Full Length Research Paper

ABSTRACT
We described the antimicrobial susceptibility pattern of pathogenic bacteria causing urinary tract infections among males with lower urinary tract obstruction (LUTO) at the Komfo Anokye Teaching Hospital (KATH), Kumasi, Ghana. Between January and December 2009, a cross sectional hospital based study was conducted for 102 subjects. Patients presenting with symptoms of LUTO and who were on short admission (at most 48 h) at the accident and emergency unit of KATH were identified as potential study subjects. All the patients presented with acute retention of urine at the emergency unit of KATH and urethral catheterization was attempted to relieve them of the retention under sterile conditions. Urine specimen were collected into sterile urine containers immediately after the catheterization (irrespective of type) and sent to the microbiology laboratory at KATH for routine examination, culture and antimicrobial sensitivity testing. The mean age for males with LUTO was 62 years (Range: 2-93 years). The overall prevalence of pathogens was highest among the >70 years age group (40.2%). Whilst Klebsiella spp. (43.5%) and Pseudomonas spp. (50.0%) were the most predominant species within the >70 years age group, Escherichia coli (45.3%) and Staphylococcus aureus (57.1%) were the most predominant species within the <50 and 50-70 age groups. With respect to antibiotic sensitivity, Salmonella spp. showed the highest susceptibility rate of 15.8% whilst Klebsiella spp. was the least susceptible (9.2%) to antimicrobial agents used. The highest and least multi-drug susceptible bacterial isolates were E. coli and Citrobacter freundii respectively. This study’s results indicate that antibiotics commonly used in UTIs are still effective, but species distribution and their susceptibility to antibiotics are changing. The caution therefore is that antimicrobial susceptibility testing needs to be done to help select the appropriate antibiotic for effective treatment of diseases.
Key words: Antibiotic, asymptomatic, bacteriuria, acute, cystitis, urosepsis, catheter, antimicrobial susceptibility.
INTRODUCTION
Antimicrobial resistance (AMR) is resistance of a micro-organism to an antimicrobial compound. Resistant organ-isms including bacteria, fungi, viruses and some parasites are able to withstand attack by antimicrobial compounds, such as antibiotics, antifungals, antivirals and antimalarials, so that standard treatments become ineffective and infections persist increasing risk of spread to others. The evolution of resistant strains is a natural phenomenon that happens when microorganisms are exposed to antimicrobial drugs, and resistant traits can be exchanged between certain types of bacteria. The misuse of antimicrobial medicines and poor infection control practices accelerates this natural phenomenon. Many of the drug treatment breakthroughs of the last century could be lost through the spread of antimicrobial resistance. As a result, many infectious diseases may one day become uncontrollable and could rapidly spread throughout the world (Bhullar et al., 2012; WHO, 2012).
Infections caused by resistant microorganisms often fail to respond to the standard treatment, resulting in prolonged illness and greater risk of death. The death rate for patients with serious infections caused by resistant pathogens is about twice that in patients with infections caused by non-resistant bacteria (WHO, 2012). New resistance mechanisms, such as enzymes produced by the bacteria that destroy last generation antibiotics, have emerged among several Gram-negative bacilli and have rapidly spread among many countries. This can render ineffective powerful antibiotics, which are often the last defense against multi-resistant strains of bacteria. This new resistant mechanism is encountered in ordinary human pathogens (for example, E. coli) that cause common infections such as urinary tract infection (Bhullar et al., 2012; Kuo, 1999).
Lower urinary tract obstruction (LUTO) and urinary tract infections (UTIs), bladder cancer, incontinence, etc. are more common in elderly patients. UTI is currently one of the most common type of bacterial infection in humans. It involves any part of the urinary system, including urethra, bladder, ureters and kidney. It has been reported that about 150 million people around the globe are diagnosed each year with UTI and this cost in excess of six billion dollars (Gupta et al., 2001). UTI is mostly caused by bacteria though viruses and fungi are rare aetiologic agents (Griebling, 2007). Gram negative bacteria such as Escherichia coli, Klebsiella spp., Pseudomonas spp., Proteus spp., Neisseria gonorrhoea etc are usually the predominant causative agents of UTI (Al Sweih et al., 2008). However, other non-Gram negative bacteria such as Staphylococcus spp., Streptococcus spp., Chlamydia trachomatis, etc. have also been identified as causative agents (Griebling, 2007). The emergence of antibiotic resistance in the management of UTI is a serious public health concern, particularly in the developing world where apart from high level of poverty, ignorance and poor hygienic practices, there is also high prevalence of fake and spurious drugs of questionable quality in circulation (Abubakar, 2009).
This study was conducted to determine the etiological agents of UTI in men presenting with LUTO at KATH and their antimicrobial susceptibility and resistance patterns.
MATERIALS AND METHODS
Subjects
This was a cross-sectional hospital based study conducted for 102 subjects between January and December 2009. Patients with symptoms of LUTO or who had acute urine retention and were on short admission (up to 48 hours) at the Accident and Emergency Unit (AEU) of KATH were identified as potential study subjects. Prior to the study, ethical approval was sought from the Kwame Nkrumah University of Science and Technology (KNUST) School of Medical Sciences (SMS)/KATH Committee on Human Research Publications and Ethics (CHRPE). The participation of the respondents was voluntary and informed consent was obtained from each participant.
Inclusion and exclusion criteria
All patients admitted to the AEU with acute urine retention received urethral catheterization to relieve them of the retention under sterile conditions. Suprapubic Cystostomy (SPC) was done for a number of patients whose initial urethral catheterization failed. Urine specimen for routine examination, culture and sensitivity tests was collected into sterile urine containers immediately after the catheterization (irrespective of type). Subjects whose urinalysis revealed pyuria and positive urine culture and who had voluntarily agreed to participate in the study were enrolled. Subjects whose urine culture had multiple bacteria growth were considered to be contaminants and were excluded from the study.
Specimen collection
The importance of clean catch urine specimen was explained to consented study subjects. 10 ml of urine was collected from study subjects for routine examination, culture and sensitivity tests. The urine specimens were collected from the distal end of the catheter immediately after the catheterization (irrespective of type) into sterile urine containers.
Specimen processing
Collected urine specimens were transported immediately (within 30 min after collection) to the microbiology laboratory of KATH for routine examination, culture and sensitivity testing. Samples were processed within 30 min of arrival into the laboratory. Specimens were initially processed appropriately for culture and sensitivity before the routine examinations were done. Sample processing was done by following standard procedures and processes within the laboratory.
Urine culture
The urine specimens were gently mixed to avoid foaming. A calibrated loop (1 µl) full of the unspun urine was inoculated onto a CLED agar (Difco Laboratories GmbH, Augsburg, Germany) and streaked out for single colonies. These plates were then incubated under aerobic conditions (35-37°C) for 16-24 h. The plates were examined after the incubation period for significant growth. Biochemical tests such as catalase tests, coagulase tests and oxidase tests were performed to help identify the bacterial pathogens using Becton Dickinson’s Phoenix Spec Nephelometer and BBL Crystal semi-auto reader for bacterial pathogens at the Microbiology Laboratory of Kumasi Centre for Collaborative Research in Tropical Medicine (Malaria Research Centre, Agogo, Asante Akim North). All the microbiology procedures were quality controlled using American Type Culture Collection (ATCC) strains (Cheesbrough, 2009).
Antibiotic susceptibility testing
The antibacterial susceptibility testing of the pathogenic isolates was done using the Kirby-Bauer disk diffusion method (Bauer et al., 1966) following the definition of the Clinical and Laboratory Standards Institute using antibiotics containing discs from Oxoid. Mueller-Hinton agar (Difco Laboratories GmbH, Augsburg, Germany) was prepared following the guidelines of the Clinical and Laboratory Standards Institute (Clinical and Laboratory Standards Institute, 2006).
The sensitivity test was performed based on the guidelines provided by CLSI (Clinical and Laboratory Standards Institute, 2006). The mean of triplicate results was taken as the zone diameter. The antibiotics discs and the concentration used were ampicillin 25 μg, naladixic acid 30 μg, cefuroxime 25 μg, ciprofloxacin 25 μg, chloramphenicol 30 μg, ofloxacin 5 μg, erythromycin 5 μg, gentamicin 25 μg, amikacin 30 μg, nitrofurantoin 20 μg, ceftriazone 25 μg, streptomycin 25 μg, tetracycline 25 μg, cefotaxime 25 μg, imipenem 25 μg, meropenem 25 µg, flucloxacillin 25 μg, augmentin 25 μg and cloxacillin 25 μg. Isolates were classified as either resistant or intermediate sensitive or sensitive based on the CLSI definition (Clinical and Laboratory Standards Institute, 2006) and in accordance with WHO requirements (Onanuga et al., 2005). Resistant and intermediate isolates were grouped together for analysis in this study. An isolate was considered multi-drug resistant if it was resistant to at least three of the antibiotics tested (Santos et al., 2008). Quality control of the susceptibility discs were performed using reference strains of Escherichia coli (ATCC 25922), Pseudomonas aeruginosa (ATCC 27853), Staphylococcus aureus (ATCC 25923) and E. faecalis (ATCC 29212) of known sensitivity.
Urine microscopy
The remaining urine specimens were transferred into centrifuge tubes and spun at 4000 relative centrifugal force for 5 min. Each supernatant was decanted and the sediment remixed by tapping the bottom of the tube. A drop of well mixed sediment was transferred unto a microscopic slide, cover-slipped and examined microscopically as described earlier. The pellet was screened microscopically for epithelia, bacteria, Trichomonas vaginalis, Schistosoma spp. etc (Cheesbrough, 2009).
Bio-data analysis
Data generated in this study were entered on Microsoft Excel, cleaned and exported into Graph Pad Prism version 5.00 (Graph Pad software, San Diego California USA) for windows for the statistical analysis.
RESULTS
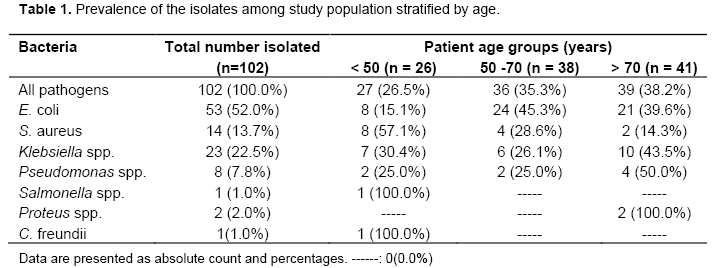
A total of 102 suspected UTI patients participated in the study. The mean age of the study patients was 62 years (Range: 2-93 years). The overall prevalence of pathogens was highest among the >70 years age group (40.2%). Whilst Klebsiella spp. (43.5%) and Pseudomonas spp. (50.0%) were the most predominant isolates within the >70 years age group, E. coli (45.3%) and S. aureus (57.1%) were the most predominant isolates within the <50 and 50-70 age groups (Table 1).
Susceptibility results of the isolates to the various antibiotics are presented in Table 2. Whilst Salmonella spp. showed the highest susceptibility rate of 15.8%, Klebsiella spp. was the least susceptible (9.2%) to antimicrobial agents used. Compared to the other isolates, E. coli was found to be susceptible to most of the antibiotics with about half of it susceptible to nitrofurantoin. With the exception of Citrobacter freundii which was completely resistant to all the antibiotics except imipenem and meropenem, at least one of all other isolates was susceptible to nitrofurantoin. The only isolated Salmonella spp. was susceptible to only nitrofurantoin, gentamycin and ciprofloxacin (Table 2).
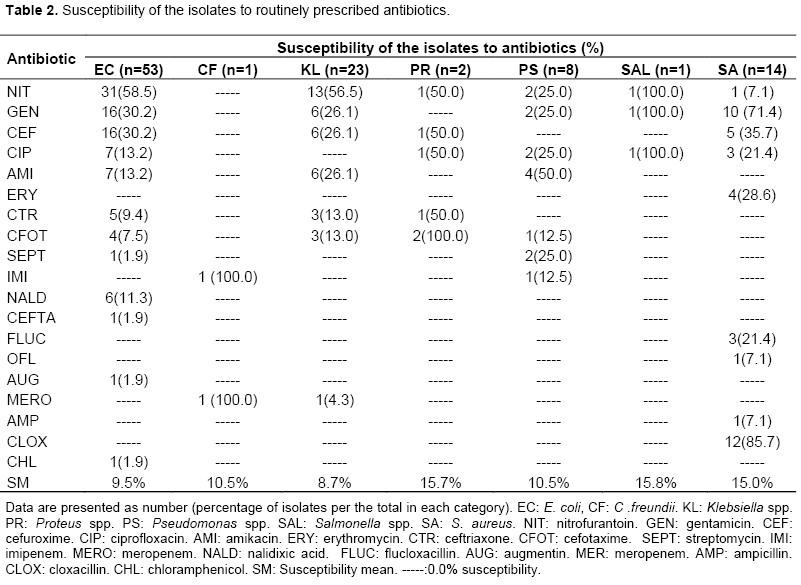
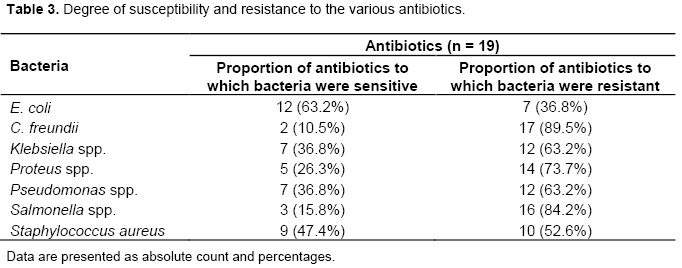
All the organisms except Citrobacter freundii showed a certain degree of susceptibility to nitrofurantoin (Table 2). The Gram-negative bacteria constituted the largest group (6 out of 7) with a prevalence of 85.70%, while Gram-positive bacteria constituted 14.30% of the total isolates. The proportions of the isolates showing multidrug resistance are shown in Table 3. The highest and least multi-drug susceptible bacterial isolates were E. coli and C. freundii respectively. A reverse trend was however observed for those two organisms in terms of multi-drug resistance. None of the isolates was sensitive to all the antibiotics tested and none, except E. coli was resistant to less than 10 of the 19 different antibiotics tested (Table 3).
DISCUSSION
Globally, urine culture has been identified as the gold stan-dard for infection assessment whereas the susceptibility Agogo Malaria Research Unit, Kumasi Centre for Collaborative Research in Tropical Medicine, Kumasi, Ghana testing also helps in antibiotic selection for therapeutic guidance. The various bacteria isolated from the urine samples were E. coli (52.0%), S. aureus (13.7%), Klebsiella spp. (22.5%), Pseudomonas spp. (7.8%), Salmonella spp. (1.0%), Proteus spp. (2.0%) and C. freundii (1.0%). These isolates represent clinically significant pathogens which are most often isolated from urine cultures. The significant bacteriuria identified in the urine samples of our study patients depicts a good clinical correlation between clinical and microbiological diagnosis as reported in western Nepal (Das et al., 2006).
The bacterial isolates in our study were mostly the Gram negative bacteria (85.70%) whereas the Gram positive bacteria accounted for 14.3%. This finding is consistent with a similar study conducted by Bahadin and colleagues (2011). This study also reported that the uropathogenic bacteria isolated from urine cultures were mainly the Gram negative type due to a number of properties that enables them to attach and invade urothelium as compared to the Gram positive bacteria (Bahadin et al., 2011).
E. coli (52.0%), the most common isolate was sensitive to 12 (63.2%) antibiotics but resistance to 7 (36.8%) anti-biotics, largely the most common microbial agent (Table 3). C. freundii was sensitive to only two antibiotics (imipenem and meropenem). The highest degree of antimicrobial resistance was identified with C. freundii (89.5%) followed by Salmonella spp. (84.2%), Proteus spp. (73.7%), Klebsiella spp. and Pseudomonas spp. (63.2% each), S. aureus (52.6%) and E. coli (36.8%).
The high rate of resistance to the penicillin based anti-biotics (such as ampicillin, amoxicillin, flucloxacillin, oxacillin, cloxacillin, etc.), tetracycline, aminoglycosides (such as streptomycin, gentamicin, etc.), etc. observed in this study may reflect the fact that these are the most commonly prescribed antibiotics at the hospital and also the most easily available in the community without prescription. The degree of resistance however reduced among quinolones (ciprofloxacin, nalidixic acid) and cephalosporins (including cefuroxime, ceftriaxone, cefotaxime, etc.). In their study of resistance to antimicrobial drugs in Ghana using bacterial isolates from a number of clinical specimens including urine, Newman and her colleagues reported similar findings from a study conducted in Ghana (Newman et al., 2011). They reported high resis-tance for ampicillin, chloramphenicol and cotrimoxazole whereas multi-drug resistance was observed for a combination of ampicillin, tetracycline, chloramphenicol and cotrimoxazole. Navaneeth and colleagues reported a similar resistant rate (80.0%) for Proteus spp. to a number of common antibiotics in India (Navaneeth et al., 2002). Resistance to antimicrobial agents has been noted since their first use and has gradually become a global challenge. A study done pointed out that high antimicrobial resistance rates in tertiary hospitals especially where both inpatients and outpatients are involved, could be due to some of those patients having complicated UTIs or having failed in previous UTI treatment (Mazzulli, 2002).
CONCLUSION
Overall susceptibility testing demonstrated a significantly reduced usefulness of common antibiotics and further strengthens the need for a re-evaluation of common antibiotics used in the therapeutic management of patients with urinary tract infection. This study’s results do indicate that antibiotics commonly used in UTIs are still effective, but species distribution and their susceptibility to antibiotics are rapidly changing. The important caution therefore is that antimicrobial susceptibility testing may have to be done in order to help select the appropriate antibiotic for effective treatment of diseases.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
We are thankful to all the study participants for taking part in the study. We are also thankful to the staff of the Urology and Microbiology Departments, KATH and Agogo Malaria Research Units for their support during the study.
REFERENCES
|
Abubakar El-Mahmood M (2009). Antimicrobial susceptibility pattern of pathogenic bacteria causing urinary tract infections at the Specialist Hospital, Yola, Adamawa state, Nigeria. J. Clin. Med. Res. 1(1):1-8 |
|
|
Al Sweih N, Jamal W, Rotimi VO (2008). Spectrum and antibiotic resistance of uropathogens isolated from hospital and community patients with urinary tract infections in two large hospitals in Kuwait. Med. Princ. Pract. 14(6):401-407 |
|
|
Bahadin J, Teo SSH, Mathew S (2011). Aetiology of community-acquired urinary tract infection and antimicrobial susceptibility patterns of uropathogens isolated. Singapore Med. J. 52(6):415-420 |
|
|
Bauer AW, Kirby WMM, Sherris JC, Turck M (1966). Antibiotic susceptibility testing by a standardizedsin-gle disk method. Am. J. Clin. Pathol. 45(4):493-496 |
|
|
Bhullar K, Waglechner N, Pawlowski A, Koteva K, Banks ED, Johnston MD, Barton HA, Wright GD (2012). Antibiotic resistance is prevalent in an isolated cave microbiome. PLoS One 7(4):e34953 |
|
|
Cheesbrough M (2009). Parasitological tests, In A. Moody, G. Malcolm, W. John, Eds, District Laboratory Practice in Tropical Countries, vol. 1, New York, U.S.A: Cambridge University Press. |
|
|
Clinical and Laboratory Standards Institute (CLSI) (2006). Performance Standards for Antimicrobial Susceptibility Testing; Sixteenth Informational Supplement. 26(3). |
|
|
Das RN, Chandrashekhar TS, Joshi HS, Gurung M, Shrestha N, Shivananda PG (2006). Frequency and susceptibility profile of pathogens causing urinary tract infections at a tertiary care hospital in western Nepal. Singapore Med. J. 47(4):281 |
|
|
Griebling T (2007). Urinary Tract Infection in men, In Litwin MS, Saigal CS, Eds, Urologic Diseases in America. US Department of Health and Human Services, Public Health Service, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases., Washington, DC:US Government Printing Office: NIH Publication No. 07-5512. pp. 623-645. |
|
|
Gupta K, Hooton TM, Stamm WE (2001). Increasing antimicrobial resistance and the management of uncomplicated community-acquired urinary tract infections. Ann. Intern. Med. 135(1):41-50 |
|
|
Kuo HC (1999). Clinical prostate score for diagnosis of bladder outlet obstruction by prostate measurements and uroflowmetry. Urology 54(1):90-96. |
|
|
Mazzulli T (2002). Resistance trends in urinary tract pathogens and impact on management. J. Urol. 168(4):1720-1722. |
|
|
Navaneeth BV, Belwadi S, Suganthi N (2002). Urinary pathogens' resistance to common antibiotics: a retrospective analysis. Trop. Doct. 32(1):20-22 |
|
|
Newman MJ, Frimpong E, Donkor ES, Opintan JA, Asamoah-Adu A (2011). Resistance to antimicrobial drugs in Ghana. Infect. Drug Resist. 4:215. |
|
|
Onanuga A, Oyi AR, Olayinka BO, Onaolapo JA (2005). Prevalence of community-associated multi-resistant Staphylococcus aureus among healthy women in Abuja, Nigeria. Afr. J. Biotechnol. 4(9) |
|
|
Santos AOD, Ueda-Nakamura T, Dias Filho BP, Veiga Junior VF, Pinto AC, Nakamura CV (2008). Antimicrobial activity of Brazilian copaiba oils obtained from different species of the Copaifera genus. Memórias do Instituto Oswaldo Cruz 103(3):277-281 |
|
|
WHO (2012). Antimicrobial resistance. http://www.who.int/mediacentre/factsheets/fs194/en/. Accessed July 2014. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


