ABSTRACT
This work aimed at the phenotypic and molecular characterization of inducible clindamycin resistance among strains of Staphylococcus aureus isolated from cancer patients with febrile neutropenia. Out of 231clinical specimens Staphylococci were isolated from 179 (77.48%) cases. Isolates were identified by conventional microbiological methods. Antimicrobial sensitivity to all isolates was done using disc diffusion methods. For strains that were erythromycin resistant, D-test was performed to screen the presence of inducible clindamycin resistance. Multiplex polymerase chain reaction (multiplex-PCR) was done for strains with constitutive or inducible resistance to detect the distribution of erm (e), and erm (C) genes. Out of 231 clinical specimens, staphylococci were isolated from 179 (77.48%). Staphylococcal isolates were tested for susceptibility to erythromycin; 100 (55.8%) of them were erythromycin resistant. of these 100, erythromycin resistant isolates (8, 4.46%) were resistant to both erythromycin and clindamycin indicating constitutive MLSB Phenotype; 92 isolates were erythromycin resistant, and clindamycin sensitive. Out of these, 45 (25.1%) isolates showed positive D test indicating inducible MLSB phenotype while 47(26.2%) gave negative D test indicating MS phenotype. Molecular study revealed that 8 strains (100%) of staphylococci with constitutive MLSB phenotype and 23 strains (51.1%) of staphylococci with inducible MLSB phenotype had both erm(e) and erm(c) gene, erm (e) gene was present in 33.3% and erm (c) gene present in 15.6% of staphylococcus isolates with inducible MLS B phenotype. Inducible resistance and MS phenotype were found to be higher in MRSA as compared to MSSA (27.6, 24.3 and 1.6 and 4% respectively). Rapid dissemination of inducible clindamycin-resistant S. aureus isolates is worrisome and calls for judicious use of antibiotics. Therefore, the D-test should be added as a routine procedure on each staphylococcal isolates to detect inducible clindamycin resistance to avoid failure of antibiotic therapy.
Key words: Clindamycin, Staphylococcus aureus, antimicrobial susceptibility.
Febrile neutropenia is defined as fever with other signs of infection, in a patient with neutropenia, which is considered with abnormal low concentration of neutrophils granulocytes (<500 cells/mm3), the most abundant circulating white blood cells that is considered the first line of the organism defence against infections (Viscoli et al., 2005). Percentage of patients with malignancy experience a decrease in the cells and other elements of the immune systems that make them more liable to different types of infections (Lustberg, 2012). Neutropenia could be considered as an oncology emergency and can lead to serious adverse consequences such as serious infection complications and death (Villafuerte et al., 2014). Bacteria, including Gram-positive and Gram-negative species, viruses, and fungi; all of these may be a causative agent of febrile neutropenia. The incidence and epidemiology of febrile neutroprnia depends on different factors including type of cancer, the age, and sex of the patient, the type and cycle of treatment (Kristjanson, 2015).
Staphylococcus aureus (S. aureus) is considered as one of the most common organisms causing infections in patients with malignancy with increasing the risk of resistance to wide range of antibacterial drugs. Macrolide-Lincosamide-Streptogramin B (MLSB) is a group of antibiotics that are nowadays used in treatment of S. aureus infections. Clindamycin is the most preferred antimicrobial drug in this group due to its proper pharmacokinetic properties that led to increase development of clindamycin resistance among strains of S. aureus (Yilmaz et al., 2007).
Clindamycin resistance in Staphylococcus species can be either constitutive or inducible (Deotale et al., 2010). It is difficult to detect strains of S. aureus that have inducible clindamycin resistance by routine laboratory methods as they appears as erythromycin-resistant and clindamycin sensitive in routine laboratory in vitro disc diffusion tests when the two discs of erythromycin and clindamycin not placed adjacent to each other (Lim et al., 2006). When these cases are treated with clindamycin; the target will be constitutive erm genes that lead to failure of treatment (Drinkovic et al., 2001). Strains of S. aureus that have msrA genes (efflux genes) have with another mechanism of resistance that presented clinically as erythromycin-resistant and clindamycin-sensitive both in vivo and in vitro, with no resistance to clindamycin resistance during therapy (Laclercq, 2002).
The aim of this study was to detect the incidence of staphylococcus aureus causing infection among cancer patients with febrile neutropenia with phenotypic and molecular characterization of inducible and constitutive clindamycin resistance among these strains.
A prospective study was carried out in the Department of Medical Microbiology and Immunology, Faculty of Medicine, Tanta University over a period of 6 months from September 2017 to March 2018 on 273 cancer patients with febrile neutropenia admitted to Oncology Department in Tanta University Hospital with suspected clinical sepsis after the approval of ethical committee in Tanta Faculty of Medicine, and a written consent from the participated patients. Clinical sepsis was defined as per the criteria established by American College of Physicians and Society of Critical Care Medicine (ACOM, SCCM) which included temperature >38°C, heart rate >90/min and respiratory rate >20/min. Neutropenia was defined as an absolute neutrophilic count (ANC) of 500 mm3 or less or a count that is expected to fall to that level in the next 1-2 days (Steven and John, 2008).
Out of 273 samples 100 staphylococci strains could be isolated that were eligible for the study.
Different patient samples (pus, throat swabs, blood, urine, sputum) were collected from the patients under complete asepsis and transferred immediately to microbiology laboratory. Samples were cultured on blood agar and mannitol salt agar. Staphylococci were identified using conventional microbiological methods and biochemical reactions; coagulase test and catalase test according to the standards of Clinical and Laboratory Standards Institute (2007).
Antibiotic susceptibility testing
Antibiotic susceptibility testing was performed using the disk diffusion method. The antibiotics chosen were Erythromycin, Clindamycin, vancomycin, gentamicin, oxacillin, cefotaxime, ciprofloxacin, cefepime and meropenem, Interpretation of the results acoording to the standards of Clinical and Laboratory Standards Institute (2007).
Phenotypic identification of clindamycin resistance (D-test)
All erythromycin-resistant isolates were further examined by double-disc test with erythromycin (15 μg) and clindamycin (2 μg) discs and the results were interpreted according to Clinical and Laboratory Standards Institute (2007) guidelines, to determine the resistance phenotype. According to the results of D-test; 3 phenotypes could be identified MSB phenotype, showed circular zone around clindamycin disc, iMLSB (indicible resistance) phenotype, demonstrated a flat zone around clindamycin disc, and cMLS phenotype were resistant to both discs of erythromycin and clindamycin (constitutive resistance).
Multiplex PCR for Genotypic identification of staphylococcal strains with clindamycin resistance
DNA extraction
QIAamp DNA Mini Kit (Qiagen) was used for isolation of genomic presence of erythromycin resistance methylase erm genes erm (e), and erm (C) PCR using the primer pairs as described by Lim et al. (2006).
Multiplex PCR for erm (a) and erm (c) was performed in final volume of 20 μl by DFS Master Mix Kit (Cinagen) including Taq polymerase enzyme, MgCl2, dNTP, (NH4)2SO4, TrisHCl, Tween –20. Reaction mixtures consisted of 12.5 μl Master Mix, 1 μl MgCl2, 0.25 μl of each primer, 2 μl distilled water and 1 μl DNA template. Cycling conditions were primary denaturation at 94°C for 4 min, denaturation at 94°C for 30 s, annealing at 52ºC for 30 s, extension at 72ºC for 1 min, then 30 cycle, followed by a final extension at 72ºC for 5 min. Primers used for erm (a) gene were: 5’ TCA GGA AAA GGA CAT TTT ACC3’, : 3’ATA TAGTGG TGG TAC TTT TTT GAG C5’detedted at 118 bp, erm (c) gene 5’TAGCAAACCCGTATTCCACG3’,3’CTTGTTGATCACGATAATTTCC5’detected at 495bp, (Matthew et al., 2006).
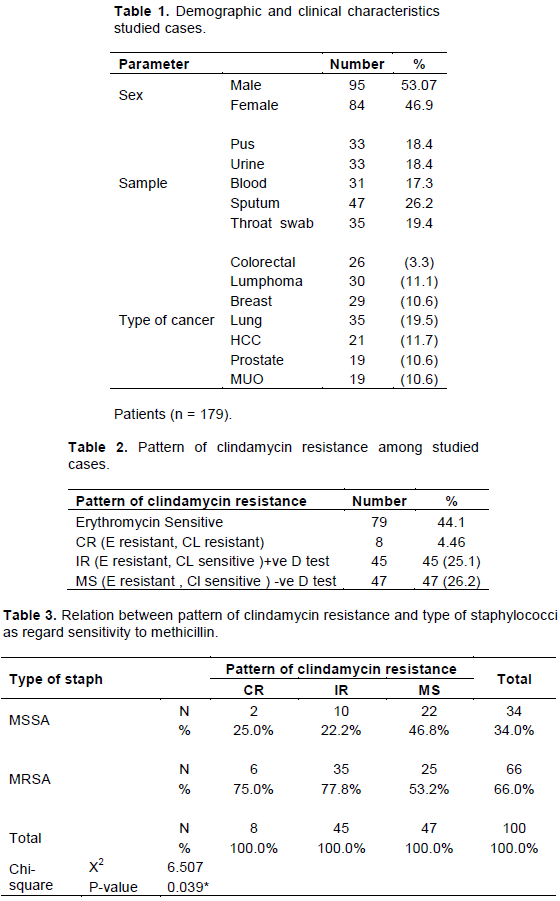
Table 1 shows the demographic and clinical characteristics studied cases where among 179 cases from which S. aureus were isolated, 95 cases were male patients and 84 were female patients, with their age from 18 to 72 (33±24.66), samples were collected from different sites according to the site of infection; pus 33 (18.4%), urine 33 (18.4%), blood 31 (17.3%), sputum 47 (26.2), throat swab 35 (19.4%). Colorectal cancer represent 3.3%, lymphoma 11%, Breast 10.6%, lung 19.5%, Hepatocellular carcinoma (HCC) 11.7%, Prostate 10.6% and Metastasis of unknown origin (MUO) 10.6%.
Table 2 shows pattern of clindamycin resistance among studied cases where among 179 S. aureus that were eligible for the study, 79 (44.1%) strains were erythromycin sensitive, and 100 (55.8%) of them were erythromycin resistant. Of these 100 erythromycin resistant strains, 8 (4.46%) isolates were resistant to both erythromycin and clindamycin indicating constitutive MLSB phenotype; 92 isolates were erythromycin resistant, and clindamycin sensitive. Out of these, 45 (25.1%) isolates showed positive D test indicating inducible clindamycin resistance (MLSB phenotype) while 47(26.2%) gave negative D test indicating MS phenotype.
Table 3 shows relation between pattern of clindamycin resistance and type of staphylococci as regard sensitivity to methicillin where constitutive MLS B Phenotype was found in higher percentage in MRSA [2 strains (25%)] of MSSA and 6 strains (70%) of MRSA; inducible MLS B phenotype found also in higher percentage in MRSA (10 strains (22.2%) of MSSA and 35 strains of MRSA (77.8%). As regard MS, phenotype was equally distributed in MSSA and MRSA [22 strains (46.8%) and 25 strains (53.2)] respectively.
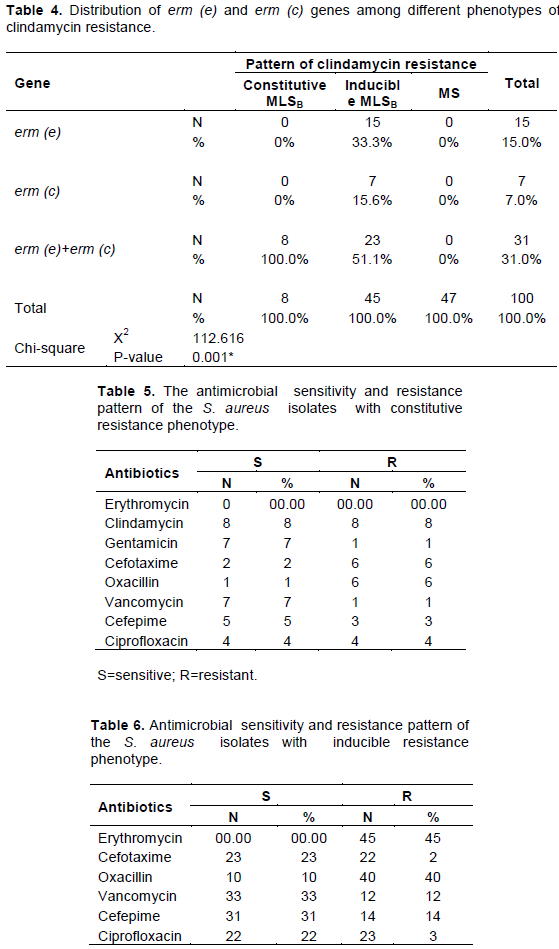
Table 4 shows the distribution of erm (e) and erm (c) genes among different phenotypes of clindamycin resistance where it was found that 100% of the strains with constitutive resistance phenotype contain both erm(e) and erm(c) gene, and as regard strains with inducible resistance phenotype, 15 strains (33%) contain erm(e )gene, 7 strains (15.8%) contain erm(c) gene, 23 strains (51%) contain both erm (c) and erm(e) genes
Table 5 shows the antimicrobial sensitivity and resistance pattern of the S. aureus isolates with constitutive resistance phenotype where highest sensitivity was for vanomycin (98.7%), oxacillin (97.4%), cefpime and ciprofloxacillin (83.5%) each, and all of the erythromycin sensitive strains were clindamycin sensitive.
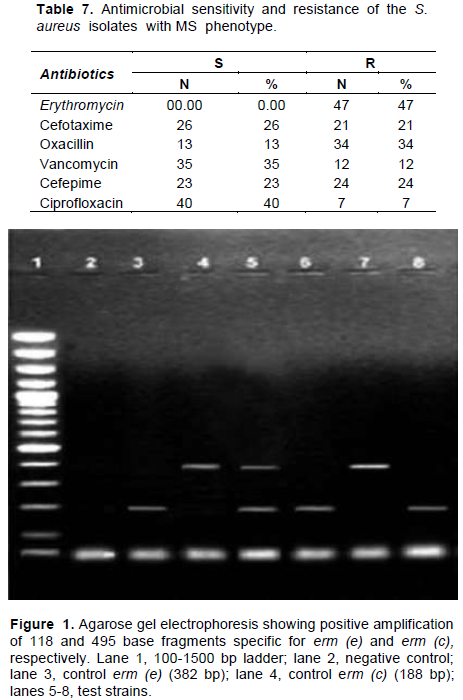
Tables 6 and 7 shows the antimicrobial sensitivity and resistance pattern of staphylococcal strains with inducible resistance phenotype where 75% of the strains were resistant to meropenem, gentamycin, and ciprofloxacin, 62% of the strains were resistant to cefotaxim , 50% were resistant to cefepime, and 100% of the strains were vancomycin sensitive. Agarose gel electrophoresis showing positive amplification of 118 and 495 base fragments is shown in Figure 1.
Cancer patients receiving cytotoxic antineoplastic therapy are at risk for invasive infection due to colonizing bacteria or fungi that translocate across intestinal mucosal surfaces. Since the magnitude of the neutrophil-mediated component of the inflammatory response may be muted in neutropenic patients. The first-line empirical treatment should cover the prevalent microorganism of the institute.
This study performed on 231 cases of febrile neutropenia from which Staphylococcus aureus could be isolated from 179 (77.4%). On reverse to this work, a study performed by Taj et al. (2015) found that Gram negative infections accounted for 68 (85%) and Escherichia coli was the commonest isolate. Gram positive microorganisms were isolated in 12 (15%) cases and most common was S. aureus. This study reported only one staphylococcus isolate (1%) with constitutive clindamycin resistance; resistant to vancomycin and 12 strains with inducible clindamycin resistance (12%) were resistant to vancomycin. Taj et al. (2015) also reported that the commonest Gram positive isolate is S. aureus and 4 cases of MRSA were isolated: all were sensitive to vancomycin; however, 2 cases of vancomycin resistant enterococci (VRE) were documented and were treated successfully with linezolid. In this study, sputum samples represents 26%, pus and urine 18.4 and 18.4% respectively, throat swab 19.4%, blood 17.3% of the clinical samples of cancer patients febrile neutropenia. Anderson et al. (2006) and Nasehi et al. (2010) reported that the most common infections that complicate cancer patients with febrile neutropenia include urinary tract infections, soft tissue infection, pneumonia, and septicaemia.In this study, out of 179 S .aureus that were eligible for the study, 79 (44.1%) strains were erythromycin sensitive, and 100 (55.8%) of them were erythromycin resistant. Of these 100 erythromycin resistant strains, 8 (4.46%) isolates were resistant to both erythromycin and clindamycin indicating constitutive MLSB Phenotype; 92 isolates were erythromycin resistant, and clindamycin sensitive. Out of these, 45 (25.1%) isolates showed positive D test indicating inducible MLS B phenotype while 47 (26.2%) gave negative D test indicating MS phenotype.
The study of Deotale et al. (2010) showed high percentage of erythromycin resistant isolates [80 (32.4%)]. Amongst them 36 (45%) isolates tested positive for inducible clindamycin resistance by D test while the rest of the isolates were negative for D test, out of which 9 (11.25%) were shown to have constitutive clindamycin resistance and 35 (43.75%) showed true sensitivity to clindamycin (MS phenotype).They reported that these results indicate that D test must be done as a routine laboratory procedure otherwise most of the erythromycin resistant isolates will be misidentified as clindamycin sensitive resulting in failure of treatment. As regard the relation of pattern of clindamycin resistance to the type of sensitivity of S .aureus to mecithelline, the results of this study showed that constitutive MLSB Phenotype was found in higher percentage in MRSA [2 strains (25%) of MSSA and 6 strains (70%) of MRSA), inducible MLS B phenotype were found also in higher percentage in MRSA [10 strains (22.2%) of MSSA and 35 strains of MRSA (77.8%)]. As regard MS, phenotype was equally distributed in MSSA and MRSA [22 strains (46.8%) and 25 strains (53.2)] respectively. These results are in accordance with the results of Kavitha et al. (2011) who observed that percentages of inducible resistance and constitutive clindamycin resistance were higher amongst MRSA as compared to MSSA (20, 16.66, 6.15, and 6.15%, respectively).
As regard the antimicrobial sensitivity and resistance pattern of the S. aureus, isolates with constitutive resistance phenotype in this study showed that highest sensitivity was to vanomycin (98.7%), oxacillin (97.4%), cefpime and ciprofloxacillin (83.5% each), and all of the erythromycin sensitive strains were clindamycin sensitive.
Moreover and as regard the antimicrobial sensitivity and resistance pattern of staphylococcal strains with inducible resistance phenotype, the results of this study showed that 75% of the strains were resistant to meropenem, gentamycin, and ciprofloxacin, 62% of the strains were resistant to cefotaxim, 50% were resistant to cefepime, and 100% of the strains were vancomycin sensitive.
Rapid dissemination of inducible clindamycin-resistant among isolates of S. aureus is worrisome and calls for judicious use of antibiotics. Therefore, the D-test should be added as a routine procedure of antimicrobial susceptibility tests on S. aureus isolates to detect inducible clindamycin resistance to avoid failure of antibiotic therapy with improvement of the mortality rate among cancer patients with febrile neutropenia.
The authors have not declared any conflict of interests.
The teamwork of this research greatly acknowledge departments of Medical Microbiology and Immunology, Tropical Medicine, Internal Medicine, Clinical Oncology for their great help and support.
REFERENCES
|
Anderson DJ, Engemann JJ, Harrell LJ, Carmeli Y, Reller LB, Kaye KS (2006). Predictors of Mortality in Patients eith Bloodstream Infections Due to ceftazidime-Resistant Klebsiella Pneumoniae. Antimicrobial Agents and Chemotherapy 50:1715-1720.
Crossref
|
|
|
|
Clinical and Laboratory Standards Institute (CLSI) (2007). Performance standards for antimicrobial susceptibility testing; seventeenth informational supplement. CLSI document M100-S17. Wayne, PA, USA.
|
|
|
|
|
Deotale V, Mendiratta DK, Raut U, Narang P (2010). Inducible clindamycin resistance in Staphylococcus aureus isolated from clinical samples. Indian Journal of Medical Microbiology 28:124-126.
Crossref
|
|
|
|
|
Drinkovic D, Fuller ER, Shore KP, Holland DJ, Ellis-Pegler R (2001). Clindamycin treatment of Staphylococcus aureus expressing inducible clindamycin resistance. Journal of Antimicrobial Chemotherapy 48:315-316.
Crossref
|
|
|
|
|
Kavitha P, Sunil RA, Venkatakrishna R (2011). Inducible Clindamycin Resistance in Staphylococcus aureus Isolated from Clinical Samples. Journal of Laboratory Physicians 3(1):25-27.
Crossref
|
|
|
|
|
Kristjanson M (2015). Febrile neutropenia, the empirical strike back. Cancer Care Monitoba 6:1-6.
|
|
|
|
|
Laclercq R (2002). Mechanisms of resistance to macrolides and lincosamides: Nature of resistance elements and their clinical implications. Clinical Infectious Diseases 34:482-492.
Crossref
|
|
|
|
|
Lim HS, Lee H, Roh KH, Yum JH, Yong D, Lee K, Chong Y (2006). Prevalence of inducible clindamycin resistance in staphylococcal isolates at Korean tertiary care hospital. Yonsei Medical Journal 47:480-484.
Crossref
|
|
|
|
|
Lustberg MB (2012). Management of Neutropenia in Cancer Patients. Clinical Advances in Hematology and Oncology 10(12):825-826.
|
|
|
|
|
Matthew VN, Sullivan O, Cai Y, Kong F, Zeng X, Gilbert GL (2006). Influence of Disk Separation Distance on Accuracy of the Disk Approximation Test for Detection of Inducible Clindamycin Resistance in Staphylococcus spp. Journal of Clinical Microbiology. 44(11):4072-4076.
Crossref
|
|
|
|
|
Nasehi L, Shahcheraghi F, Nikbin VS, Nematzadeh SH (2010). CTX-M, TEM and SHV Beta-lactamases In Clinical Isolates of Klebsiella pneumonia Isolated from Tahran, Iran. Iranian Journal of Basic Medical Sciences 13:111-118.
|
|
|
|
|
Steven MH, John IG (2008). Disorders of granulocytes and monocytes, chap 61. In: Fauci AS, Braunwald E, Isselacher KJ, Wilson JD, Martin JB, Kasper DL, Hauser SL, Longo DL, editors. Harrison's principles of internal medicine. 17. Singapore: Macgraw-Hill Book Co pp. 375–384.
|
|
|
|
|
Taj M, Farzana T, Shah T, Maqsood SS, Ahmed D, Shamsi TS (2015). Clinical and Microbiological Profile of Pathogens in Febrile Neutropenia in Hematological Malignancies: A Single Center Prospective Analysis. Journal of Oncology 2015(5):596504.
Crossref
|
|
|
|
|
Villafuerte Gutierrez P, Villalon L, Losa JE, Henriquez Camacho C (2014). Treatment of Febrile Neutropenia and Prophylaxis in Hematologic Malignancies: A Critical Review and Update. Advances in Hematology 2014:9.
Crossref
|
|
|
|
|
Viscoli C, Varnier O, Machetti M (2005). Infections in patients with febrile neutropenia: epidemiology, microbiology, and risk stratification. Clinical Infectious Diseases 40(Suppl 4):240-245.
Crossref
|
|
|
|
|
Yilmaz G, Aydin K, Iskender S, Caylan R, Koksal I (2007). Detection and prevalence of inducible clindamycin resistance in staphylococci. Journal of Medical Microbiology 56:342-345.
Crossref
|
|