Full Length Research Paper

ABSTRACT
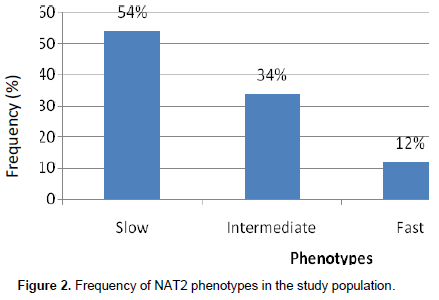
The human N-acetyltransferase II (NAT2) gene may vary between individuals resulting in variability in the incidence of adverse drug reactions. We set out in this adhoc analysis to determine the distribution of allele frequencies of NAT2 gene variants among children less than ten years treated with artemisinin-based combinations in Cameroon. Children with uncomplicated malaria were deparasitized with artemisinin based combination therapy (artesunate-amodiaquine, dihydroartemisinin-piperaquine and artemether-lumefantrine) and followed up for 42 days and adverse events recorded. Blood was spotted on filter paper prior to drug administration for DNA extraction by chelex method. Standard nested PCR followed by restriction enzyme analysis with KpnI, TaqI, and BamHI for detection of polymorphisms in the NAT2 was performed. Allelic frequencies and acetylator phenotypes were compared between participants with or without adverse drug events. The prevalence of slow, intermediate and fast acetylators was 54, 34 and 12% respectively. Significant clustering of mutant alleles (NAT2*5, NAT2*6 and NAT2*7) occurred among those who experienced skin rash and tiredness (OR = 5.765, P = 0.046) (OR = 13.280, P = 0.020). No significant difference was observed between fast and slow acetylators with respect to the development of other recorded adverse events. Overall, producers of the slow acetylator alleles were more likely to develop any adverse events (OR = 8.286, P = 0.017) during the study period. Mutant alleles of the wild type NAT2*4 associated with the slow acetylator phenotype were the most predominant NAT2 allelic type and individuals with the phenotype were more likely to develop adverse events to ACTs.
Key words: N-Acetyltransferase 2, Artemisinin based combination therapy, adverse events, slow acetylators, allele.
Abbreviation: NAT2, N-Acetyltransferase II; PCR, polymerase chain reaction; ACTs, artemisinin-based combinations therapies; ASAQ, artesunate-amodiaquine; WHO, world health organisation; CYP, cytochrome P450 enzymes; EDTA, ethylene diamine tetraacetic acid; DNA, deoxyribonucleic acid.INTRODUCTION
African countries on recommendation by WHO have increasingly adopted artemisinin-based combinations therapies (ACTs) as first line drugs against uncomplicated malaria. In Cameroon, artesunate-amodiaquine (ASAQ) was adopted as the first line drug against uncomplicated malaria in 2006. Amodiaquine an accompanying drug in these combinations has been associated with adverse drug reactions leading to reduced adherence to this drug (Adjei et al., 2009; AlKadi, 2007). In the light of increase in use of these ACTs, the science and activities relating to the detection, evaluation, understanding and prevention of adverse reactions to medicines or any other medicine-related problems is necessary for evaluating safety risks (WHO, 2002). Pharmacovigilance is important in the resource-constrained settings because patients may present different profiles of adverse events due to genetic, co-morbidity, and other drug interactions (Pirmohammed et al., 2007).
Drug action on the one hand, depends on how drugs are metabolized and how differences in activity of metabolizing enzymes could significantly contribute to the efficacy of these drugs (Ladero, 2008). Mutations in a gene coding for a drug metabolizing enzyme could result in an enzyme with normal, slow, or fast activity (Agundez, 2008). It has been demonstrated that only 30 to 60% of common drug therapy is successful and that adverse drug reactions could cause 7% of all hospital admissions, 4% of withdrawal from new medical entities, and this can cost society an amount equal to the cost of drug treatment itself (Agundez, 2008). The human N-acetyltransferase (NAT) is an expression product of a single intronless protein-coding exon which is 870 bp open reading frame located in chromosome 8p22 and encoding 290 amino acids. It is one of the important phase II drug metabolizing enzymes which catalyses the conjugation or N-acetylation of arylamine derived therapeutic drugs and carcinogenic compounds (Agundez, 2008). Two functional polymorphic variants of the NAT gene exist; the NAT I and NAT II (Sim et al., 2008). Genetic polymorphisms in the NAT2 locus influence individual variation in cancer susceptibility, responses to environmental toxins, and the effectiveness of prescribed medications (Ingelman-Sundberg, 2005; Lee et al., 2010). The NAT2 gene polymorphisms may vary between individuals and ethnicities and results in variability in the incidence of adverse drug reactions (Kang et al., 2009). Several single nucleotide polymorphisms (more than 15 point mutations) exist on the NAT2 gene that have given rise to at least 50 allelic variants today (Vatsis et al., 1995). A database for nomenclature of the growing number of different alleles or haplotypes of NAT polymorphisms exist (http://nat.mbg.duth.gr/). Polymorphisms in the wild type, (known as NAT2*4) give rise to combinations of 1-4 nucleotide substitutions in characteristic positions in the 870 bp coding sequence of the gene. Thus, wild type homozygotes are designated as NAT2*4/NAT2*4 made of two wild type alleles (Vatsis et al., 1995). It has been demonstrated that some single nucleotide polymorphisms (SNPs) in the NAT2 gene may cause structural protein changes or stability or reduced enzyme quantity (Sim et al., 2008; Walraven et al., 2008). Consequently, segregated gene variants in humans give rise to acetylation phenotypes classified as “rapid” (homozygotes of the NAT2*4 polymorphism), intermediate” (heterozygotes of the NAT2*4 polymorphism) and “slow” acetylation phenotypes (Boukouvala, 2005) (homozygotes of the mutant NAT2*5, NAT2*6, NAT 2*7 alleles) depending on the rate of enzyme activity (Chen et al., 2006; Chen et al., 2007). The effects of genetic polymorphism in the NAT2 gene on N-acetylation activity led to investigations of NAT2 SNPs as genetic markers for therapeutic response with resultant adverse reactions to drugs (Furet et al., 2002). Association studies have linked NAT2 polymorphisms and the acetylation status to individual differences in adverse events (Huang et al., 2002), as well as to development of bladder (Hein, 2002) and colon cancers (Garcia-Closas et al., 2005), rheumatoid arthritis (Kumagai et al., 2004) and systemic lupus erythematosus (Rychlik-Sych et al., 2006). The CYP2A6 and CYP2C8 genes are associated with the metabolism of ACTs. Several authors who analyzed the NAT2 gene also analyzed the CYP2A6 and CYP2C8 genes and have these to be correlated with predominantly slow metabolizers status (Gupta et al., 2013). This evidence indicates that when individuals are slow gene CYP2A6 and CYP2C8 they also present with the same “slow” phenotype for the NAT2 gene and could be at risk of developing adverse events. Achonduh et al. (2013), recently showed that NAT2 slow acetylators alleles clustered with individuals experiencing adverse to ASAQ in a study in the Northwest Cameroon. Therequencies of common NAT2 alleles were investigated to assess the distribution of these alleles among patients responding to ACTs in Cameroon. The aim of this study was thus to determine the genotypic frequencies of common NAT2 genotypes and investigate their association with adverse events in response to ACT treatment in children less 120 months in Cameroon.
MATERIALS AND METHODS
Study area
The study was conducted at two geographically distinct sites, that fall within two of the three major geo-ecological zones of Cameroon as described by MARA maps (Kleinschmidt et al., 2001) namely; Mutengene is situated at coordinates 04°01’N, 09°11’E. The climate is equatorial with a rainfall of 10,000 mm per annum and a temperature average of 25°C. The vegetation is semi-mangrove and tropical wet forest. The study site is limited to the south and south-east by the sea and to the north and north east by mount Cameroon, an active volcano that is 4,100 m above sea level. The population works predominantly on palm and rubber plantations or estates that are owned by the agro-industrial Cameroon Development Corporation (CDC).
Garoua is in the north of Cameroon and lies at the coordinates, 06°24’N, 10°46’E. Garoua serves as a river port in years when the rainfall is abundant. Situated in the river Benue basin, it receives an average annual rainfall of 380 mm. It has about 4 months of rainy season. The mean temperatures for most of the year are about 31oC and the vegetation is guinea-savannah. The population is predominantly of the Fula ethnic group and comprises of cattle grazers. A few have taken to trading in small provision merchandise with neighbouring Nigeria.
Screening and enrollment
Eligible children aged 6 to 120 months with acute uncomplicated falciparum malaria were screened at the outpatient department and informed consent obtained from parents or guardians. Patients meeting the inclusion criteria were randomized to trial allocation and pre-treatment investigations (clinical and laboratory assessments) conducted. Criteria for inclusion were; children of either gender, suffering from acute uncomplicated P. falciparum malaria confirmed by microscopy, or presenting with fever (axillary temperature ≥ 37.5°C) or having a history of fever in the preceding 24 h; ability to ingest tablets orally; willingness and ability to attend the clinic on stipulated follow-up days. A presentation was made of the anticipated risks and benefits, the discomfort to which the subjects were exposed, as well as the right to interrupt the participation at any time on their own free-will. A total of 696 patients were enrolled for the study and were registered into the three arms of the study at the 2 study sites.
ACT Administration and follow-up
Children were randomized to receive artesunate-amodiaquine, dihydroartemisinin-piperaquine and artemether-lumefantrine in the ratio of 2:2:1 respectively.. The first dose of the antimalarials was administered in the hospital and the rest of the tablets were administered at home, according to the prescription. The medication was administered with water after a meal. Follow up of children was ensured by community health workers (CHW) who visited participants daily in the first three days and reported any complaints from the mother. They also visited these mothers with complaints on other days besides the protocol stipulated days (D7, D14, D28, D35 and D42 after first dose). Adverse events following ingestion of the drugs were recorded on a case report form designed to capture these events. They included but were not limited to any signs and symptoms suggestive of malaria or toxicity, date of onset, duration of symptoms, severity of malaria or other treatment administered and patient outcome. Participants were followed up for 42 days post ACT-administration.
Sample collection and DNA extraction
Finger-prick blood was collected and spotted on filter paper at inclusion and during follow up on days D7, D14, D21, D28, D35& D42 for genomic. Blood spots on the filter paper were excised with a sterile pair of surgical scissors. DNA was extracted from the dried blood spots by bioling in Chelex-100 in buffered Tris-EDTA as previously described (Plowe et al., 1995). The DNA was stored in a Tris-EDTA buffer at -20°C until analysis and allelic discrimination analysis.
Genotyping single nucleotide polymorphisms in NAT2 gene
The most common alleles in Africa population were investigated. They contained following mutations: C481T (rs1799929, silent mutation, amino acid change L161L), G590A (rs1799930, amino acid change R197Q), A803G (rs1208, amino acid change K268R) and G857A (rs1799931, amino acid change G286E). The primers used to amplify the gene were: NAT2 (+) 5'-GCCTCAGGTGCCTTGCATTT-3' and NAT2 (-) 5'-CGTGAGGGTAGAGAGGATAT-3'. The amplification was carried out using a T3 thermal cycler (Biometra, UK). Each PCR cycle was performed in a total volume of 25 μl containing: nuclease free water, 10Xthermopol buffer, 10 mMdNTPs (200 μM of each deoxyribonucleotide), 20 pmol primer and 5 U/μL Taq polymerase and 3 ng of gDNA. After initial denaturation at 95°C for 5 min, 30 cycles of amplification were carried out with denaturation at 95°C for 50 s, annealing at 55°C for 50 s and extension at 72°C for 50 s, followed by a final extension at 72°C for 5 min. To confirm the presence of NAT2 alleles, PCR products were electrophoresed on a 2% agarose gel and polymorphisms determined by restriction endonuclease digestion of amplified gene fragments as described (Chen et al., 2007). The amplicons were digested under conditions stipulated for the restriction enzymes KpnI and BamHI (New England Biolabs, USA) (37°C for 16 h while Taq I digested at 65°C for 16 h). The digestion reaction was followed by inactivation at 80°C for 20 min. Digested and undigested fragments of each sample were electrophoresed on a 2% agarose gel stained with Ethidium Bromide and the pattern of migration analysed by UV trans-illumination. Different alleles and combinations of alleles of the NAT2 gene were determined for each sample according to the migration pattern and information indicated in Table 5.
Classification of acetylator genotype
NAT2 acetylator genotypes were produced according to previously published data (Yokogawa et al., 2001). Homozygotes (NAT2*4/NAT2*4) or heterozygotes (NAT2*4/NAT2*5, NAT2*4/NAT2*6 and NAT2*4/NAT2*7 combinations) for the dominant NAT2*4wildtype allele were classified as fast acetylator genotypes, while homozygotes of the mutant alleles (NAT2*5, NAT2*6 and NAT2*7) were classified as slow acetylator genotypes.
Data analysis
Data was entered on an SPSS version 16.0 (SPSS Inc., USA) statistical software. Frequency of the NAT2 allele and acetylator genotypes in the study population was performed. The association between NAT2 acetylator genotype and adverse events of ACTs in the study population was assessed by binary logistic regression analysis. The odd ratios (ORs) and 95% confidence interval (CIs) were also determined and a P-value < 0.05 was considered as statistically significant.
Ethical clearance
Ethical approval was obtained for the study from the National Ethics Committee for Health Research on human subjects in Cameroon and the Ethics Review Committee of the World Health Organisation (WHO-ERC).
RESULTS
Characteristics of study population
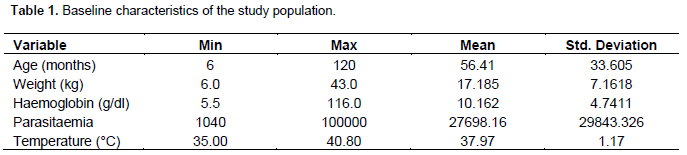
Of the 696 participants recruited in the study, the mean age was 56.41 months. Average hemoglobin was 10.162 g/dL and a geometric mean parasitaemia of 27698.16. The mean temperature was 37.97 with an average weight of 17.185 kg (Table 1).
Adverse reactions following ACTs administration and association with NAT2 alleles
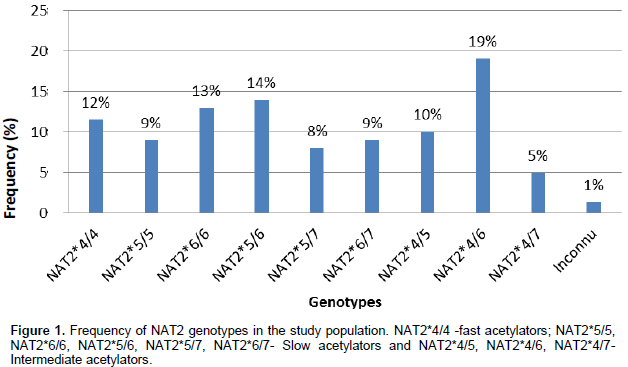
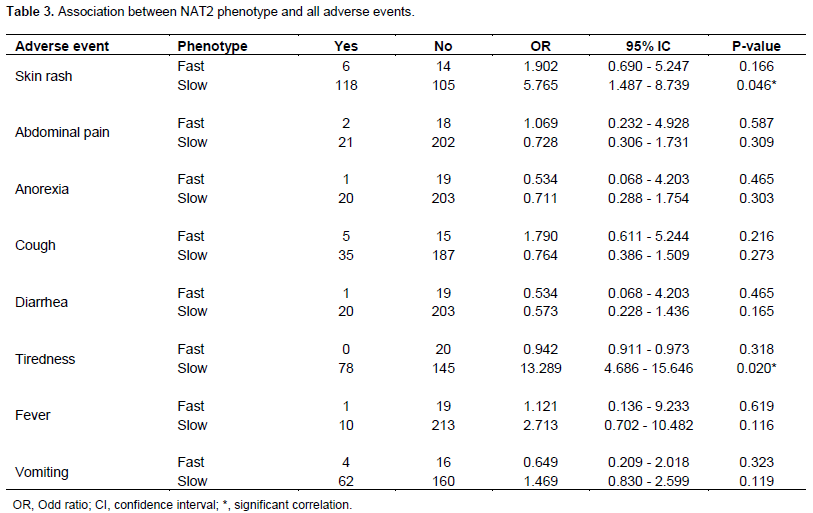
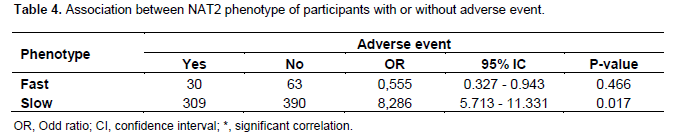
Adverse events reported during the study were asthenia, diarrhea, skin rash, anorexia, abdominal pain, cough, fever, tiredness and vomiting with severity ranging from mild to life-threatening. The causality of adverse events was ranged from no related to most probable with respect to test drug (Table 2). The frequencies of NAT2 genotypes and phenotypes in the study population are shown in Figures 1 and 2. Relative to fast acetylators, there was an association between NAT2 slow acetylators and susceptibility to develop skin rash (OR = 5.765, P = 0.046) and tiredness (OR = 13.280, P = 0.020) (Table 3). However, no significant difference was observed between fast and slow acetylators and the development of adverse events. Generally, slow acetylators were more likely (OR = 8.286, P = 0.017) to develop any of the adverse events compared to fast acetylators (Table 4).


DISCUSSION
Information gathered on the distribution of genetic polymorphism in populations is essential to understand population wide differences in response to treatment and disease risk. The profiles of the NAT2 genotypes/phenotypes in children less than 10 years were determined and their association with adverse reactions to ACTs as fixed dose combination following deparasitization analysed. Functional genetic polymorphisms of xenobiotic metabolizing enzymes have been associated with therapeutic response differences (Wilkinson, 2005) and disease risk susceptibility (Wilkinson, 2005; Nebert, 1997). In this study, it was observed that the slow acetylator phenotype was an independent risk factor for susceptibility (OR = 6.974, P = 0.017) to any adverse drug event, that is, asthenia, diarrhea, skin rash, anorexia, abdominal pain, cough, fever, tiredness and vomiting compared to those with fast acetylator phenotypes. This could be due to slow elimination of drugs from the system resulting in prolonged exposure and subsequent adverse events. Relative to other adverse events, tiredness and skin rash were observed to be significantly associated with slow acetylator phenotype. The question has been raised why African would preferentially maintain a mutation that places them at a disadvantage of adverse events during therapy. It is probable that over many centuries the pathophysiology allowed for minimal elimination of herbal drugs that accumulated in the body at sub-optimal concentration so that infections could be cleared by the presence of these active ingredients. Selectively the African population with slow metabolism is not exposed to drugs administered at high enough concentrations to usher in adverse events by preferential drug retention.
Results presented herein demonstrate a higher prevalence of NAT2 slow acetylators in this population with the like likelihood to develop adverse events. These findings indicate that NAT2 polymorphism may be considered a good genetic marker for safety assessment of inter-population differences when populations are exposed to drug such as when assessing the safety profile of newly developed drugs in phase 3 and 4 clinical trials in Africa.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ABBREVIATIONS
NAT2, N-Acetyltransferase II; PCR, polymerase chain reaction; ACTs, artemisinin-based combinations therapies; ASAQ, artesunate-amodiaquine; WHO, world health organisation; CYP, cytochrome P450 enzymes; EDTA, ethylene diamine tetraacetic acid; DNA, deoxyribonucleic acid.
REFERENCES
|
Achonduh OA, AtoghoTB, Mbulli IA, Chedjou JP, Achu M, Nji AM, Fokou E, Kamgue E, Veyee V, Karana O, Sahfe D, Mbacham WF (2013). Adverse events clustering with NAT2 slow metabolisers following deparasitization in children in Bangolan, NWR Cameroon. J. Life Sci. 7(7):742. |
|
|
Adjei GO, Goka BQ, Rodrigues OP, Høgberg LC, Alifrangis M, Kurtzhals JA (2009). Amodiaquine-associated adverse effects after inadvertent overdose and after a standard therapeutic dose. Ghana Med. J. 43(3):135-138. |
|
|
Agundez JA (2008). Polymorphisms of human N-acetyltransferases and cancer risk. Curr. Drug Metabol. 9(6):520-531. |
|
|
AlKadi HO (2007). Antimalarial drug toxicity: A review. Chemotherapy 53(6):385-391. |
|
|
Boukouvala BSE (2005). Structural analysis of the genes for human arylamine N-acetyltransferases and characterization of alternative transcripts. Basic Clin. Pharmacol. Toxicol. 96(5):343-351. |
|
|
Chen B, Zhang WX, Cai WM (2006). The influence of various genotypes on the metabolic activity of NAT2 in a Chinese population. Eur. J. Clin. Pharmacol. 62(5):355-359. |
|
|
Chen M, Xia B, Chen B, Guo Q, Li J, Ye M, Hu Z (2007). N-acetyltransferase 2 slow acetylator genotype associated with adverse effects of sulphasalazine in the treatment of inflammatory bowel disease. Can. J. Gastroenterol. 21(3):155-158. |
|
|
Furet Y, Bechtel Y, Le Guellec C, Bechtel PR, Autret-Leca E, Paintaud G (2002). Clinical relevance of N-acetyltransferase type 2 (NAT2) genetic polymorphism. Therapie 57(5):427-431. |
|
|
Garcia-Closas M, Malats N, Silverman D, Dosemeci M, Kogevinas M, Hein DW, Tardón A, Serra C, Carrato A, García-Closas R, Lloreta J (2005). NAT2 slow acetylation, GSTM1 null genotype, and risk of bladder cancer: results from the Spanish Bladder Cancer Study and meta-analyses. Lancet 366(9486):649-659. |
|
|
Gupta VH, Amarapurkar DN, Singh M, Sasi P, Joshi JM, Baijal R, Ramegowda PH, Amarapurkar AD, Joshi K, Wangikar PP (2013). Association of N-acetyltransferase 2 and cytochrome P450 2E1 gene polymorphisms with antituberculosis drug-induced hepatotoxicity in Western India. J. Gastroenterol. Hepatol. 28(8):1368-1374. |
|
|
Hein DW (2002). Molecular genetics and function of NAT1 and NAT2: role in aromatic amine metabolism and carcinogenesis. Mutat. Res. 506-507:65-77. |
|
|
Huang YS, Chern HD, Su WJ, Wu JC, Lai SL, Yang SY, Chang FY, Lee SD (2002). Polymorphism of the N-acetyltransferase 2 gene as a susceptibility risk factor for antituberculosis drug-induced hepatitis. Hepatology 35(4):883-889. |
|
|
Ingelman-Sundberg M (2005). Genetic polymorphisms of cytochrome P450 2D6 (CYP2D6): clinical consequences, evolutionary aspects and functional diversity. Pharmacogen. J. 5(1):6-13. |
|
|
Kang TS, Jin SK, Lee JE, Woo SW, Roh J (2009). Comparison of genetic polymorphisms of the NAT2 gene between Korean and four other ethnic groups. J. Clin. Pharm. Ther. 34(6):709-718. |
|
|
Kleinschmidt I, Omumbo J, Briet O, Van De Giesen N, Sogoba N, Mensah NK, Windmeijer P, Moussa M, Teuscher T (2001). An empirical malaria distribution map for West Africa. Trop. Med. Int. Health 6(10):779-786. |
|
|
Kumagai S, Komada F, Kita T, Morinobu A, Ozaki S, Ishida H, Sano H, Matsubara T, Okumura K (2004). N-acetyltransferase 2 genotype-related efficacy of sulfasalazine in patients with rheumatoid arthritis. Pharm. Res. 21(2):324-329. |
|
|
Ladero JM (2008). Influence of polymorphic N-acetyltransferases on non-malignant spontaneous disorders and on response to drugs. Curr. Drug Metabol. 9(6):532-537. |
|
|
Lee SW, Chung L, Huang HH, Chuang TY, Liou YH, Wu L (2010). NAT2 and CYP2E1 polymorphisms and susceptibility to first-line anti-tuberculosis drug-induced hepatitis. Int. J. Tuberc. Lung Dis. 14(5):622-626. |
|
|
Nebert DW (1997). Polymorphisms in drug-metabolizing enzymes: what is their clinical relevance and why do they exist. Am. J. Hum. Genet. 60(2):265-271. |
|
|
Pirmohammed MAK, Dodoo ANO, Winstanley P (2007). Pharmacovigilance in developing countries: Requires collaboration between stakeholders to develop novel models of funding. Br. Med. J. 335(7618):462-462. |
|
|
Plowe CV, Djimde A, Bouare M, Doumbo O, Wellems TE (1995). Pyrimethamine and proguanil resistance-conferring mutations in Plasmodium falciparum dihydrofolate reductase: polymerase chain reaction methods for surveillance in Africa. Am. J. Trop. Med. Hyg. 52(6):565-568. |
|
|
Rychlik-Sych M, Skrêtkowicz J, Gawro-ska-Szklarz B, Górnik W, Sysa-Jêdrzejowska A, Skrêtkowicz-Szarmach K (2006). Acetylation genotype and phenotype in patients with systemic lupus erythematosus. Pharmacol. Rep. 58(1):22-29. |
|
|
Sim E, Lack N, Wang CJ, Long H, Westwood I, Fullam E, Kawamura A (2008). Arylamine N-acetyltransferases: structural and functional implications of polymorphisms. Toxicology 254(3):170-183. |
|
|
Vatsis KP, Weber WW, Bell DA, Dupret JM, Evans DA, Grant DM, Hein DW, Lin HJ, Meyer UA, Relling MV, Sim E (1995). Nomenclature for N-acetyltransferases. Pharmacogenet Genomics 5(1):1-17. |
|
|
Walraven JM, Zang Y, Trent JO, Hein DW (2008). Structure/Function Evaluations of Single Nucleotide Polymorphisms in Human N-Acetyltransferase 2. Curr. Drug Metabol. 9(6):471-486. |
|
|
WHO (2002). The importance of pharmacovigilance: safety monitoring of medicinal products. In. Geneva. |
|
|
Wilkinson GR (2005). Drug metabolism and variability among patients in drug response. New Eng. J. Med. 352(21):2211-2221. |
|
|
Yokogawa K, Nakaharu T, Ishizaki J, Ozaki E, Takeda Y, Mabuchi H, Matsushita R, Kimura K, Nakashima E, Ichimura F, Miyamoto KI (2001). Kinetic phenotypic diagnosis of N-acetylation polymorphism in patients based on ratio of urinary metabolites of salicylazosulfapyridine. Int. J. Pharm. 229(1-2):183-191. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


