. Shear waves are important for elastography because calculation of stiffness is performed using a mathematical formula (Young's modulus) that requires wave velocity data (Hoskins, 2012). Local displacement of the tissue occurs as shear waves pass through it. These local displacements cause changes in the returning echo pattern over time that can be monitored using methods of axial image correlation. However, this requires that the time between subsequent ultrasound pulses be less than 0.5 ms, which is equivalent to a minimum pulse repetition frequency (PRF) of 2,000 Hz. This parameter can be easily adjusted in devices that produce one-dimensional images (for example, in M-mode). However, a PRF is required to produce two-dimensional multiaxial images; such images cannot be obtained using conventional technology devices (Levinson, 1987; O’Brian and Holmes, 2007; Hoskins, 2012).
Another stress source that can be used in ultrasound elasticity imaging to overcome the challenge of introducing stress into internal organs of interest is the acoustic radiation force, the force that results from transfer of momentum from the propagating ultrasonic wave to the sound-absorbing soft tissue. This transfer of momentum applies a force in the direction of the wave propagation; thus, through the use of longer and/or stronger acoustic pulses which are typically used in diagnostic ultrasound, transient tissue deformation on the order of microns can be generated. The acoustic radiation force (F) is a force applied over a volume of material, and it is related to the acoustic attenuation of the tissue (α), the acoustic intensity (I) and the speed of sound (c) by the formula F=2αI/ c.
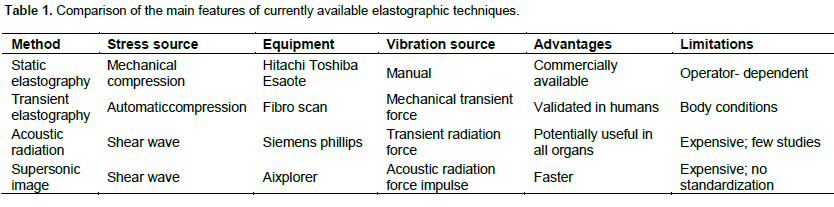
The ultrasound systems that are currently commercially available can be classified according to their capacity for wave emission and detection (Ophir et al., 1991; Nightingale et al., 2002; Palmieri and Nightingale, 2011; Jaffer et al., 2012). The elasticity of tissue can be inferred in three ways: by generation of shear waves using an external mechanical agent; by sonoelastography that involves automatic generation of shear waves and by generation of shear waves using acoustic radiation force or shear force associated with a B-mode image (Table 1). The types of stress sources described above can be applied (quasi) statically (that is, under conditions in which a stress state is applied and held), dynamically (the stress is applied impulsively, that is, there is a transient excitation typically lasting tens to hundreds of microseconds) or harmonically (that is, the stress is applied as a sinusoid of one or more frequencies).
ELASTOGRAPHY IMAGE PROCESSING
Quantitative evaluation of the mechanical parameters of tissues has yielded a broad range of values (Parker et al., 1990). Most studies of the mechanical parameters of tissues have been performed on tissues (muscles, arteries, lungs, tendons, bones, skin, ureter) that were subjected to a tensile force. Conversely, limited data on the compression features of tissues within organs have been gathered. Even fewer studies have measured the elastic resultants of these tissues in vitro (Parker et al., 1990). Some in vivo studies were performed; the results of these studies indicate that the mechanical properties of tissues are significantly different under normal conditions and in the presence of tumorous lesions (Han et al., 2003).
The existence of significant differences in the responses of normal and abnormal tissues to a mechanical stimulus has enabled the development of imaging techniques that reveal the mechanical attributes of a tissue or a region of interest within a tissue (Nightingale et al., 2002; Jaffer et al., 2012). Currently, a variety of techniques can be used to obtain measurements of tissue mechanical properties and process the measurements into an image format that can be used as a diagnostic tool. The commercially available methods can be subdivided into two main types: strain elastography or elastography by mechanical com-pression waves and shear wave elastography performed by shear wave emission (Figure 3) (Hoskins, 2012).
In shear wave elastography, a force is exerted on the tissue, and the imaging system measures the response of the tissue to that force. There are two basic techniques that can be used; both are based on tissue compression. In the first method, the transducer is moved along an axis; this technique is termed strain elastography (A-line correlation) or static elastography. The other technique, which is called sonoelasticity imaging, transient elasto-graphy or Fibroscan, involves the application of low-frequency vibration energy to the tissue followed by simultaneous detection of Doppler ultrasound waves showing the hemodynamic disturbance caused by vibra-tions (Nightingale et al., 2002). In the latter case, data obtained using the Doppler tool generate a result that shows the elastic modulus calculated from the wavelength at the vibration site; that is, they show only the displacement amplitude related to the elasticity of this modulus also along an axial path (Hoskins, 2012).
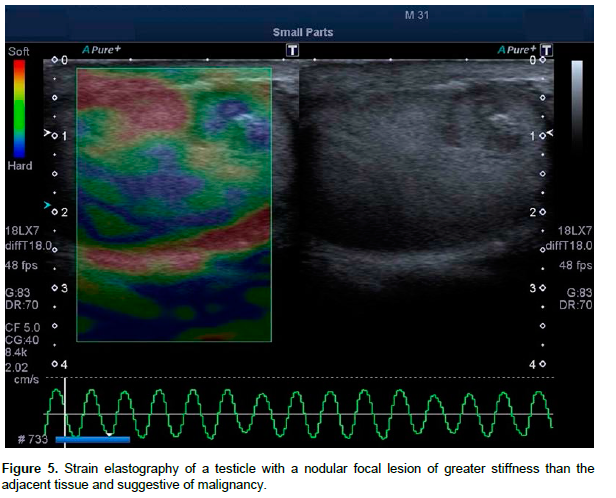
The technique termed strain elastography measures the local response of a tissue subjected to a force and transforms the calculations of longitudinal (axial) dis-placement of the relevant components at different points of a single tissue into an image (Ophir et al, 1991). The resulting image is known as an elastogram (Figure 4). This technique can be used to detect tissue movement, tissue compression and extension along the axis of displacement and are especially used in real-time in clinical practice (Hoskins, 2012). They may be performed in real-time or not, using ultrasound devices equipped with specific software that is capable of evaluating the physical properties of a tissue (Figure 5) and assessing its degree of stiffness in relation to the adjacent tissue through compression of the evaluated site (Jaffer et al., 2012).
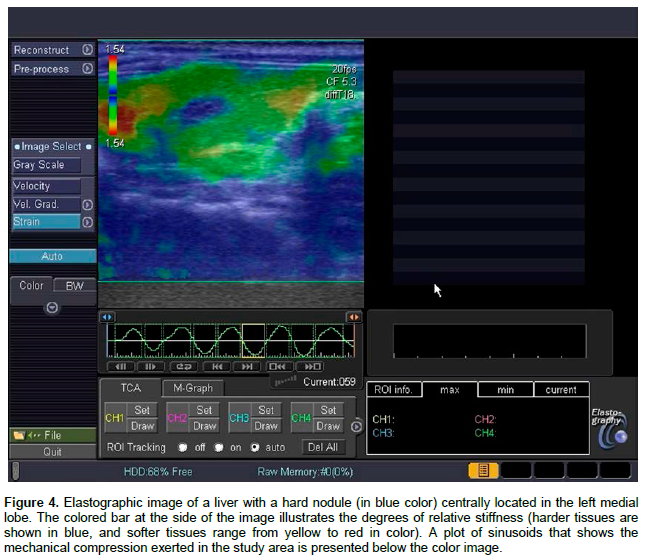
In static elastography, a sound beam is emitted by the transducer while a slight manual mechanical compression is simultaneously performed. An elastogra-phic image is generated from the tissue deformation, with the software performing a comparative analysis of the moment of compression and the resultant after com-pression. Harder tissues deform less upon compression, while tissues more susceptible to compression show greater deformation (Saftoiu et al., 2007). The deformity experienced by the tissue is represented on a color scale, according to the elastic variation: red corresponds to softer tissues, green to tissues showing intermediate deformity, and blue to tissues with less deformation, that is, of greater stiffness (Saftoiu et al., 2007).
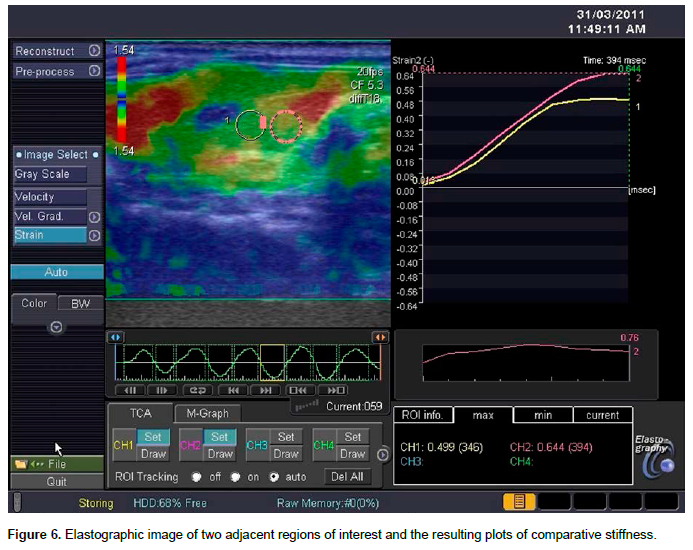
It is important to note that strain elastography does not provide an exact mathematical image of the elastic modulus itself. In strain elastography, a stiffness index can be estimated by comparing the stiffness of the lesion with that of an adjacent reference region. Thus, the operator must remember that the measurement is sensitive to the positioning of the reference region; to obtain a reliable index, the reference region should be at the same depth as the lesion under study (Figure 6). This is important because the stress caused by compression (that is, the force per unit area) often changes with depth.
In a uniform tissue such as the liver or at a phantom, stress and elasticity decrease with increasing depth (Hoskins, 2012). Thus, depth becomes a limitation because lesions at depths greater than 5 cm cannot be compressed sufficiently to be evaluated by this imaging technique. This primarily occurs in organs located at greater depths or in obese patients (Hoskins, 2012). Variations of elastography techniques, including real-time elastography and transient elastography, have been described in the literature. These variations are the result of technological development aimed at finding optimal methods for different clinical indications (Hoskins, 2012).
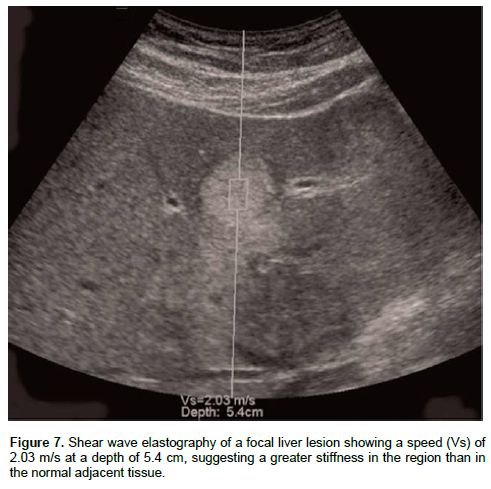
Another technique that has been described in the literature is based on the propagation of an acoustic radiation force impulse (ARFI) or a shear waveform. This force is capable of causing tissue displacement without the need for manual compression. This technique can provide both strain and sheare wave data (Figure 7). The displacement caused by the shear wave is minimal, although the focus of a high-mechanical index pulse may produce displacements of up to 20 µm, with the tissue returning to its initial position in 5 ms (Nightingale et al., 2002). The displacement can be detected using the strain elastography technique and can be used at greater depths and they are permitted by simple strain elastography because the force originates directly from the focal region of the transducer. Moreover, the subjectivity of the measurements resulting from the variation in compression force applied by the operator ceases to exist with this method. Thus, the method is more accurate and involves less inter-observer variation and greater reproducibility (Jaffer et al., 2012).
Shear wave elastography involves a step forward in the reconstruction of the elastic modulus resulting from axial displacement in real-time, as it measures the waves able to cause elastic deformation in the direction of motion, thereby enabling the user to calculate the tissue stiffness from the data gathered in the region of interest (Kallel et al., 1999). Several studies that show the accuracy of estimates of the displacement of waves in various tissues have been published (Konofagou et al., 1999). Shear wave elastography or shear wave elastography is currently performed using devices that rely on focused ultrasound wave propagation to generate marginal and orthogonal (or shear) waves within the organ. This process may be performed using either ARFI imaging devices or supersonic shear wave imaging devices (Konofagou et al., 1999).
PRIMARY APPLICATIONS OF ELASTOGRAPHY
Among the primary applications of the method, it is important to emphasize the use of so-called transient elastography. Transient elastography was the first elasto-graphy method to be commercially used. It is performed using a device termed Fibroscan® that was specifically developed to quantify liver fibrosis without, however, forming an image. This device has the ability to send elastic waves together with the sound beam. These waves go through the tissue at speeds directly propor-tional to tissue stiffness. The technique offers advantages over conventional biopsy for the quantification of liver fibrosis: it is risk-free for patients, it is painless, and it evaluates liver tissue within a 1-cm-thick and 2-cm-deep cylindrical fragment that is 100 times larger than the fragment removed by biopsy (Serejo et al., 2007; Rivero-Juárez et al., 2012). However, studies show that some conditions associated with chronic liver disease, including liver inflammation and congestion, biliary obstruction and portal hypertension, may increase the elasticity of the liver, making the method inconclusive in 20% of cases (Friederich-Rust et al., 2008; Castera and Pinzani, 2010). Furthermore, some technical difficulties, including the high cost of the device, the long user learning curve and the impossibility of performing the technique in the presence of ascites and in obese patients, limit the use of the method (Hoskins, 2012).
Mechanical or real-time elastography involves the use of ultrasound devices with specific software and offers the advantages of lower cost and ease of operation. Most ultrasound device manufacturers produce machines that use this method. Notwithstanding its advantages, mechanical elastography is considered operator-dependent because it requires manual application of the force; for this reason, it has low reproducibility. The literature reports that mechanical elastography has been used as an auxiliary method in conventional ultrasound imaging for differentiating malignant from benign focal lesions (O’Brian and Holmes, 2007). Preliminary studies of its use in liver tissue have aimed to standardize the technique and evaluate its diagnostic value in detecting focal and diffuse lesions, differentiating malignant and benign processes (Carvalho et al., 2012), and detecting degenerative and inflammatory processes (Orlacchio et al., 2012) in addition to quantifying fibrosis in human (Boozari et al., 2010) and canine (Rivero-Juárez et al., 2012) patients. For these reasons, many expectations have been generated regarding this new technique (Jaffer et al., 2012).
Lastly, methods based on shear wave propagation (ARFI and supersonic shear waves) offer several advantages compared to other methods. They enable the procedure to be combined with routine real-time ultrasound even in overweight patients or in patients with ascites because they generate greater penetration of the mechanical wave. Furthermore, the technique provides better accuracy in the calculation of tissue elasticity and better reproducibility because the result is independent of the skill of the operator (Friedrich-Rust et al., 2009; Muller et al., 2009; Boursier et al., 2010). The primary disadvantages of the shear wave propagation techniques are related to the cost of the device, which often precludes its use outside of reference centers for human and veterinary medicine. We may also add that another disadvantage of the shear wave propagation method is the size of the sample measured, which is small and not always significant in relation to the whole organ in the case of diseases without diffuse parenchymal infiltration (Friedrich-Rust et al., 2008). Studies using this technique are still very recent, and there are no established benchmarks in the veterinary literature.
Elastography has the potential to be more challenging in animals than humans. Obtaining measurements from deeper regions within the liver was sometimes problematic as these regions had a tendency to show increased movement during the respiratory cycle, com-pared with the more subtle movement of the superficial tissues. Breath holding is commonly used in human elastography but, in veterinary medicine, is not possible to request conscious patients to breath hold or remain still; therefore, the values obtained are likely to be more variable. Some patients that were uncooperative and moving and patients that were panting heavily were noted to produce invalid readings (XXX readout). To minimize the impact of respiratory motion on the accuracy and reliability of results, efforts can be made to time measurements such that acquisition to occur during the normal end-expiratory pause. Another possible solution, in some instances, would be to sedate or anesthetize animals for the procedure to prevent voluntary movement, permit control over respiration and allow breath-hold techniques to be employed (Holdsworth et al., 2014). Besides the application of the Elastography on the evaluation of the hepatic parenchyma, recently, in several case reports this technique is also being used on the evaluation of different organs.
This technique has proved to be immensely useful in assessing lymph nodes in the neck and maxillofacial region (Tan et al., 2010). Information on lymph node stiffness would likely be clinically useful for guidance of percutaneous biopsy and/or nodal dissection. Such information might also improve patient follow-up by enabling early detection of cancer recurrence (Lyshchik et al., 2007). Elastography has been used to identify metastatic lymph nodes, measure masseter stiffness (Ariji et al., 2009) for the purpose of massage and to evaluate focal lesions in major salivary glands (Bhatia et al., 2010; Das et al., 2011).
Pancreatic applications of ultrasound elastography are relatively recent because of the difficulty in pressing the pancreas, which is located deep in the body. The lesion detection rate and diagnostic rate could be improved to over 90% by the combined use of B-mode and elastographic images, compared to using b-mode images alone (Uchida et al., 2009; Park et al., 2014). This tech-nique has been reported to be useful in characterizing and differentiating normal pancreas, chronic pancreatitis and acute pancreatitis. In a study using ARFI elasto-graphy to evaluate the pancreas tissue, the authors conclude that mean ARFI values less than 2,2m/s for pancreatic parenchyma may be exclude an acute pancreatic inflammatory disease. If mean ARFI value is higher than 2,2m/s, an acute pancreatitis attack may be diagnosed. Higher ARFI values in acute pancreatitis are due to increased fluid content in the inflamed organ making the tissue hard (Mateen et al., 2012). Another study (Janssen et al., 2007) concluded that chronic pancreatitis and hard tumors cannot be distinguished by elastography, probably because of their similar fibrous structure and calcification, leading to high ARFI values (Janssen et al., 2007; Park et al., 2014).
Spleen stiffness as measured by noninvasive imaging modalities, as elastography, has more recently been reported to be a marker for prediction of portal hypertension (Grgurevic et al., 2011). Spleen stiffness as measured by the mean share wave velocity has a close relationship with portal vein pressure and can be used to predict the presence of cirrhosis and varices in patients with liver fibrosis and portal hypertension. When portal vein pressure is higher, the spleen is stiffer, and the mean share wave velocity is increased, whereas when portal vein pressure is lower, the spleen becomes softer, and the mean share wave velocity is decreased (Gao et al., 2012). The explanation for these results would be that portal hypertension would initially and directly induce hypersplenism with associate histologic changes in the spleen (Ran et al., 2012).
Some recent studies showed that acoustic radiation force impulse (ARFI) elastography was useful for the differentiation between benign and malignant thyroid nodules. The mean share wave velocity value of malignant thyroid nodules was significantly higher than that of normal tissue or benign nodules (Zhang et al., 2014). In a study about clinical application of thyroid elastography including 92 consecutive patients with a single nodule, the researchers calculated the sensitivity to be 97% and the specificity to be 100% from predicting thyroid malignancy (Rago et al., 2007). In practice, elastography is usually performed as an extension of convencional US and not as an independent test (Kwak and Kim, 2014). Vorländer et al. (2010), confirmed the possibility of measuring the increased stiffness in Hashimoto disease by using magnetic resonance elastography and in other study was reported the possible possible usefullness of ARFI to confirm the presence of Graves disease and chronic autoimmune thyroiditis (Zaleska-Dorobisz et al., 2014).
Another common application of ultrasound elasto-graphy is in breast examinations. The combination of conventional ultrasound, elastography and virtual touch tissue quantification technology are proven to have high diagnosis performance on detecting breast lesions and diagnostic of breast cancer. The stiffness of breast lesions is closely associated with the degree of malig-nancy, and is the basis for the evaluation of benign or malignant tumors by elastography. However, due to the overlap in the hardness of benign and malignant tumors, actual clinical application would benefit from combining these methods with conventional ultrasound to optimize the accuracy of breast tumor diagnoses. Furthermore, elastography would increase the sensitivity of B-mode sonography in distinguishing benign and malignant lesions, in consequence, could potentially reduce unnecessary biopsies. This seems to be an important aim because nearly 80% of biopsied breast lesions turn out to be benign, according to the American Cancer Society (Jiang et al., 2014; Zaleska-Dorobisz et al., 2014). In a study to evaluate the applicability of acoustic radiation force impulse elastography as a complementary method in diagnosing mammary neoplasia in 50 female dogs, the autors conclude that elastography helped to differentiate between malignant and benign mammary neoplasm. Future studies with larger number of samples should be performed in order to determine the sensitivity and specificity of this imaging technique in the evaluation of mammary tumors in dogs (Feliciano et al., 2014).
Elastography is constantly being improved and it also allows us to show the lesions that are in the prostate gland. This method targeted approach detects high-risk prostate cancer more reliably than biopsy, requires a reduced number of cores for prostate cancer detection, and enhances the overall sensitivity in the combined biopsy setting (Junker et al., 2014). Inconsequence, it helps in making a decision on whether to carry out a biopsy and thanks to higher precision additional contuses is not necessary (Zaleska-Doronisz et al., 2014). Trans rectal elastography revealed carcinoma in 93% cases in a study with 97 patients. In these study, the detectability of carcinoma was higher than in trans rectal ultrasound – 59% in 16 patients, but the autors (Junker et al., 2014) noticed that the effectiveness of sonoelastography of the prostate gland depends on malignant tumor size. In the case of foci of 0 to 5 mm the effectiveness of this method is 6/62, 6 to 10 mm is 10/37, 11 to 20 mm is 24/34 and the highest detectability of 14/14 is in the case of tumors bigger than 20 mm (Zaleska-Dorobisz et al., 2014).
Application of these new ultrasound techniques to the kidney has been shown to be possible and the first results are encouraging. However, the kidney is a much more complex organ than the liver, with two compart-ments and a high vascularity. Increased cellularity and increased intratubular and interstitial hydrostatic pressure would change and bias the elasticity values obtained within the renal parenchyma. But the correlation between renal elasticity quantification and intrarenal pathological changes is quite controversial in the literature. One possible explanation for such discrepancies is the non-specificity of stiffness changes related to interstitial fibrosis. The results of recent studies suggest that the degree of renal cortical stiffness does not reflect any specific intrarenal change, such as fibrosis, but rather the association of several renal microlesions, especially chronic lesions. Therefore, more experience is needed in preclinical models and in patients’ cohorts with pathological correlation to better understand which are the physical factors of variation and the histopathological causes of elasticity changes (Grenier et al., 2013).
CONCLUSION
The primary challenges that complicate the widespread and routine use of elastography in human (Palmieri and Nightingale, 2011) and veterinary medicines are:
1. The difficulty of access in obese patients and to some organs, including the liver, given the thoracic skeleton; this is true especially in the case of veterinary medicine because some breeds of dogs have keel-shaped deep chests, complicating liver examination.
2. The need for devices that support the new technology and are affordable.
However, elastographic imaging methods have a promising future given their safety and the good image resolution of current conventional diagnostic ultrasound devices (Table 1) (Palmieri and Nightingale, 2011). The main areas in which we may expect significant progress and clinical research for the application of this technique are:
1. Characterization of the stiffness of tissues with respect to the presence of structural lesions in organs (Holdsworth et al., 2014; White et al., 2014).
2. Monitoring of processes of tissue fibrosis in various organs.
3. Tumor characterization based on the image pattern associated with the tumor’s mechanical properties (including stiffness and mobility);
4. Early detection of malignant lesions using three-dimensional characterization of the affected area.
5. Lastly, applications at the cellular level through the use of high-frequency transducers for small organs (Konofagou, 2004).
These are some examples of the numerous possibi-lities various elastography methods may provide for clinical applications in veterinary medicine in the coming years.
ACKNOWLEDGEMENT
Special thanks are extended to the São Paulo State Research Foundation (Fundação para Amparo a Pesquisa do Estado de São Paulo - FAPESP) for funding the studies conducted by the authors in the field of ultrasound elastography.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
|
Ariji Y, Katsumata A, Hiraiwa Y, Izumi M, Iida Y, Goto M, Sakuma S, Ogi N, Kurita K, Ariji E (2009). Use of sonographic elastography of the masseter muscles for optimizing massage pressure: a preliminary study. J. Oral. Rehabil. 36:627-635. Crossref |
||||
|
Bhatia KS, Basalkar DP, Lee YP, Wong KT, King AD, Yuen HY, Ahuja AT (2010). Evaluation of real time qualitative sonoelastography of focal lesions in the parotid and submandibular glands: applications and limitations. Eur. Radiol. 20:1958-1964. Crossref |
||||
|
Boozari B, Potthoff A, Mederacke I, Hahn A, Reising A, Rifai K, Wedemeyer H, Bahr M, Kubicka S, Manns M, Gebel M (2010). Evaluation of sound speed for detection of liver fibrosis. Prospective comparison with transient elastography and histology. J. Ultrasound Med. 29:1581-1588. Pubmed |
||||
|
Boursier J, Konate A, Guilluy M, Gorea G, Sawadogo A, Quemener E (2010). Learning curve and interobserver reproducibility evaluation of liver stiffness measurement by transient elastography. Eur. J. Gastroenterol. Hepatol. 22:1074-1084. Crossref |
||||
|
Carvalho CF, Chammas MC, Cogliati B, Stefano JT, Carrilho FJ, Oliveira CPM (2012). Elastography and contrast-enhanced ultrasonography improves early detection of hepatocellular carcinoma in an experimental model of NASH. J. Hepatol. 56:S495. Crossref |
||||
|
Castera L, Pinzani M (2010). Non-invasive assessment of liver fibrosis: are we ready? Lancet 375:1419-1420. Crossref |
||||
|
Das D, Gupta M, Kaur H, Kalucha A (2011). Elastography: the next step. J. Oral. Sci. 53:137-141. Crossref |
||||
|
Feliciano MAR, Maronezi MC, Pavan L, Castanheira TL, Simões APR, Carvalho CF, Canola JC, Vicente WRR (2014). ARFI elastography as a complementary diagnostic method of mammary neoplasia in female dogs – preliminary results. J. Small Anim. Pract. 55:504-508. Crossref |
||||
|
Friedrich-Rust M, Ong MF, Martens S, Sarrazin C, Bojunga J, Zeuzem S, Herrmann E (2008). Performance of transient elastography for the staging of liver fibrosis: a meta-analysis. Gastroenterology 134:960-974. Crossref |
||||
|
Friedrich-Rust M, Wunder K, Kriener S, Sotoudeh F, Richter S, Bojunga J, Herrmann E, Poynard T, Dietrich CF, Vermehren J, Zeuzem S, Sarrazin C (2009). Liver fibrosis in viral hepatitis: noninvasive assessment with acoustic radiation force impulse imaging versus transient elastography. Radiology 252:595-604. Crossref |
||||
|
Gao J, Ran HT, Ye XP, Zhen YY, Zhang DZ, Wang ZG (2012). The spleen stiffness measured with ARFI pre and post TIPS. Clin. Imaging 36:135-141. Crossref |
||||
|
Grenier N, Gennisson JL, Cornelis F, Le Bras Y, Couzi L (2013). Renal ultrasound elastography. Diagn. Interv. Imaging 94:545-550. Crossref |
||||
|
Grgurevic I, Cikara I, Horvat J, Lukic IK, Banic M, Heinzl R, Kujundzic M, Brkljacic B (2011). Noninvasive assessment of liver with acoustic radiation force impulse imaging: increased liver and splenic stiffness in patients with liver fibrosis and cirrhosis. Ultraschall Med. 32:160-166. Crossref |
||||
|
Han LH, Noble JA, Burcher M (2003). A novel ultrasound indentation system for measuring biomechanical properties of in vivo soft tissue. Ultrasound Med. Biol. 29:813-823. Crossref |
||||
|
Holdsworth A, Bradley K, Birch S, Browne W, Barberet V (2014). Elastography of normal canine liver, spleen and liver. Vet. Radiol. Ultrasound 6:620-627. Crossref |
||||
|
Hoskins PR (2012). Principles of ultrasound elastography. Ultrasound 20:8-15. Crossref |
||||
|
Jaffer O, Lung PFC, Bosanac D, Shah A, Sidhu PS (2012). Is ultrasound elastography of the liver ready to replace biopsy? A critical review of the current techniques. Ultrasound 20:24-32. Crossref |
||||
|
Janssen J, Schlörer E, Greiner L (2007). EUS elastography of the pancreas: feasibility and pattern description of the normal pancreas, chronic pancreatitis, and focal pancreatic lesions. Gastrointest. Endosc. 65:971-978. Crossref |
||||
|
Jiang Q, Zhang Y, Chen J, Zhang YX, He Z (2014). Technical evaluation of Virtual Touch tissue quantification and elastography in benign and malignant breast tumors. Exp. Ther. Med. 8:1059-1064. Pubmed |
||||
|
Junker D, De Zordo T, Quentin M, Ladurner M, Bektic J, Horniger W, Jaschke W, Aigner F (2014). Real time elastography of the prostate. Biomed. Res. Int. 2014:180804. Crossref |
||||
|
Kallel F, Price RE, Konofagou EE, Ophir J (1999). Elastographic imaging of the normal canine prostate in vitro. Ultrasonic Imaging 21:201-215. Crossref |
||||
|
Konofagou EE (2004). Quo vadis elasticity imaging? Ultrasonics 42:331-336. Crossref |
||||
|
Konofagou EE, Varghese T, Ophir J, Alam SK (1999). Power spectral strain estimators in elastography. Ultrasound Med. Biol. 25:1115-1124. Crossref |
||||
|
Kwak JY, Kim EK (2014). Ultrasound elastography for thyroid nodules: recent advances. Ultrasonography 33:75-82. Crossref |
||||
|
Lai R (2009). The elastic solid. In: Introduction to continuum mechanics, 4th Edition. Burlington, MA; Pergamon Press. Crossref |
||||
|
Levinson SF (1987). Ultrasound propagation in anisotropic soft tissues: the application of linear elastic theory. J. Biomech. 20:251-260. Crossref |
||||
|
Lyshchik A, Higashi T, Asato R, Tanaka S, Ito J, Hiraoka M, Insana MF, Brill AB, Saga T, Togashi K (2007). Cervical limph node metastases: diagnosis at sonoelastography – initial experience. Radiology 243:258-267. Crossref |
||||
| Mateen MA, Muheet KA, Mohan RJ, Rao PN, Majaz HMK, Rao GV, Reddy DN (2012). Evaluation of ultrasound besed acoustic radiation force impulse (ARFI) and eSie touch sonoelastography for diagnosis of inflammatory pancreatic disease. J. Pancreas 13:36-44. | ||||
|
Muller M, Gennisson JL, Deffieux T, Tanter M, Fink M (2009). Quantitative viscoelasticity mapping of human liver using supersonic shear imaging: preliminary in vivo feasibility study. Ultrasound Med. Biol. 35:219-229. Crossref |
||||
|
Nightingale KR, Soo MS, Nightingale RW, Trahey GE (2002). Acoustic radiation force impulse imaging: in vivo demonstration of clinical feasibility. Ultrasound Med. Biol. 28:227-235. Crossref |
||||
|
O'Brien RT, Holmes SP (2007). Recent advances in ultrasound technology. Clin. Tech. Small. Anim. Pract. 22:93-103. Crossref |
||||
|
Ophir J, Cespedes EI, Ponnekanti H, Yazdi Y, Li X (1991). Elastography: a quantitative method for imaging the elasticity of biological tissues. Ultrasonic Imaging 13:111-134. Crossref |
||||
|
Orlacchio A, Bolacchi F, Antonicoli M, Coco I, Costanzo E, Tosti D, Francioso S, Angelico M, SImonetti G (2012). Liver elasticity in NASH patients evaluated with real-time elastography (RTE). Ultrasound Med. Biol. 38:537-544. Crossref |
||||
|
Palmieri ML, Nightingale KR (2011a). Acoustic radiation force-based elasticity imaging methods. Interface Focus 1:553-564. Crossref |
||||
|
Palmieri ML, Nightingale KR (2011b). What challenges must be overcome before ultrasound elasticity imaging is ready for the clinic? Imaging Med. 3:433-444. Crossref |
||||
|
Park MK, Jo JH, Kwon H, Cho JH, Oh JY, Noh MH, Nam KJ (2014). Usefullness of acoustic radiation force impulse elastography in the differential diagnosis of benign and malignant solid pancreatic lesions. Ultrasonography 33:26-33. Crossref |
||||
|
Parker KJ, Huang SR, Musulin RA, Lerner RM (1990). Tissue response to mechanical vibrations for sonoelasticity imaging. Ultrasound Med. Biol. 16:241-246. Crossref |
||||
|
Rago T, Santini F, Scutari M, Pinchera A, Vitti P (2007). Elastography: New developments in ultrasound for predicting, malignancy in thyroid nodules. J. Clin. Endocrinol. 92:2917-2922. Crossref |
||||
|
Ran HT, Ye XP, Zheng YY, Zhan DZ, Wang ZG, Chen J, Madoff D, Gao J (2013). Spleen stiffness and splenoportal venous flow. J. Ultrasound Med. 32:221-228. Pubmed |
||||
|
Rivero-Juárez A, Morgaz J, Camacho A, Mu-oz-Rascón P, Domingues JM, Sánchez-Céspedes R, Torre-Cisneros J, Rivero A (2012). Liver stiffness using transient elastography is applicable to canine hepatic disease models. PLoS One 7:e41557. Crossref |
||||
|
Saftoiu A, Gheonea DI, Ciurea T (2007). Hue histogram analysis of the real-time elastography images for noninvasive assessment of liver fibrosis. Am. J. Roentgenol. 189:232-233. Crossref |
||||
|
Sarvazyan AP (1993). Shear acoustic properties of soft biological tissues in medical diagnostics. J. Acoust. Soc. Am. 93:23-29. Crossref |
||||
| Serejo F, Marinho R, Velosa J, Costa A, Moura MC (2007). Elastografia hepática transitória, um método não invasivo para avaliação da fibrose em doentes com hepatite C crônica [Transitory hepatic elastography: a non-invasive method to evaluate fibrosis in chronic HCV patients]. J. Port. Gastrenterol. 14:8-14. | ||||
|
Tan R, Xao Y, He Q (2010). Ultrasound elastography: it's potential role in assessment of cervical limphadenopathy. Acad. Radiol. 17:849-855. Crossref |
||||
|
Uchida H, Hirooca Y, Itoh A, Kawashima H, Hara K, Nonogaki K, Kasugai T, Ohno E, Ohmiya N, Niwa Y, Katano Y, Ishigami M, Goto H (2009). Feasibility of tissue elastography using transcutaneous ultrasonography for the diagnosis of pancreatic disease. Pancreas 38:17-22. Crossref |
||||
|
Vorländer CH, Wolff J, Saalabian S, Lienenlüke RH, Wahl RA (2010). Real time ultrasound elastography – a noninvasive diagnostic procedure for evaluating dominant thyroid nodules. Langenbecks Arch. Surg. 395:865-871. Crossref |
||||
|
White J, Gay J, Farnswoth R, Mickas M, Kim K, Matton J (2014). Ultrasound elastography of the liver, spleen and kidneys in clinically normal cats. Vet. Radiol. Ultrasound 55:428-434. Crossref |
||||
|
Zaleska-Dorobisz U, Kaczorowski K, Pawlus A, Puchalska A, Inglot M (2014). Ultrasound elastography – review of techniques and its clinical applications. Adv. Clin. Exp. Med. 23:645-655. Crossref |
||||
| Zhang YF, Liu C, Xu HX, Xu JM, Zhang J, Guo LH, Zheng SG, Liu LN, Xu XH (2014). Acustic radiation force impulse imaging: a new tool for the diagnosis of papillary thyroid microcalcinoma. Biomed. Res. Intl. 2014:416969. | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


