There is a rising concern for the rapid increase of COVID-19 confirmed cases in Kandahar province. From zero reported cases until 17th March 2020, then Kandahar saw a sudden rise in the cases by 16th May 2020. Decreased literacy rates, poor health education, lack of facilities, inconsistent government policies, and defying coronavirus safety advisory by the public have resulted in the rapid spread of COVID-19. The awareness and practices of the people towards the COVID-19 were significantly low. Therefore, the risk of coronavirus in Kandahar province is extremely high due to the aforementioned reasons. To overcome this virus, the local government must declare strict measures and provide the public with information about the severity and prevention mechanisms of this fatal disease. Mass and random diagnostic testing are required to track the actual infection rates, which can give a realistic picture of what is occurring. In this article, the current situation of COVID-19, available medical facilities, and public response to the ongoing pandemic in Kandahar, Afghanistan was highlighted.
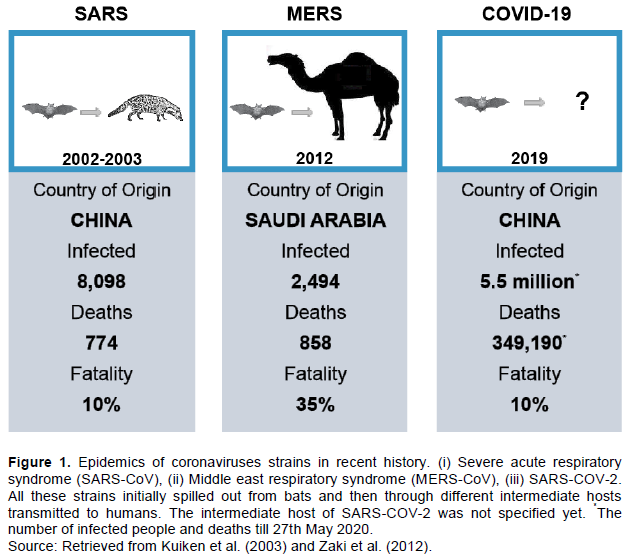
Coronaviruses are a large group of single-stranded, non-segmented, positive-sense RNA viruses belonging to the family Coronaviridae (Cui et al., 2019; Wege and Ter Meulen, 1982). Members of this family cause respiratory and gastrointestinal infections in humans and animals (Perlman, 1998). In the past two decades, two well-known pathogenic strains of coronaviruses, e.g. SARS-CoV and MERS-CoV, have emerged in humans (Kuiken et al., 2003; Zaki et al., 2012). The newly appeared novel type coronavirus (2019-nCoV or SARS-COV-2), is the third infectious strain of the coronaviruses (Zhu et al., 2020) (Figure 1). Genomic sequence analysis of SARS- COV-2 coronavirus showed 80% identity to SARS and 50% to MERS (Lu et al., 2020; Ren et al., 2020). The novel coronavirus is likely to be harbored by bats (Andersen et al., 2020; Lu et al., 2020; Wan et al., 2020; Zhou et al., 2020) and transmitted to humans through an unknown intermediate animal in Wuhan, Hubei province, China in late December 2019 (Surveillances, 2020; Wang et al., 2020), and spread rapidly throughout the world causing a global pandemic. At the time of writing, over 5.5 million people have been infected, and 349,190 deaths have been reported worldwide (WHO, 2019). To date, no approved vaccine or antiviral drug has been found to fight against this disease. Prevention measures, including social distancing, self-isolation, lockdown, and quarantine are certain guidelines that have helped in the prevention of COVID-19 spread. The knowledge about SARS-COV-2 is evolving rapidly because scientists around the globe continue to study molecular, functional, and structural approaches in the light of international cooperation for the development of vaccines.

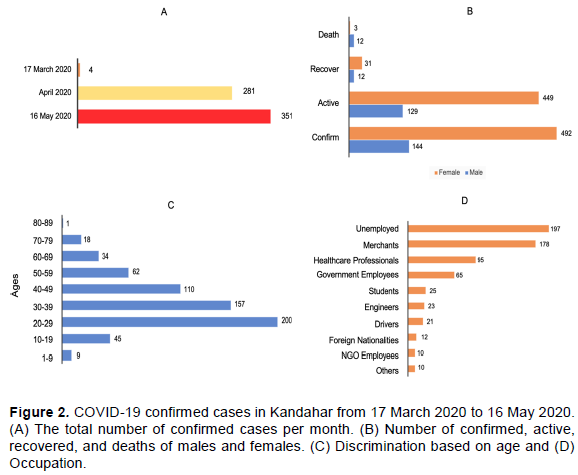
The COVID-19 pandemic reached Afghanistan on the 24th of February, 2020, when the first confirmed case was reported in Herat, a province that borders Iran, one of the major hubs of COVID-19 associated mortality. The pandemic has since spread throughout the 34 provinces of Afghanistan; however, three provinces (Kabul, Herat, and Kandahar) contain higher numbers of confirmed cases, respectively (Figure 2). We conducted this short study to pinpoint the current situation of COVID-19 and the behavior of the public to this pathogenic disease in Kandahar province, home to 3 million people and the second-largest city in the south of Afghanistan.
Two types of study designs were used in this study, that is, retrospective study to collect the data of 636 COVID-19 confirmed cases. In contrast, a cross-sectional study was conducted to interview 250 randomly selected residents of Kandahar city. The initial data regarding COVID-19 cases in Kandahar province was obtained from the database of the office of National Disease Surveillance and Response (NDSR), Directorate of Public Health (DoPH), Kandahar Province, Afghanistan. Inclusion criteria were all the patients who were PCR positive for COVID-19. Patients with only positive rapid tests were excluded from the study. The response and practices of the public towards the novel COVID-19 were determined through a questionnaire method. In this part of the study, inclusion criteria were residents of Kandahar city and willing to take part in this study. We collected the opinions of 250 randomly selected participants who volunteered to be interviewed. Consent was taken from all the participants before the interview. The surveillance system is not good in Afghanistan. Most of the cases are missed due to the limited number of tests available, as well as poor tracking of COVID-19 cases. The duration of the study was two months (17th March 2020 to 16th May 2020).
Current situation of COVID-19 in Kandahar
The first positive COVID-19 case was reported in Kandahar province on 17 March 2020, when a doctor tested positive upon returning from Pakistan, which shares a border with Kandahar. Within a few weeks (16 May), the total confirmed numbers increased exponentially to 636. Included in this numbers, 95 were healthcare professionals (Doctors, Nurses, Technicians, and Midwives), reflecting that they have not followed standardized safety guidelines as stated in Jin et al. (2020). Since they are in close contact with the public, they might have inadvertently spread the virus to patients, other staff, and family members. Surprisingly, a total of 50 confirmed COVID-19 patients have vanished after the first diagnosis, which is a serious threat to the whole community as health authorities are unable to complete contact tracing. However, as of 16th May 2020, a total of 2,063 suspected samples had been tested, and 636 (36.80%) were positive, 492 (77.2%) were male, and 144 (22.8%) were female, 578 (90.9%) active cases, 43 (6.8%) recovered, and 15 (2.4%) deaths have recorded. The majority of those who tested positive were aged between 20 and 29 years. Additional details of COVID-19 patients are shown in Figure 2.
In response to cope with this virus, the local government did not react as quickly or with strong restrictions as the response observed in countries such as Italy or China. This can be attributed to low incomes, food insecurity, and the social structure in Kandahar, where many people in the community are already struggling with low wages and daily work. Once the pandemic was fueled across the country, therefore in the mid-April 2020, the local authorities took initial measures including: (i) Kandahar city was placed under partial lockdown but without any restrictions on entry and exit. During day time, a big portion of the city was in quarantine except for medicals, dairy products shops, and bakery. The markets and shops were scheduled to remain open from 12:00 to 6:00 am to try to reduce the number of crowds gathering at the same time. (ii) All educational institutions were suspended. (iii) Various campaigns were launched throughout the province to increase awareness among the public. However, in the arrival of Muslims holy month (Ramadhan) on 22nd April 2020, the lockdown time was rescheduled from 5:00 am to 4:00 pm, so all the shops were opened in day hours, but during night time the city was in quarantine. With all these efforts, major lapses were seen at every step, ranging from inconsistent government policies, avoiding health advisory by public populations, and lack of awareness resulted in the rapid spread of the pandemic in Kandahar province. Based on such observations, it could be predicted that the number of confirmed cases will continue to rise rapidly in the coming weeks/months.
Medical facilities
The local government designated a newly built government hospital (Ainomina Hospital) with 350 bed capacity as the COVID-19 response facility where patients who were suspected or confirmed could be isolated; this is the only isolation and healing center in the province. The Ministry of Public Health along with other international health donor agencies such as International Committee of the Red Cross (ICRC), World Health Organization (WHO), UNICEF, and Afghan Red Crescent assisted in providing crucial supplies such as N95 masks, personal protective equipment (PPE), cleaning materials and other necessary health items to protect the healthcare professionals at the front line of pandemic battle.
Initially, Ainomina Hospital lacked COVID-19 diagnostic facilities; the suspected samples were sent to the Central Reference Laboratory at the Ministry of Public Health (MoPH) located in Kabul, the capital of Afghanistan. This whole process took almost a week to determine whether someone is infected or not. Fortunately, in early April 2020, the DoPH received diagnostic kits from MoPH, and Ainomina Hospital was given the kits to complete testing on patients who were suspected of COVID-19. Until 16th of May 2020, a total of 2,063 suspected people have visited this hospital for testing to confirm their diagnosis. The hospitalized patients were given supportive therapy, such as analgesics, antipyretics, and oxygen therapy. The recovered patients were discharged from the hospital once they were afebrile for three days and had tested negative twice for COVID-19. Infection prevention measures were put in place to ensure all the rooms where positive patients had been admitted were decontaminated with 0.5% chlorine.
Public response to COVID-19 outcome
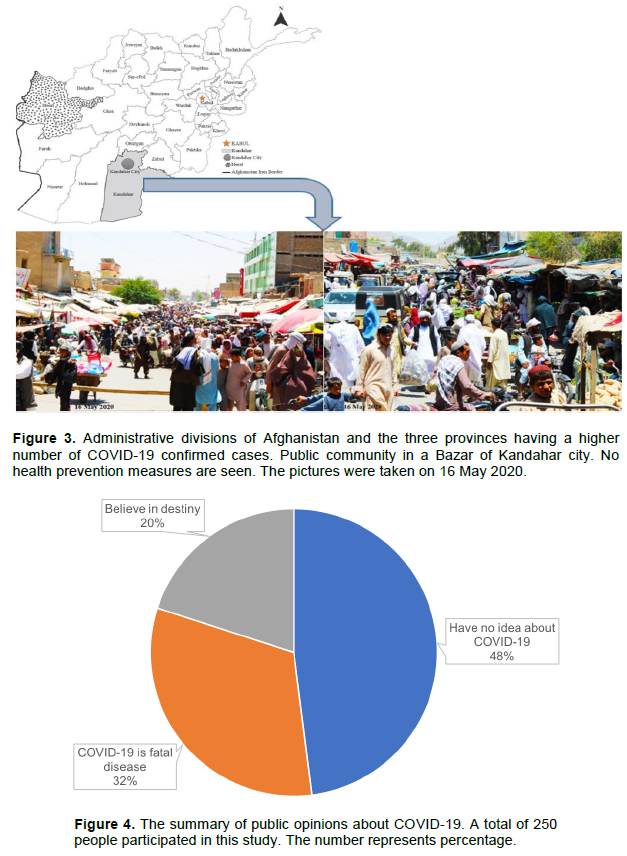
The initial response in the community to the threat of COVID-19 was apathetic. Despite the risk of the health emergency, the public has been reluctant to cooperate with government calls and have violated or ignored the request for lockdown in the community to try to halt the transmission of the virus. The global slogan “social distancing” was wholly ignored in this part of the world. Throughout the province during the lockdown period, regardless of the time of day, a large-scale gathering of people continued with no concern around health safety measures such as shopping in crowded areas (Figure 3), attending large wedding parties, picnics, and funerals. Such activities for sure can exacerbate the spread of COVID-19. From our short and random interview with people, we found that the public ignored safety restrictions mainly for the following reasons: (i) the majority of the people interviewed had very little knowledge about COVID-19 due to poor educational literacy. They were unwilling to accept this pandemic as a serious risk to their health but rather consider it as a rumor. (ii) A portion of the participants-based response on religious beliefs where they think death is predetermined already, and they will die on specific time as written in destiny. Hence, there is no need for social distance or take any other health safety measures. (iii) We also found very few people in a cluster of our study participants who accepted COVID-19 as a potentially lethal virus and follow all the health and safety measures that are recommended (Figure 4).
There are many reasons why the COVID-19 cases in Kandahar continue to rise rapidly; they include the community not maintaining social distancing or taking health measures such as using masks and gloves. Therefore, the local government and all other relevant authorities should be well prepared for the worst situation in the coming months. Although it is still not late, comprehensive measures like strict curfew to reduce person to person transmission of this virus are required to slow down the further spread of the disease. Efforts should be made against the spread of this pandemic, and there should be plans implemented with local authorities and international health donors under one platform. A strict curfew has shown to work in some countries, but the community should be educated on how to keep themselves safe to reduce transmission. However, if curfew cannot be implemented due to some reasons, at least other preventive measures, like wearing masks and gloves, should be made complimentary for the people. Public services’ offices, banks, hospitals, and all other places with mass gathering should be sprayed and provided with disinfectants regularly.
The diagnostic testing capacity was low; in the last three months, around 2,000 samples have been tested which is not enough for the population at risk among nearly 3 million residents of Kandahar, a large number of diagnostic kits and qualified technicians are required to conduct mass screening to track the actual infection rates
front line of battle against COVID-19. For public awareness, the best option that government can use to avoid further disaster is to get the help of religious scholars since our society is very much religious-based and scholars have special influence among ordinary people. They can convey health alert messages better than anyone else throughout the province. Lastly, in the current study there were limitations in retrospective study type and higher illiteracy rate of the majority of the interweaved individuals.
The authors have not declared any conflict of interests.
The authors thank the staff in the National Disease Surveillance and Response (NDSR), Directorate of Public Health (DoPH) of Kandahar province, for providing the primary data.