Full Length Research Paper

ABSTRACT
INTRODUCTION
METHODOLOGY
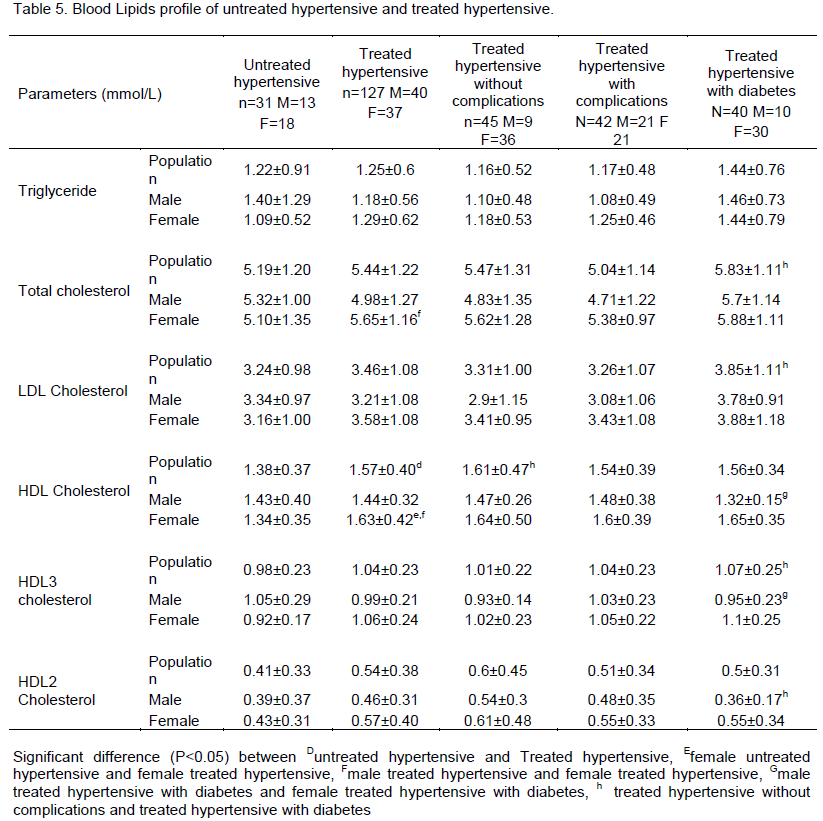
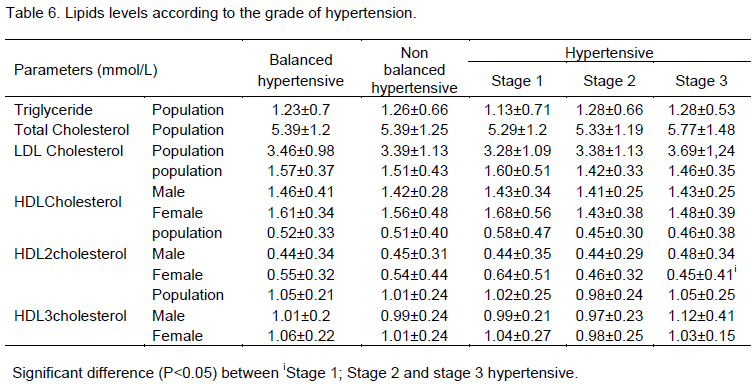
RESULTS
DISCUSSION
CONCLUSION
The HDL2C might be a better predictor of hypertensive complications if the relationship between its decreases with hypertensive stage of severity is confirmed by further studies.
CONFLICT OF INTERESTS
The authors did not declare any conflict of interest.
REFERENCES
|
Adamu UG, Okuku GA, Oladele CO, Abdullahi A, Oduh JI, Fasae AJ (2013). Serum lipid profile and correlates in newly presenting Nigerians with arterial hypertension. Vasc. Health Risk Manag. 9:763-768. |
|
|
|
|
|
Ai M, Otokozawa S, Asztalos BF, Ito Y, Nakajima K, White CC, Cupples LA, Wilson PW, Schaefer EJ (2010). Small dense LDL cholesterol and coronary heart disease: results from the Framingham Offspring Study. Clin Chem. 56(6):967-76. |
|
|
|
|
|
Andrew JK, Clifford JB (1994). Type 2 diabetes. London: Royal Society of Medicine Press. p. 107 |
|
|
|
|
|
Bakogianni MC, Kalofoutis CA, Skenderi KI, Kalofoutis AT (2001). Clinical evaluation of plasma high-density lipoprotein subfractions (HDL2, HDL3) in non-insulin dependent diabetics with coronary disease. J. Diabetes Complications 15(5):265-269. |
|
|
|
|
|
Cai L, Zhang L, Liu A, Li S, Wang P (2012). Prevalence, awareness, treatment, and control of dyslipidemia among adults in Beijing, China. J. Atheroscler. Thromb. 19:159-168. |
|
|
|
|
|
Dobiasova M, Stribrna J, Pritchard P, Frohlich J (1992). Cholesterol esterification rate in plasma depleted of very low and low density lipoprotein is controlled by the proportion of HDL2 and HDL3 subclasses: study in hypertensive and normal middle aged and septuagenarian men. J. Lipid Res. 33:1411-1418. |
|
|
|
|
|
DurakoÄŸlugil ME, Ayaz T, Kocaman SA, KırbaÅŸ A, DurakoÄŸlugil T, ErdoÄŸan T, Çetin M, Åžahin OZ, Çiçek Y (2014).The relationship of plasma catestatin concentrations with metabolic and vascular parameters in untreated hypertensive patients: Influence on high-density lipoprotein cholesterol. Anadolu Kardiyol Derg. 2014 Jul 17. |
|
|
|
|
|
Freedman DS, Otvos JD, Jeyarajah EJ, Shalaurova I, Cupples LA, Parise H, et al (2004). Sex and age differences in lipoprotein subclasses measured by nuclear magnetic resonance spectroscopy: the Framingham Study. Clin Chem. 50:1189-1200. |
|
|
|
|
|
Hirano T, Nohtomi K, Koba S, Muroi A, Ito Y (2008). A simple and precise method for measuring HDL-cholesterol subfractions by a single precipitation followed by homogenous HDL-cholesterol assay. J. Lipid Res. 49(5):1130-1136. |
|
|
|
|
|
Iaccarino G, Trimarco V, Lanni F, Cipolletta E, Izzo R, Arcucci O, De Luca N and Di Renzo G (2005). β-Blockade and increased dyslipidemia in patients bearing Glu27 variant of β2 adrenergic receptor gene. Pharmacogenomics J. 5:292-297 |
|
|
|
|
|
Joy T and Hegele RA (2008). Is raising HDL a futile strategy for atheroprotection? Nat. Rev. Drug Discov. 7:143-155. |
|
|
|
|
|
Kanaya AM, Vittinghoff E, Shlipak MG, Resnick HE, Visser M, Grady D, Barrett-Connor E (2003). Association of total and central obesity with mortality in postmenopausal women with coronary heart disease. Am. J. Epidemiol.158:1161-1170. |
|
|
|
|
|
Maeda S, Nakanishi S, Yoneda M, Awaya T, Yamane K, Hirano T, Kohno N (2012). Associations between Small Dense LDL, HDL Subfractions (HDL2, HDL3) and Risk of Atherosclerosis in Japanese-Americans. J. Atheroscler. Thromb. 19(5):444-52 |
|
|
|
|
|
McPherson R, Frohlich J, Fodor G, Genest J (2006). Canadian Cardiovascular Society position statement †Recommendations for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease. Can. J. Cardiol. 22:913â€27. |
|
|
|
|
|
Moriyama K, Negami M, Takahashi E (2014). HDL2-cholesterol/HDL3-cholesterol ratio was associated with insulin resistance, high-molecular-weight adiponectin and components for metabolic syndrome in Japanese Diabetes. Res. Clin. Pract. 106(2):360-365. |
|
|
|
|
|
Okeahialam BN, Osunkwo A, Isichei CO (2008). Artherogenic burden of hypertensive, diabetic and hypertensive – diabetic patients seen in Jos. J. Med. Trop. 5:50-55. |
|
|
|
|
|
Saidu H, Karaye KM, Okeahialam BN (2014). Plasma lipid profile in Nigerians with high--normal blood pressure. BMC Res. Notes 7:930. |
|
|
|
|
|
Shuhei N, Söderlund S, Jauhiainen M, Taskinen MR (2010). Effect of HDL composition and particle size on the resistance of HDL to the oxidation. Lipids Health Dis. 9(1):104-114. |
|
|
|
|
|
Skoczyńska A, Wojakowska A, Turczyn B, Zatońska K, Wołyniec M, Regulska-Ilow B, Ilow R, Szuba A, Zatoński W (2013). Lipid pattern in middle-aged inhabitants of the Lower Silesian region of Poland. The PURE Poland sub-study. Ann. Agric. Environ. Med. 20(2):317-24 |
|
|
|
|
|
Srisawasdi P, Chaloeysup S, Teerajetgul Y, Pocathikorn A, Sukasem C, Vanavanan S, Kroll MH (2011). Estimation of plasma small dense LDL cholesterol from classic lipid measures. Am. J. Clin. Pathol. 136(1):20-9. |
|
|
|
|
|
Stone NJ, Bilek S, Rosenbaum S.Strona NCEPT ATP III (2005). Recent National Cholesterol Education Program Adult Treatment Panel III update: adjustments and options. Am. J. Cardiol. 96(4A): 53E-59E. |
|
|
|
|
|
Sun GZ, Li Z, Guo L, Zhou Y, Yang HM, Sun YX (2014). High prevalence of dyslipidemia and associated risk factors among rural Chinese adults. Lipids Health Dis.13(1):189. |
|
|
|
|
|
Superko HR (2009). Advanced Lipoprotein Testing and Subfractionation are Clinically Useful. Circulation 119:2383-2395. |
|
|
|
|
|
Szollár LG, Mészáros I, Tornóci L, Rischák K, Molnár M, Mányai S (1990). Effect of metoprolol and pindolol monotherapy on plasma lipid and lipoprotein-cholesterol levels (including the HDL subclasses) in mild hypertensive males and females. J. Cardiovasc. Pharmacol. 15(6):911-917. |
|
|
|
|
|
Thalameh Y, Wei R, Naito H (1986). Measurement of HDL HDL2, and HDL3 by HDL3 by dextran sulfate –MgCl2 precipitation technique in human serum. Clin. Chim. Acta 158:33-41. |
|
|
|
|
|
Van Linthout S, Spillmann F, Schultheiss HP; Tschope, C (2010). High-density lipoprotein at the interface of type 2 diabetes mellitus and cardiovascular disorders. Curr. Pharm. Des. 16(13):1504-1516. |
|
|
|
|
|
Vassault A, Grafmeyer D, de Graeve J, Cohen R, Beaudonnet A, Bienvenu J (1999). Analyse de biologie médicale : spécification et normes d'acceptabilité à l'usage de la validation de techniques. Ann. Biol. Clin.57: 685-95. |
|
|
|
|
|
Wang B, Wei D, Wang C, Zhang J, Pan L, Ma M, Xue F, Wu Z, Shan G (2012). Prevalence of dyslipidemia and associated factors in the Yi farmers and migrants of Southwestern China. Atherosclerosis 223:512-518. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


