Full Length Research Paper

ABSTRACT
The World Health Organization (WHO) ranks healthcare-associated infection (HCAI) as one of the top ten causes of hospital death worldwide. Hand hygiene is arguably the simplest and most effective way to prevent the transmission of HCAI between one patient to another or from patients to healthcare workers. The practical implementation of hand hygiene depends on the attitude and knowledge of health practitioners regarding hand hygiene practices. The authors, therefore, investigated the knowledge attitude and hand washing practices of healthcare workers in Tanzania. The study was an institutional-based descriptive cross-sectional study conducted at Muhimbili National Hospital between 23rd July and 21st August 2020. Ethical clearance for conducting research was issued by the Institutional Review Board of the Muhimbili University of Health and Allied Sciences, Tanzania. A total of 148 healthcare workers participated in the study. The mean age of the participants was 31.06 ± 8.160 years (range: 21 - 57). Females comprises of 50.7% of the participants. Unmarried participants constituted 61.5%. Regarding educational qualifications, 63.5% had a medical degree, while 31.8% were the nursing staff. It was found that the healthcare cadre correlated with the attitude toward hand hygiene. Of all the respondents, 62.2% had moderate knowledge about hand hygiene, while 35.10% had good knowledge. Regarding attitudes to hand hygiene practices, 62.8% had a good attitude. Concerning practices, 57.4% had good practices toward hand hygiene. More than half (64.9%) of the study participants received training in hand hygiene. Continued education and training programs should be implemented at healthcare facilities to increase hand washing compliance and knowledge among workers.
Key words: Attitude, hand hygiene, hand washing practices, HCAI, healthcare-associated infection, infection control and prevention, IPC, knowledge, Tanzania.
INTRODUCTION
Hand washing is the single most important infection prevention procedure. Washing hands with soap and water significantly reduces the number of organisms to prevent potential infections (Ahmed et al., 2020; Ejemot-Nwadiaro et al., 2021; Freeman et al., 2014). Hand washing should be performed after arriving at work, before leaving work, between client contacts, after removing gloves, when hands are visibly soiled, before eating, after urination and defecation, after contact with body fluids, before and after performing invasive procedures, and after handling contaminated equipment (Jemal, 2018). Furthermore, the World Health Organization (WHO) introduced "my five moments for handwashing," intending to minimize healthcare-associated infection (HCAI). The five moments emphasize handwashing before touching a patient, before performing aseptic and cleaning procedures, after being at risk of exposure to body fluids, after touching a patient, and after touching the patient’s surroundings (Van Nguyen et al., 2020). The time required for handwashing depends on the circumstances. High-risk areas such as nurseries usually require about a 2-min hand wash and soiled hands generally require more time (Jemal, 2018). However, the time recommended for washing hands to remove transient flora from hands range from 10 to 15 s.
HCAIs are infections that patients acquire while receiving treatment for medical or surgical conditions and are the most frequent adverse event during care delivery (Dellinger, 2016; Haque et al., 2018). HCAIs occur in all care settings, including hospitals, surgical centers, ambulatory clinics and long-term care facilities such as nursing homes and rehabilitation facilities. Globally, HCAI due to poor hand hygiene are a significant problem for the safety of the patient and the healthcare workers. HCAI impact prolonged hospital stays and increases the financial burden for patients and hospitals. It may also promote the antibiotic resistance of microorganisms due to associated treatment (Allegranzi et al., 2011).
HCAI concern 5–15% of hospitalized patients in developed countries and can affect 9–37% of those admitted to intensive care units (ICUs). Consequently, HCAI contribute to mortality and morbidity (World Health Organization, 2011).
HCAI; account for 37,000 attributable deaths in Europe and potentially many more that could be related and account for 99 000 deaths in the United States of America (Ahmed et al., 2020; World Health Organization, 2011). Despite limited data on HCAI in developing countries, the recent prevalence surveys in single hospitals in Albania, Morocco, Tunisia, and the United Republic of Tanzania indicated that HCAI prevalence rates varied between 14.8 and 19.1% (WHO Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clean Care Is Safer Care, n.d.). However, the study conducted in 2002 at Kilimanjaro Christian Medical Center (KCMC) in Tanzania showed the overall prevalence of HCAI to be 14.8% (Gosling et al., 2003), and surgical site infections are as high as 40% in one medical ICU (Gosling et al., 2003; The United Republic of Tanzania, 2012).
Although there is low compliance with hand hygiene among healthcare workers in both developed and developing countries, ensuring the availability of handwashing facilities (Kaplan and McGuckin, 1986), providing regular training, and reminding healthcare workers of the importance of hand hygiene have been shown to improve compliance with hand hygiene. A study conducted in Shiraz University of Medical Sciences hospitals, 2013 - 2014, indicated that shiraz healthcare workers had proper hand hygiene knowledge and attitudes; however, compliance was rated poor (Hosseinialhashemi et al., 2015). Furthermore, the study conducted in Northeast Ethiopia highlighted that 60(65.9%) were knowledgeable and 31(34.1%) were not knowledgeable. However, most health professionals, 51(56.0%), had poor practice and 40(43.0%) had a good handwashing practice. The majority of health professionals were knowledgeable. However, they had a poor practice of handwashing (Jemal, 2018).
Identifying and understanding individual cognitive factors associated with hand hygiene may help build successful hand hygiene promotion strategies. The factors that influence behavior may include knowledge, attitudes, beliefs and personality of individuals involved. To the authors knowledge, no study in Tanzania has tried to study individual cognitive factors related to hand hygiene among healthcare workers. Our study aimed to assess knowledge attitude and handwashing practices at Muhimbili National Hospital in Tanzania. This will help address the gap and intervention needed in infection prevention control in Tanzania.
METHODOLOGY
Study designing
This study was an institutional-based, descriptive, and cross-sectional one conducted at Muhimbili National Hospital (MNH) between 23rd July and 21st August 2020. Ethical clearance for conducting research was issued by the Institutional Review Board of the Muhimbili University of Health and Allied Sciences, Tanzania. Approval for conducting research was obtained from the Teaching, Research, and Consultancy unit of the MNH. Verbal consent was obtained and participation was voluntary for all the respondents.
Participants
Research participants were medical students, medical doctors, nurses, pharmacists, specialists from the obstetrics and gynecology department, surgery department, internal medicine department, and pediatrics department.
Sampling
A simple random sampling technique was used to select the study participants. A sample size of 148 was required to obtain a confidence level of 95% with a confidential interval of 5%. The sample size calculation was based on the research conducted in Pakistan, where the general knowledge level was 87.3% (Rao et al., 2012). The online survey tool REDcap was used in data collection. Healthcare workers were interviewed and then responses were recorded (Harris et al., 2009, 2019).
Questionnaire designing and scoring
The questionnaire was a modified version of the standardized questionnaire of WHO. A pilot survey was conducted using this modified version of the questionnaire and internal consistency was tested before its application to the designated sample (WHO Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clean Care Is Safer Care, n.d.; World Health Organization, 2009a, 2009b). The questionnaire included participants' social demographic characteristics, hand hygiene knowledge, hand washing practices, and attitude toward hand hygiene.
The demographics included age, gender, education level, profession, work experience, department of practices, and if they received handwashing training.
The knowledge questions were adopted from the WHO hand hygiene knowledge questionnaire and others previously used (Nair et al., 2014; World Health Organization, 2009a). Fourteen questions were asked where correct answer = 1 and wrong answer = 0. The attitude and handwashing questions were sampled from the WHO perception questionnaire and previously published research (World Health Organization, 2009b). Likert scale of 5 points were 1 = strongly agree, 2 = agree, 3 = neutral, 4 = strongly disagree and 5 = strongly disagree were used. The score in each part was high (greater or equal to 75%), moderate (74% - 50%) and poor (less than 50%). The score was adopted from research conducted in the Tertiary healthcare Centre in Raichur, India (Nair et al., 2014) and categorized as high hand hygiene, knowledge, high hand washing practices, and high attitude towards hand hygiene.
Data availability statement
The dataset associated with this study is privately stored at DRYAD repository https://datadryad.org/stash/share/r3nE_EHOtZo_vqFM_8NRci6YyUbNxOvYUFHwfYsrye8 With doi 10.5061/dryad.kd51c5b6q.
Statistical analysis
Data were extracted from Research Electronic Data Capture (REDCap) and then exported to Statistical Package for the Social Sciences (SPSS) version 24 for data analysis. The collected data were subjected to data quality scrutiny and cleaning. The results were presented using frequency, tables and charts. A Chi-square or Fisher-exact tests were used to test associations between categorical variables with knowledge attitude and hand hygiene practices. A p-value of less than 0.05 was considered statistically significant.
RESULTS
Out of 173 healthcare workers who were approached for consent to participate in the study, only 169 (97.7%) agreed to this survey, while 4 (2.3%) rejected participating in this survey. Of those accepted to participate, 148 (87.6%) had complete responses used for data analysis. In contrast, 21 (12.4%) had incomplete responses, therefore omitted from the data analysis.
Social demographics data
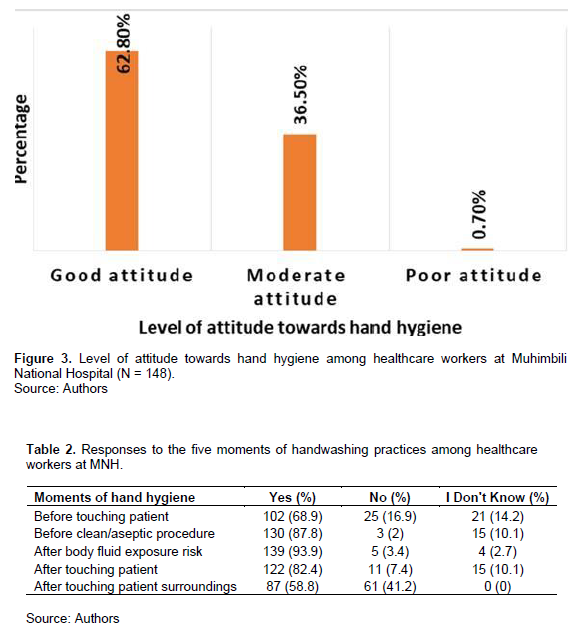
Of 148 respondents, the majority (50.7%) was female and 61.5% were single. In terms of religious denominations Christians predominated at the proportion of 77%. Most (63.5%) of the participants were bachelor's degree holders. The professional cadre of nurses constituted 31.8% of the respondents. The majority of participants (41.9%) were from the obstetrics and gynecology department (Table 1). A high proportion of the participants (64.9%) received formal training in hand hygiene practices.
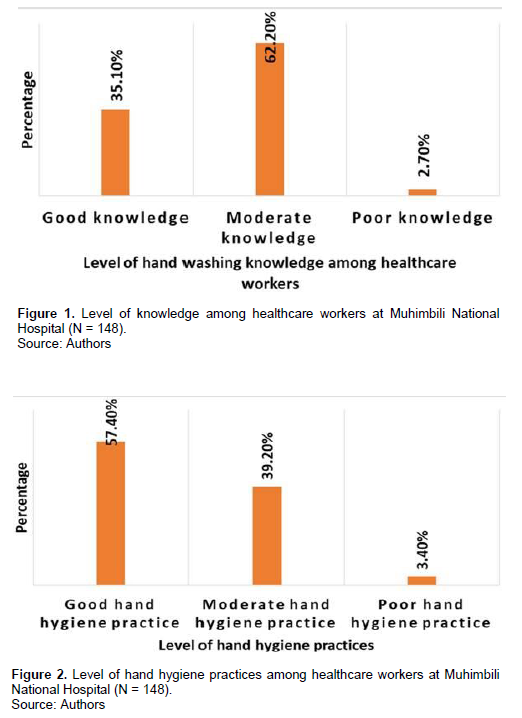
Knowledge of healthcare workers toward hand washing
Out of 148 healthcare workers enrolled in the study, most healthcare workers (62.2%) had moderate knowledge (Figure 1). Among all healthcare workers, 72 (48.7%) did not know the most critical reason healthcare workers practice good hand hygiene, 82 (55.4%) did not know the main route of cross-transmission of potentially harmful germs between patients in a healthcare facility. A total of 82 (58.1%) knew that alcohol-based hand rub is the best agent for killing bacteria. It was found that 124 (83.8%) agree that the healthcare worker's hands are a source for spreading resistant organisms to other patients.
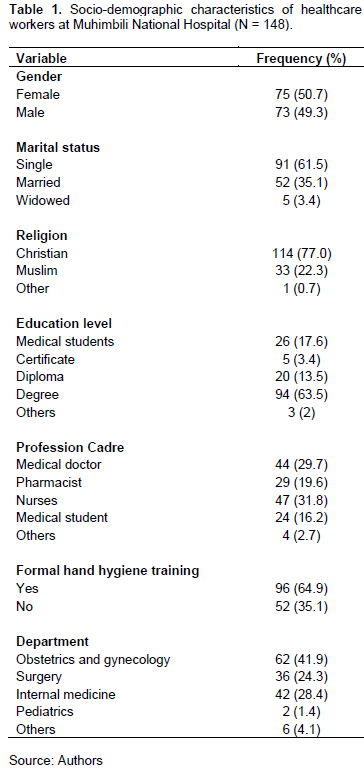
Handwashing practices among healthcare workers at Muhimbili National Hospital
Of all 148 respondents, 85 (57.4%) were categorized as having good hand hygiene practices, 58 (39.2%) were categorized as having moderate hand hygiene and also 5 (3.4%) were categorized as having poor hand hygiene practices (Figure 2).
Healthcare workers' hand hygiene practices according to five moments of handwashing, 102 (68.9%) washed their hands before touching a patient, 130 (87.6%) washed their hands before an aseptic procedure, 139 (93.9%) washed their hands after being exposed to body fluids of a patient 122 (82.4%) washed their hands after touching patient 87 (58.8%) washed their hands after touching patient's surroundings (Table 2).
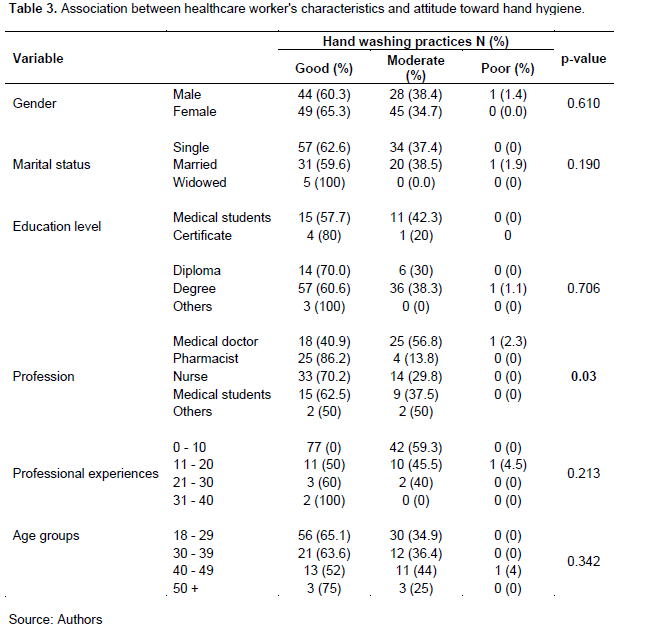
Attitude towards handwashing among healthcare workers
Out of 148 respondents, the majority (62.8%) were categorized as having a good attitude towards hand washing (Figure 3). (50%) considered hand washing practices to be useful, (54%) answered that it is not difficult to perform hand hygiene, (85.8%) perceived education on hand hygiene to each healthcare worker would improve hand hygiene permanently in your institution, (89.2%) agreed if leaders and senior managers at Muhimbili National Hospital support and openly promote hand hygiene would improve hand hygiene.
Association between socio-demographic characteristics with hand hygiene practices and attitude
There was no statistically significant difference in healthcare workers' knowledge, attitude, and handwashing practices between gender, marital status, education level, and professional experience (Table 3). However, there were statistically significant observed in the profession's attitude toward hand hygiene.
DISCUSSION
There is extensive evidence of knowledge on how proper hand hygiene practices can avoid the problem of HCAI in many healthcare settings (Ahmed et al., 2020). The authors therefore, conducted a study to investigate the knowledge, attitude and practice of hand hygiene in Tanzania, to add up to this body of knowledge.
A total of 148 healthcare workers from the cadres of doctors, nurses, pharmacists and medical students consented to participate in this survey. A high proportion (62.2%) of respondents showed moderate knowledge. In addition, 57.4% had good hand hygiene practices, while also (62.8%) had a good attitude toward hand hygiene.
Among all participants, 62.2% of MNH healthcare workers had moderate knowledge. This is low compared to research conducted in two teaching hospitals (Hashemi-Nejad and Emem Reza hospitals) in Mashhad, Iran, between May 2014 and September 2015 (Zakeri et al., 2017). The majority (68%) of respondents had moderate knowledge. On another occasion, a study conducted among medical residents in Imam Hossein hospital, Iran, in 2013 showed that medical residents had moderate knowledge of hand hygiene, 65.7%, higher than the findings (Nabavi et al., 2015). The results point to an increased need to improve hand hygiene conditions and educate them further according to the WHO guidelines. It was note that, despite nurses spending much time with patients because of their work schedule, their hand hygiene knowledge is as good as expected. Findings showed that (76.6%) of nurses had moderate hand hygiene knowledge and (23.4%) had good knowledge. This underscores the need for increased training and emphasis on hand hygiene among nurses. Healthcare workers' characteristics had no significant effect on hand hygiene knowledge. Of all participants (51.4%) knew the single most important reason for healthcare workers to practice good hand hygiene. A cross-sectional, hospital-based survey conducted in major public sector hospitals of Faisalabad, Lahore, Quetta, Islamabad Multan, Jamshoro and Peshawar showed that healthcare workers had good (98%) knowledge. Concerning the reason for healthcare workers practice hand hygiene (Rao et al., 2012), 44.6% knew the main route of cross-transmission of potentially harmful germs between patients in a healthcare facility, (58.1%) knew that alcohol-based hand rub is the best agent in killing bacteria (18.2%), knew how much time would an ICU nurse save during an 8-h shift by using an alcohol-based hand rub instead of soap and water. This explains the importance of increasing training among healthcare workers to improve hand hygiene knowledge in essential areas.
Of the respondents in the study, 57.4% scored good handwashing practices. Regarding five handwashing moments, 130 (87.8%) participants always washed their hands before clean and aseptic procedures. The result was higher than the results obtained in Northeast Ethiopia, where 36.3% of participants washed their hands before clean and aseptic procedures (Jemal, 2018). About 102 (68.9%) of participants always washed their hands before individual patient contact, but this result was higher compared to 21 (60.1%) in a study conducted in Pakistan. In addition, 64 (43.2%) always used alcohol-based hand rub for hand hygiene.
In the current study, only 122 (82.4%) washed their hands after contact with patients, compared to a survey conducted in Ethiopia, where 78% of healthcare workers washed their hands after contact with body secretions. At the same time, research showed that 139 (93.9%) washed hands after contact with body secretions. When comparing these two studies, healthcare workers adhere to washing hands after body fluid exposure more often than the other five moments of hand hygiene. This can be explained that healthcare workers are more concerned about conditions threatening their health than conditions threatening patients' health. Therefore, healthcare workers' major concern was to protect themselves.
Healthcare workers' characteristics showed no statistically significant relationship with handwashing practices. However, the study done in Australia showed that gender played an important role in influencing healthcare workers' handwashing rate (van de Mortel et al., 2001).
In this study, only 93 (62.8%) were categorized as having a good attitude towards hand hygiene. However, the survey conducted in Jordan showed that attitude towards handwashing was 65.28% higher than the results (Ghafari and Aburuz, 2019).
It was lower than the overall attitude towards hand hygiene conducted at Anuradhapura Teaching Hospital Sri Lanka, whereby 47.5% had good attitudes, 42.5% had moderate attitudes and 10% showed poor hand hygiene attitudes (Kudavidnange et al., 2013). Most studied healthcare workers had a positive attitude toward hand hygiene in the present study. However, 50% strongly agreed that hand hygiene is helpful before and after touching the patient, before clean/ aseptic procedures, after body fluid exposure, after touching the patient, and after touching the patient's surroundings.
Moreover, 28% agreed that it is difficult to comply with hand hygiene to improve hand hygiene compliance. Of all participants, 81.7% agreed that if healthcare facilities make alcohol-based hand rub always available, it will improve hand hygiene permanently in their institution. Furthermore, the majority of healthcare workers believed that displaying reminders, education and promotion of hand hygiene by seniors and leaders would improve hand hygiene practices in their institution.
Some study constraints may limit the interpretation of the results. First, this was only a single-center study conducted at the National Hospital in the country. The current setting may benefit from more availability of knowledgeable healthcare workers in aspects of hand hygiene as opposed to remote settings in the country. Secondly, because the study was conducted during the first peak of the emerging COVID-19 pandemic, most responses may have been influenced by the prevailing pandemic. In addition, the proportion of different cadres may not be well balanced, and at the time of the survey, a few medical students in their final years of training were included in the study. The inclusion of these medical students may have counteracted some of the findings. Nevertheless, this cadre of healthcare workers has a pivotal role in serving the patients at the study site. Therefore, their responses were relevant to the practice of hand hygiene in Tanzania.
CONCLUSION
Even though most healthcare workers were found to have good hand washing practices and attitudes, there is an urgent need to introduce measures and strategies to increase the knowledge, attitudes and handwashing practices at Muhimbili National Hospital and other healthcare settings in Tanzania. The suggested initiative may play a crucial role in improving hand hygiene compliance among healthcare workers. Finally, it was recommend that further study should be conducted to observe handwashing practices and assess the effect of availability of handwashing facilities on handwashing practices, knowledge and attitude toward hand hygiene among healthcare workers.
ACKNOWLEDGMENT
The authors would like to thank all the participating healthcare workers.
ETHICS APPROVAL
Consent was obtained or waived by all participants in this study. Muhimbili University of Health and Allied Sciences issued approval DA.25/111/01/10/Feb/2020. Ethical clearance for conducting research was issued by the Institutional Review Board of the Muhimbili University of Health and Allied Sciences, Tanzania. Approval for conducting research was obtained from the Teaching, Research, and Consultancy unit of the Muhimbili National Hospital. Verbal consent was obtained and participation was voluntary for all the respondents.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Ahmed J, Malik F, Memon Z A, Bin Arif T, Ali A, Nasim S, Ahmad J, Khan M A (2020). Compliance and Knowledge of Healthcare Workers Regarding Hand Hygiene and Use of Disinfectants: A Study Based in Karachi. Cureus 12(2). |
|
|
Allegranzi B, Nejad SB, Combescure C, Graafmans W, Attar H, Donaldson L, Pittet D (2011). Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. The Lancet 377(9761):228-241. |
|
|
Dellinger EP (2016). Prevention of Hospital-Acquired Infections. Surgical Infections 17(4):422-426. |
|
|
Ejemot-Nwadiaro RI, Ehiri JE, Arikpo D, Meremikwu MM, Critchley JA (2021). Hand-washing promotion for preventing diarrhoea. Cochrane Database of Systematic Reviews 1. |
|
|
Freeman MC, Stocks ME, Cumming O, Jeandron A, Higgins JPT, Wolf J, Prüss-Ustün A, Bonjour S, Hunter PR, Fewtrell L, Curtis V (2014). Hygiene and health: systematic review of handwashing practices worldwide and update of health effects. Tropical Medicine and International Health 19(8):906-916. |
|
|
Ghafari ZA, Aburuz ME (2019). Hand Hygiene Knowledge, Attitude and Barriers among Jordanian Nurses. International Medical Journal, 24(03):385-400. |
|
|
Gosling R, Mbatia R, Savage A, Mulligan JA, Reyburn H (2003). Prevalence of hospital-acquired infections in a tertiary referral hospital in northern Tanzania. Annals of Tropical Medicine and Parasitology 97(1):69-73. |
|
|
Haque M, Sartelli M, McKimm J, Abu Bakar M (2018). Health care-associated infections - an overview. Infection and Drug Resistance 11:2321-2333. |
|
|
Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O'Neal L, McLeod L, Delacqua G, Delacqua F, Kirby J, Duda SN (2019). The REDCap consortium: Building an international community of software platform partners. Journal of Biomedical Informatics 95:103208. |
|
|
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG (2009). Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics 42(2):377-381. |
|
|
Hosseinialhashemi M, Kermani FS, Palenik CJ, Pourasghari H, Askarian M (2015). Knowledge, attitudes, and practices of health care personnel concerning hand hygiene in Shiraz University of Medical Sciences hospitals, 2013-2014. American Journal of Infection Control 43(9):1009-1011. |
|
|
Jemal S (2018). Knowledge and Practices of Hand Washing among Health Professionals in Dubti Referral Hospital, Dubti, Afar, Northeast Ethiopia. Advances in Preventive Medicine 1-7. |
|
|
Kaplan LM, McGuckin M (1986). Increasing handwashing compliance with more accessible sinks. Infection Control? 7(8):408-410. |
|
|
Kudavidnange B, Gunasekara T, Hapuarachchi S (2013). Knowledge, attitudes and practices on hand hygiene among ICU staff in Anuradhapura Teaching hospital. Anuradhapura Medical Journal 5(1):29. |
|
|
Nabavi M, Alavi-Moghaddam M, Gachkar L, Moeinian M (2015). Knowledge, Attitudes, and Practices Study on Hand Hygiene Among Imam Hossein Hospital's Residents in 2013. Iranian Red Crescent Medical Journal 17(10). |
|
|
Nair SS, Hanumantappa R, Hiremath SG, Siraj MA, Raghunath P (2014). Knowledge, Attitude, and Practice of Hand Hygiene among Medical and Nursing Students at a Tertiary Health Care Centre in Raichur, India. International Scholarly Research Notices Preventive Medicine pp. 1-4. |
|
|
Rao MH, Arain GM, Khan MI, Taseer I, Talreja K, Ali G, Munir MK, Naz S, Hussain I, Ahmed J, Talreja L, Ali G, Munir MK, Naz S, Hussain I, Ahmed J (2012). Assessment of Knowledge, Attitude and Practices Pattern of Hand Washing in Some Major Public Sector Hospitals of Pakistan (A Multi-Center Study). Pakistan Journal of Medical Research 51(3):76-82. |
|
|
The United Republic of Tanzania (2012). National Communication Strategy for Infection Prevention and Control 2012-2017. |
|
|
van de Mortel T, Bourke R, McLoughlin J, Nonu M, Reis M (2001). Gender influences handwashing rates in the critical care unit. American Journal of Infection Control 29(6):395-399. |
|
|
Van Nguyen H, Tran HT, Khuong LQ, Van Nguyen T, Ho NT, Dao AT, Van Hoang M (2020). Healthcare Workers' Knowledge and Attitudes Regarding the World Health Organization's "My 5 Moments for Hand Hygiene": Evidence From a Vietnamese Central General Hospital. Journal of Preventive Medicine and Public Health 53(4):236-244. |
|
|
WHO Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clean Care Is Safer Care (2009). Retrieved May 2, 2022, from |
|
|
World Health Organization (2011). Report on the burden of endemic health care-associated infection worldwide: Clean care is safer care. |
|
|
World Health Organization (2009a). Hand Hygiene Knowledge Questionnaire for Health-Care Workers. |
|
|
World Health Organization (2009b). Perception Survey for Health-Care Workers. Available online: View |
|
|
Zakeri H, Ahmadi F, Rafeemanesh E, Afshari Saleh L (2017). The knowledge of hand hygiene among the healthcare workers of two teaching hospitals in Mashhad. Electronic Physician 9(8):5159-5165. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


