Full Length Research Paper
ABSTRACT
The female condom is a relatively new product that is intended to serve the dual role of protecting against unwanted pregnancy and sexually transmitted infections (STI). Very few studies have been conducted on the use of female condom in Nigeria. Therefore, information is lacking about its continued use, particularly among women at high risk of HIV and other STI. With the above consideration, the Society for Family Health conducted a quantitative and measuring access and performance (MAP) baseline survey to find out the population of women using a female condom to assess product availability and accessibility using pre-defined criteria for coverage, quality of coverage, access and equity of access in Edo, Delta and Lagos states of Nigeria. Data were entered and cleaned using SPSS 13.0. In general, the MAP study found that female condom suffers from lack of public awareness, limited patronage and stock-out; which may be due to absence of promotional efforts. To enable a successful acceptability of female condom in the Nigerian market, a comprehensive introductory and outreach programme needs to be developed. There is a need to consider the involvement of men, use of peer educators and service providers who might impact on an individual’s motivation to use the female condom.
Key words: Female condom, Nigeria, knowledge, quantitative method, measuring access and performance (MAP) study, Edo, Delta, Lagos.
INTRODUCTION
The female condom is a thin sheath or pouch worn by a woman during sexual intercourse. It lines the vagina entirely and helps to prevent pregnancy and sexually transmitted diseases including HIV. The female condom has been available in Europe since 1992 and was approved by the United States (US) Food and Drug Administration (FDA) in 1993. More than 10 years has elapsed since the female condom became widely available, and it remains the only female-initiated means of preventing both pregnancy and sexually transmitted infections (STIs), including HIV. The female condom was developed as an alternative to the male condom, and it was hailed as a method that would enable women to have greater control over their own protection from disease. It is available in many countries throughout the world, though in limited quantities. Different brands of female condom exist in different countries. In 2005, the producers of the female condom announced a new product called FC2. Large scale production of the FC2 began in 2007. The FC2 was approved by the FDA in December 2008 and the World Health Organisation has stated that the product is acceptable for bulk procurement by UN agencies.
In 2005, nearly two thirds of all female condoms were used in Africa, while the next largest shares went to North America and Europe. Asia accounted for less than 1% of the global total in 2005, though figures for latter years are higher due to population growth in India (UNFPA, 2005). With the support of the Joint United Nations Programme on HIV/AIDS (UNAIDS), public and private funders, and the manufacturer, more than 90 developing countries have introduced the method through public distribution, social marketing campaigns or commercial outlets. In several countries that have actively promoted its use, such as South Africa, Brazil, Ghana and Zimbabwe, steadily increasing female condom sales to the government suggest that effective programs can generate demand.
At the same time, there have been disappointments. Uptake in the West and in some developing countries has been lower than was initially anticipated, demonstrating that successful introduction will not be as straightforward as was hoped owing to significant structural and social barriers, including higher cost relative to the male condom and male partner resistance (Beksinska et al., 2001; Ford and Mathie, 1993). Recent comprehensive analysis of why the female condom has not reached its full potential attributed this primarily to lack of political will in the international policy arena rather than to lack of acceptability among users (Peter et al., 2010). A study by Kulczycki and colleagues published shows that the method is not popular among some women (Kaler, 2004a). Indeed, there are still gaps in knowledge about how acceptable the female condom is for long-term use and whether promoting it can help reduce STI rates (Kulczycki et al., 2004). Widespread promotion of the female condom has faced numerous social and political barriers an important backdrop for the individual choices that women make. In the United States, these barriers include ridicule of the female condom in the press, limited advertising and promotion, higher prices than those of the male condom, inadequate training of health care providers and limited distribution within the public health system.
Short-term acceptability studies consistently reveal insertion difficulties for some users (Cecil et al., 1998). Proportions of users finding the female condom difficult to insert are as large as 33 to 50% in some studies (Sapire, 1995; Ruminjo et al., 1996). Difficult insertion has been associated with less consistent use (Sly et al., 1997; Neiland et al., 2002). However, with practice and increased use, many of the insertion problems disappear (UNAIDS and WHO, 2000). Another barrier relates to negotiation with male partners. The female condom was designed to give women greater control over their own protection, without having to rely on their partners to use a condom. However, many studies confirm that partner cooperation is necessary for women to use the female condom successfully. Attitudes of men toward the female condom obtained indirectly from women's reports (Ray et al., 1995; Ruminjo et al., 1996) or directly from men (Bounds et al., 1992; El-Bassel et al., 1998; Hirkey et al., 2003; Seal et al., 1999) are generally positive. Men's positive attitudes and willingness to use the method may even enhance its acceptability to women (Hoffman et al., 2003).
Effective use of the female condom also depends on a variety of factors, including male involvement in the decision to use it. Several female condom studies have confirmed that male partner involvement and cooperation are essential for a successful use of the product (Francis-Chizororo and Natshalaga, 2003; Kaler, 2004b; Kerrigan et al, 2000; Preston-Whyte, 1995; Ray et al., 1995; Welbourne, 2006). It is surprising, therefore, that only a small number of female condom studies to date (Meekers and Richter, 2005; Penman-Aguilar et al., 2002; Witte et al., 2006) assessed men’s experiences directly. Men’s perspectives and experiences of female condom use can provide important insights into some of the key factors that impede facilitate female condom use. Programme planners and advocates now refer to the female condom as a female-initiated method, underscoring that the increased participation of men is important for its future success. Research has revealed that a man’s reaction to the female condom is often an important factor in determining whether his female partner uses the method or not (Welsh et al., 2001). A study in Zimbabwe found that, although women initiate the dialogue about using the method, both partners jointly decide to use it (Kerrigan et al., 2000). Furthermore, a study by Trivanhu et. al (2014), concluded that men have a role to play in its use and are willing to assist their partners use the method. Clearly, this means men have to be involved in female condom programming to raise their awareness as they influence female condom use greatly.
The benefits of expanding access to and use of female condom are considerable. A study in 2006 found that countrywide distribution (equivalent to 10% of condom sales) of the FC2 female condom in Brazil and South Africa would be “useful and cost-effective” in preventing HIV. The cost-savings could be greatly increased if 300 million FC2s were acquired through a global purchasing mechanism, which would cut the price per condom by two thirds (Dowdy et al., 2006). In FY 2008, the producers of the FC2 female condom sold 34.7 million units worldwide, up from 25.9 million in 2006 and 14 million in 2005 (The Female Health Company, 2008). Many of these condoms were purchased by donor agencies such as USAID and UNFPA. Altogether, female condoms account for only around 0.2% of global condom use.
It is understood that many persons still confuse female condom with the diaphragm. It was first distributed in Nigeria in the 90’s. The uptake of the product remains extremely low as a result of numerous socio-cultural, economic and programmatic factors. This is further confirmed that, Knowledge of the female condom among men and women study conducted by the health department of the federal government of Nigeria was as low as 13.4 and 20.6%, respectively (FMOH, 2005). Until now, the female condom was distributed on a limited scale as a ‘health product’ targeted at a narrow interest group mostly sex workers and women at government family planning clinics - at prices that were largely unaffordable. These, together with the low level of awareness on the benefits as well as absence of skills on proper usage have made the female condom one of the least accepted reproductive health methods in Nigeria. In addition, negotiating for safer sex in both spousal and non-spousal sexual encounters remains a major challenge for most women, as the male condom; despite its wide acceptability and availability may not always offer women the option of negotiating protected sex with their partners as use of the condom is still largely dependent on the men. According to the 2007 National HIV/AIDS and Reproductive Health Survey (NARHS), contraceptive prevalence rate (CPR) for modern family planning methods was 9.7%, while it was 13.4% for any method. These findings indicate that there is already an interest in family planning; therefore, wide sensitization, availability and affordability of the Female Condom (FC2) would widen the choices available for women and men. The current reproductive health environment in Nigeria provides the right milieu for a fresh start and it is expected that the project will leverage on these opportunities.
With the above consideration, the Society for Family Health conducted a quantitative and Measuring Access and Performance (MAP) baseline survey to find out the population of women using a female condom and to define and measure the coverage of the female condom in Edo, Delta and Lagos states. The Measuring Access and Performance (MAP) survey provides evidence for social marketing decision making. It allows programmers to make an assessment of product availability and accessibility using pre-defined criteria for coverage, quality of coverage, access and equity of access. Specifically, the study identified areas of poor coverage and estimated access in high risk areas. This information is vital for sales and marketing teams in prioritizing their efforts. In doing so, the performance of the social marketing programme will improve in terms of health impact, behaviour change, cost-effectiveness, equity and efficiency. Although MAP involves four stages of implementation, this baseline survey was limited and restricted to defining and measuring coverage of the female condom in only Edo, Delta, and Lagos states of Nigeria.
The study also sought information on any preference for female condom as an acceptable contraceptive method, knowledge and the attitudes of men and women towards the use of the female condom. Data from the baseline study assisted Senior-Friendly Hospital (SFH) in guiding the implementation of project activities towards attainment of project objectives. Data from the baseline study assisted SFH in guiding the implementation of project activities towards attainment of project objectives.
Another limitation of this study was the inability to include the health care providers perception about their thoughts and perceptions of the female condom, whether they actively promote it to clients and if these factors influence user acceptability and uptake.
DATA AND METHODS
Two types of studies; quantitative and Measuring Access and Performance were combined to obtain information on knowledge and coverage of female condom among men and women in Edo, Delta and Lagos states. The study locations were purposively selected based on the following reasons. Firstly, these states are associated with high population, contraceptive prevalence rates and high number of HIV infections.
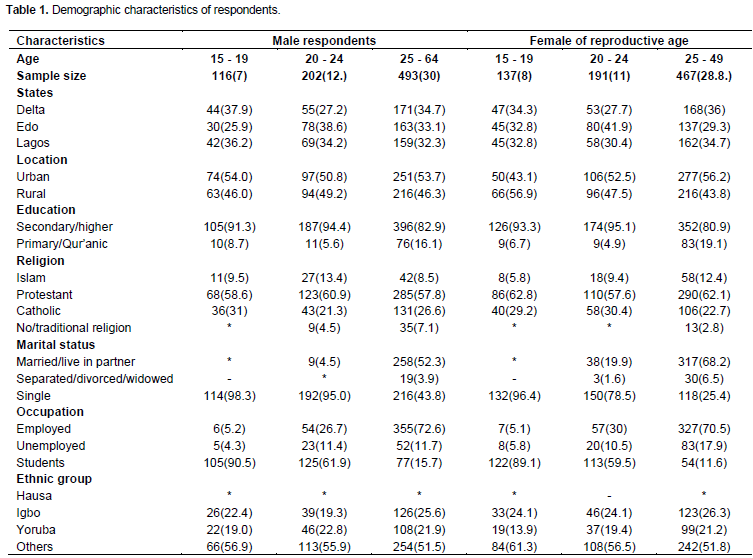
Quantitative research approach employed was in-home, face-to-face personal interview using a clustered stratified, multi stage random probability selection in other to achieve a representative sample in the study locations using and to give every eligible person equal probability of being selected for the interview. The structured quantitative method aimed at obtaining information on knowledge using a probability sampling selection process. A total of 60 enumeration areas were selected with proportional distribution across the rural and urban areas. Respondents for this study were 811 adult men (15-64 years) and 795 adult women (15 to 49 years).
For the MAP survey, 57 localities were selected based on probability proportional to size. Lists of localities were provided by the National Population Commission (NPC). Simple audit sheets were used for collecting formation on coverage and quality of coverage from the outlets in the selected 57 localities from the three states. The audit sheets were developed based on the information needed for calculating these indicators. Data collected through the audit sheets were processed in SPSS. They were cleaned and checked for completeness and appropriateness by generating initial frequency tables. During analysis, variables for coverage and quality of coverage were constructed. The interpretation of results was based on Lot Quality Assurance Sampling (LQAS) decision rule.
RESULTS AND DISCUSSION
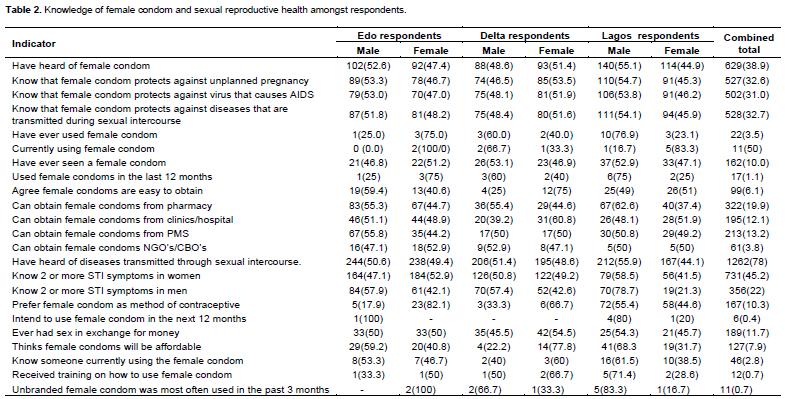
In general, findings on respondents’ knowledge about female condom and sexual reproductive health issues showed that knowledge about female condom is generally lower than average. Only about 4 in 10 (40%) of the respondents have heard of female condom. This varies considerably across the states and by gender. On the one hand, only about 33% knew that female condom can protect against an unplanned pregnancy. On the other hand, only 31% and about 33% knew that female condom can protect against virus that causes AIDS; and diseases that are transmitted during sexual intercourse respectively.
Findings on use of female condom were generally low and unimpressive. Out of all those who have heard of female condom only 3.5% of the respondents have ever used a female condom while information on intention to use is worrisome. Findings on respondents’ knowledge about female condom and sexual reproductive health issues showed that knowledge about female condom is generally lower than average. Only about 4 in 10 of the respondents have heard of female condom. This varies considerably across the states and by gender. On the one hand, only about 33% knew that female condom can protect against an unplanned pregnancy. On the other hand, only 31% and about 33% knew that female condom can protect against virus that causes AIDS; and diseases that are transmitted during sexual intercourse respectively. Results on use of female condom were generally low and unimpressive. Out of all those who have heard of female condom only 3.5% of the respondents have ever used a female condom while information on intention to use is worrisome (Table 1).
To effectively and objectively identify some determinants of use of female condom, we classified the determinants into a construct called opportunity, ability and motivation (OAM). Finding on the opportunity, ability and motivation constructs for female condom was disaggregated by gender. Scale items on these constructs were included in the survey questionnaire. The values for the items range from 1 (strongly agree) to 4 (strongly disagree). Reliability and validity of all items were investigated through Cronbach’s alpha index. This is to ascertain internal validity of the items for the constructs. The reliability scale of opportunity, availability and motivation construct was investigated through Cronbach’s alpha. The Cronbach’s alpha for opportunity construct that is, availability, brand appeal, quality of care and social norms are 0.66, 0.51, 0.60 and 0.78 respectively. The Cronbach’s alpha for ability construct, that is, social support, self-efficacy and knowledge are 0.74, 0.66 and 0.53, respectively. For motivation construct, that is, attitude, belief and outcome expectations are 0.66, 0.80 and 0.71 in that order. Under opportunity construct, availability and brand appeal’s bubbles were not significantly different between those that have heard of female condom and those that have not heard of female condom for both males and females. Considering quality of care about female condom, an adjusted mean of 2.53 among males that have heard of female condom was significantly higher than an adjusted mean of 2.48 among males that have not heard of female condom (p<0.05). Similarly for social norm, an adjusted mean of 2.52 among males that have heard of female condom was significantly higher than an adjusted mean of 2.36 for males that have not heard of a female condom. Considering opportunity construct for female analysis, findings were similar to that of male, though not significant.
Now turning attention to ability construct, self-efficacy and knowledge about female condom were significantly different between male respondents that have heard of female condom compared with those that have not heard of female condom (p < 0.05). However, social support on female condom was not statistically different between males that have heard of female condom compared with those that have not heard of female condom. Findings from the female analysis on ability construct showed that only knowledge about female condom was significantly different between female respondents that have ever heard of a female condom compared with those that have not heard of it (p < 0.05).
Issues on motivation construct that were included in the survey were: Attitude towards female condom, beliefs about female condom and outcome expectations. Generally, male and female respondents who have heard of female condoms have higher means than their counterparts who have never heard of female condom. For instance, female respondents who have heard of female condom have relatively higher means on attitudes about female condom, beliefs about female and outcome expectations compared with those who have not heard of it. This was statistically significant. The increased means on motivation construct was only significant for attitudes towards female condom (Table 2).
Coverage was low in Edo and Lagos states (35 and 45%) but above average in Delta State (55%). Quality of coverage was generally low in all the three states. None of the outlets visited displayed any promotional materials on female condom. Some of the few outlets that usually sell the product in the selected localities experienced stock-out even as at the time of the survey. Of all the outlets visited, only 45% product availability was reported in Delta State. Similar trends were also evident in Lagos State (35%), and Edo State (25%). In general, it is apparent that the product suffers from lack of public awareness, limited patronage and stock out; which may be due to absence of promotional efforts.
A benchmark price of thirty naira was set for Elegance female condom. This was only evident in a few outlets in Delta state who sold for less than $2. Prices of the product in Lagos and Edo States were above $2.
The degree for penetration for female condom was measured as the proportion of all the sales’ outlets visited, divided by the number that actually sells female condom in each of the states. The figures reported for each of the states was low with Edo having the lowest (3%), Lagos (4%), while Delta had 11% penetration. This finding clearly shows that female condom was hardly seen in these states, and buttressed the fact that its coverage was very low.
From the study, knowledge, availability and use of female condom was low and no campaigns and educational materials to promote it.
CONCLUSION AND RECOMMENDATIONS
From the study, knowledge, availability and use of female condom was low and no campaigns and educational materials to promote it. To enable a successful acceptability of female condom in the Nigerian market a comprehensive introductory and outreach programme needs to be developed. Therefore, there is need to consider the use of peer educators and service providers who might have a stronger impact on an individual’s motivation to use the female condom. Outreach workers could also be considered to solve initial difficulties in first experiences. Targeting men directly and educating them on the female condom and its correct use needs should be an urgent step. Also the many barriers to female condom use among men are not insurmountable as they are largely due to men’s limited familiarity with the method and to user related difficulties experienced by partners. These barriers can be overcome by targeting men directly for education of female condom and working jointly with couples around issues of safer sex communication and negotiation.
Female condom should primarily be made available through health facilities and drug outlets. It is therefore important that providers are properly trained to provide basic information for selling and recommending of the female condom. Providers should be encouraged to include female condom as a method of contraception during counseling of clients who require family planning services. It is therefore important that providers are properly trained on the need to provide basic information for selling and recommending of FC2. Providers should be told to include female condom as a method of contraception during counseling of clients who require family planning services. The survey clearly indicates the lack of media campaign on FC2 and the availability of FC2 in different brands because the few who were using female condom were using an unbranded type of female condom.
Findings from the MAP study revealed that coverage of the product was low in these states with Delta having the highest coverage compared with Lagos and Edo. Quality of coverage was also unimpressive. This clearly shows episodes of lack of promotional materials in all the outlets visited in the 57 localities across the three states coupled with stock outs. Furthermore, results also revealed low penetration of the product in each of the three states. This supports the evidence that coverage level of the product was poor across the three states in which the survey was conducted.
It is advisable to improve on coverage and the quality of coverage indicators for this product in the focal states. This can be done by making the product widely available, and through the development, production and deployment of promotional materials, to create and sustain public awareness and knowledge. This can instigate patronage for the product and further help to mitigate the incidence of stock-outs and grow penetration, and ultimately yield positive health outcomes. The female condom represents an important addition to the method mix, but awaits adequate empirically driven promotion and evaluation.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Beksinska ME, Rees VH, Mclyntre JA, Wilkinson D (2001). Acceptability of the female condom in different groups of women in South Africa- a multicentered study to inform the national female condom strategy. S. Afr. Med. J. 91(8):672-678. |
|
|
Cecil H, Perry MJ, Seal DW, Pinkerton SD (1998). The female condom: what we have learned thus far. AIDS Behav. 2(3):241-256. |
|
|
Dowdy DW, Sweat MD, Holtgrave DR (2006). Country-wide distribution of the Nitrile female condom (FC2) in Brazil and South Africa: a cost-effectiveness analysis. AIDS 20(16). |
|
|
Ford N, Mathie E (1993). The acceptability and experience of the female condom, Femidom, among family planning clinic attenders. Br. J. Fam. Plann. 19(2):187-192. |
|
|
Francis-Chizororo M, Natshalaga NR (2003). The female condom: Acceptability and perception among rural women in Zimbabwe. Afr. J. Reprod. Health 7:101-116. |
|
|
Hoffman S, Exner TM, Leu CS, Enrhardt AA, Stein Z (2003). Female condom use in a gender-specific family planning clinic trial. Am. J. Public Health. 93(11):1897-1903. |
|
|
Kaler A (2004). The female condom in North America: selling the technology of empowerment. J. Gend. Stud. 139(2):139-152. |
|
|
Kaler A (2004). The future of female-controlled barrier methods for HIV prevention: female condoms and lessons learned. Cult. Health Sex. 6(6):501-516. |
|
|
Kerrigan D, Mobley S, Rutenberg N, Fisher A, Weiss E (2000). The female condom: dynamics of use in urban Zimbabwe. Washington, DC: Horizons, Population Council. |
|
|
Kulczycki A, Kim DJ, Duerr A, Jamieson DJ, Macaluso M (2004). The acceptability of the female and male condom: a randomized crossover trial. Perspect. Sex. Reprod. Health 36(3):114-119. |
|
|
Preston-Whyte EM (1995). Bring us the female condom: HIV intervention, gender and political empowerment in 2 South African communities. Health Transit. Rev. 5(Suppl):209-222. |
|
|
Ray S, Basset M, Basset M, Maposhere C, Manangazira P, Nicolette JD, Machekano R, Moyo J (1995). Acceptability of the female condom in Zimbabwe: positive but male-centred responses. Reprod. Health Matters 3(5):68-79. |
|
|
Ruminjo JK, Steiner M, Joanis C, Mwathe EG, Thagana N (1996). Preliminary comparison of the polyurethane female condom with the latex male condom in Kenya. E. Afr. Med. J. 73(2):101-106. |
|
|
Sapire K (1995). The female condom (Femidom): a study of user acceptability. S. Afr. Med. J. 85(Suppl.10):S1081- S1084. |
|
|
Sly DF, Quandagno D, Harrison DF, Eberstein IW, Reihman K, Bailey M (1997). Factors associated with use of the female condom. Fam. Plann. Perspect. 29(4):181-184. |
|
|
The Female Health Company (2008). The Female Health Company Reports Record Results for Fiscal Year 2008, at High End of Guidance PR Newswire. Chicago, United States. |
|
|
Trivanhu C, Ancia M, Margret MK, Lynah M, Estelle M, Elizabeth M, Rumbidzai PC (2013). Level of Awareness and uptake of female condom in women aged 18 to 49 years in Bindura district, Mashonaland Central province Zimbabwe. J. AIDS Res. 13(1):75-80. |
|
|
UNFPA (2005). Donor Support for Contraceptives and Condoms for STI/HIV Prevention 2005. |
|
|
Welbourne A (2006). Sex, life and the female condom: Some views of HIV-positive women. Reprod. Health Matters 14:32-40. |
|
|
Welsh MJ, Feidblum PJ, Kuyoh MA, Mwarogo P, Kungu D (2001). Condom use during a community intervention trial in Kenya. Int. JSTD AIDS 12(7):469-474. |
|
|
UNAIDS, WHO (2000). The Female Condom: A Guide for Planning and Programming, Geneva: UNAIDS and WHO. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


