ABSTRACT
Widespread use of Macrolide, lincosamide and Streptogramin B (MLSB) family of antibiotics in the treatment of Staphylococcus aureus (S. aureus) has led to an increased resistance to MLSB antibiotics. The purpose of this study was to determine the frequency of MLSB resistance among clinical isolates of methicillin sensitive S. aureus (MSSA) and Methicillin resistant S. aureus (MRSA) from Mansoura University Children Hospital (MUCH), Egypt, phenotypically by using D‑test and genotypically by detection of erm genes by PCR. Different microbiological samples were collected under complete aseptic condition from patients in MUCH according to the site of infection over a period of 9 months from March 2016 to November 2016. S. aureus isolates were identified using standard microbiological methods. MRSA was detected by growth on oxacillin screen agar plate and cefoxitin disk screen test. Antimicrobial susceptibility of the isolates was determined by Kirby-Bauer disk diffusion method. S. aureus isolates that were found to be erythromycin resistant were further studied for inducible clindamycin resistance using D-zone test according to CLSI recommendations. erm genes in S. aureus isolates were detected by PCR. Among 230 S. aureus isolates, 164 were MSSA (71.3%) and 66 were MRSA (28.7%). Twenty-five MSSA (15.2%), and 37 MRSA (56.1%) isolates were erythromycin resistant. Constitutive MLSB phenotype (cMLSB) (30.3 and 4.2%) and inducible MLSB phenotype (iMLSB) (22.7 and 7.9%) were observed in MRSA and MSSA, respectively by D-zone test. The rate of iMLSB phenotype and cMLSB phenotype in MRSA was significantly higher than in MSSA isolates. The frequency of ermA, ermB and ermC genes were 72.9, 5.4 and 13.5% in MRSA isolates and 60, 4 and 12% in MSSA isolates, respectively. Screening test for of iMLSB‑resistant strains is very important by double disk diffusion test (D‑test). This phenotypic test is simple, accessible and reliable method that can be done in every laboratory and research facility, without the need of costly genetic tests. Since the treatment of patients infected with S. aureus with iMLSB phenotype with clindamycin can lead to the expansion of constitutive resistance (cMLSB) and therapy failure.
Key words: Clindamycin, cMLSB, erm genes, iMLSB phenotype, MRSA, MSSA, S. aureus.
Methicillin resistance in Staphylococcus aureus (S. aureus) is an increasing problem in children and adult populations. MRSA is resistant to almost all beta-lactam antibiotics. Resistance to other antibiotics is also common, especially in hospital-acquired MRSA (Valle et al., 2016). Initially, MRSA was linked to infections associated to health care (hospital-acquired MRSA). Currently, MRSA represent a major problem in the community (Community-associated MRSA)( Nascimento et al., 2015). While the community-associated MRSA diseases are related to skin infections, the more severe clinical infections are more frequently related to hospitalized patients (Baddour et al., 2006).
Emergence of MRSA, has led to the enquiry of possible other antibiotics other than beta-lactam for staphylococcal infections treatment as erythromycin, clindamycin, gentamicin and ciprofloxacin (Valle et al., 2016). Macrolide (erythromycin), lincosamide (clindamycin) and Streptogramin B (MLSB) family of antibiotics is generally used in the treatment of staphylococcal infections; clindamycin is a good alternative in penicillin allergic patients in treatment of S. aureus infections. In addition, clindamycin has excellent oral bioavailability making it a good option for outpatient therapy and substitution after intravenous antibiotics. However, this widespread use has resulted in an increase in the number of Staphylococci strains resistant to MLSB antibiotics (Gherardi et al., 2009).
S. aureus and MRSA resistance to Macrolide antibiotic may be due to an active efflux mechanism encoded by msrA (encoding resistance to macrolides and Type B streptogramins only) or ribosomal target modification affecting macrolides, lincosamides, and Type B streptogramins (MLSB resistance) encoded by erm genes (Navaneeth, 2006). Three main erm (erythromycin ribosome methylation) genes, that is, erm(A), erm(B) and erm(C), have been defined in Staphylococci. They encode enzymes for inducible or constitutive resistance to MLSB agents through methylation of the 23S ribosomal RNA, thus reducing binding by MLSB agents to the ribosome (Martineau et al., 2000). In vitro, S. aureus isolates with constitutive resistance (cMLSB) are resistant to erythromycin and clindamycin, and isolates with inducible resistance (iMLSB) are resistant to erythromycin but appear to be susceptible to clindamycin. The risk for therapeutic failure is increased as cMLSB may rise from iMLSB during the course of clindamycin therapy in patients with severe Staphylococci infections Goudarzi et al., 2016).
Constitutive resistance can be readily detected, but inducible resistance is not detectable by routine antimicrobial susceptibility tests (Martineau et al., 2000).The double-disk diffusion test (D test) was recommended by Clinical and Laboratory Standards Institute (CLSI) as phenotypic method to screen for inducible resistance (CLSI, 2013). ermA, ermB and ermC among clinical isolates of S. aureus is detected by polymerase chain reaction (PCR) with specific primers as a genotypic method to confirm the presence of the MLSB genes. The purpose of our study was to determine the frequency of macrolide-lincosamide-streptogramin B (MLSB) resistance among clinical isolates of MSSA and MRSA from Mansoura University Children Hospital, Egypt, phenotypically by using D‑test and genotypically by detection of erm genes by PCR.
Isolation and identification of S. aureus
Different microbiological samples (wound swabs, pus, blood, urine, respiratory tract samples and fluid) were collected under complete aseptic condition from patients in MUCH according to the site of infection over a period of 9 months from March 2016 to November 2016. The samples were transported and processed in Microbiology Diagnostic and Infection Control unit (MDICU) in Medical Microbiology and Immunology Department, Faculty of Medicine, Mansoura University. Samples were inoculated on 5% sheep blood agar and Mac Conkey’s agar (Oxoid, UK), incubated at 37°C for 24-48 h, and examined for bacterial growth.
S.aureus isolates were identified by conventional biochemical tests (catalase, coagulase, DNase) and commercial identification system (API-STAPH; bioMérieux, Fance) (Gupta et al., 2009). Identical isolates from the same patient were not included in the study.
Detection of MRSA
MRSA was detected by growth on oxacillin screen agar plate containing 6 μg/ml of oxacillin in Mueller-Hinton agar supplemented with 4% NaCl and by cefoxitin disk screen test, using a 30 μg cefoxitin disc (Oxoid, UK). An inhibition zone diameter of ≤ 21 mm was reported as oxacillin or methicillin resistant and a zone diameter of ≥ 22 mm was considered sensitive according to the CLSI guidelines (CLSI, 2013).
Antimicrobial susceptibility testing
Kirby-Bauer disk diffusion method was used to determine Antimicrobial susceptibility of the isolates according to CLSI
guidelines. Briefly a 0.5 McFarland suspension of bacteria was prepared and inoculated on Mueller-Hinton’s agar plates (Oxoid, UK). The following antibiotic disks were used; penicillin (10U), amoxicillin-clavulanic acid (20/10 μg) cefoxitin (30 μg), gentamicin (10 μg), clindamycin (2 μg), erythromycin (15 μg), trimetoprim-sulfametoxazol (1.25/23.75 μg), ciprofloxacin (5 μg), tetracycline (30 ug) and rifampin (5 μg) (CLSI, 2013).
Vancomycin and oxacillin minimal inhibitory concentrations (MICs) were determined by E-Test (Bio Mérieux) according to CLSI guidelines.
S. aureus ATCC 25923 and S. aureus ATCC 29213 were used as standard strains and quality control for disk diffusion and MIC tests; respectively.
Disk approximation test with erythromycin and clindamycin (D-Zone test)
Erythromycin resistant S. aureus isolates were further studied for inducible clindamycin resistance by disk approximation test with erythromycin and clindamycin (D-zone test) according to CLSI guidelines. 0.5 McFarland suspensions was prepared from overnight growth of erythromycin resistant S. aureus. Then inoculated and spread over the surface on Mueller-Hinton agar plates (Merck, Germany). One erythromycin disk (15 μg) and one clindamycin disk (2 μg) were placed 15 mm distance from each other on the inoculated plates. Plates were incubated at 35°C and read after 18 h (Cetin et al., 2010).
According to the inhibition zone diameters, the isolate was considered to be:
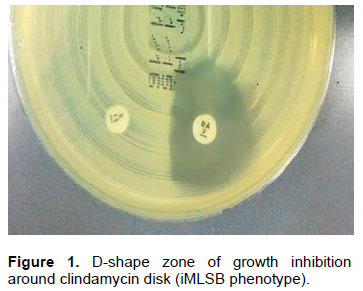
1) Macrolide-lincosamides streptogramin B inducible phenotype (iMLSB) (D test positive); if the isolate was erythromycin resistant and exhibited D-shaped inhibition zone around the clindamycin disc, (Figure 1).
2) Macrolide-lincosamides streptogramin B constitutive phenotype (cMLSB); if the isolate was resistant to both erythromycin and clindamycin.
3) Negative for inducible resistance (D test negative), but to have an active efflux pump (MSB); if the isolate was erythromycin resistant and clindamycin susceptible, with both zones of inhibition showing a circular shape (Bannerman et al., 2007).
DNA extraction
DNA was extracted from MRSA and MSSA isolates with macrolide- lincosamide-streptogramin (MLS) resistance using QIAamp® DNA Mini kits, QIAGEN (Germany) according to the producer's guidelines.
PCR for detection of erm genes
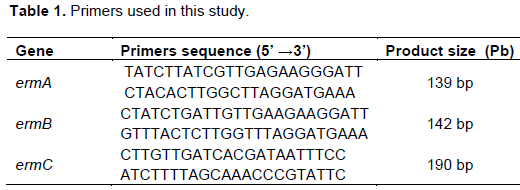
erm genes were amplified by PCR using specific primers for the erm A, B and C genes as exhibited in Table 1. Each reaction was performed in a final volume of 25 μL consisting of 5 μL of DNA template, 2.5 μL of PCR buffer (×10), 1 μL MgCl2 (50 mM), 0.5 μL of dNTPs (10 mM), 5 µM of each ermA, ermB and ermC forward
and reverse primers, 0.25 μL of Taq DNA polymerase (5 u/μL), 11.25 μL distill water.
PCR was achieved with the following reaction conditions: Initial denaturation at 94°C for 10 min, 35 cycles of denaturation at 94°C for 30 s, annealing at 53°C for 30 s, and extension at 72°C for 60 s, followed by a final extension at 72°C for 10 min (Coutinho et al., 2010).
Amplicons were analyzed after running on 2% agrose gel containing ethidium bromide in comparison to 50 bp molecular size standard ladder (Thermo Scientific Inc.).
Statistical analyses
Descriptive data were presented as frequencies and percentages via SPSS software version 18. Chi-square test was used to determine any significant differences between prevalence of the tested genes among S. aureus and MRSA strains. P value ≤ 0.05 was considered statistically significant.
Ethical Issues
This study was approved by Mansoura Faculty of Medicine, Egypt ethical committee (No: R/ 16.07.25). Written Informed consent was obtained from the guardian of each participant child. Privacy and confidentiality of personal information were saved and protected.
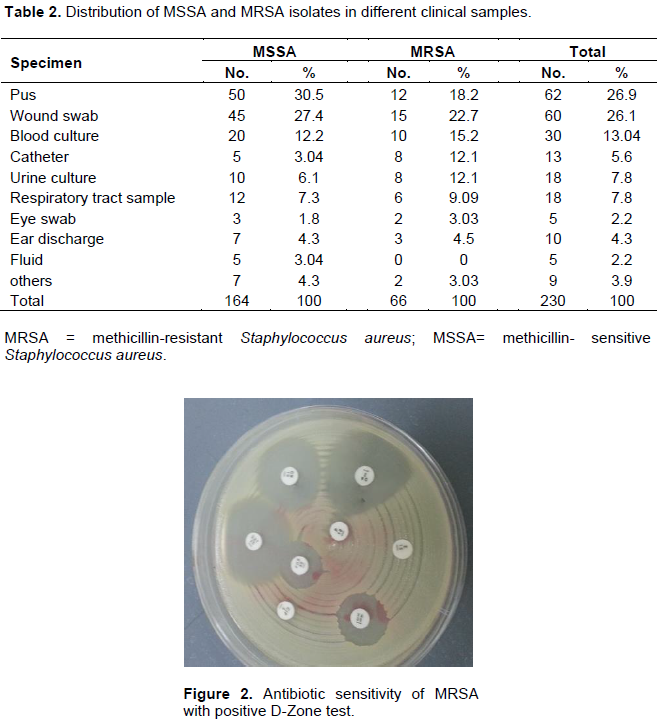
Two hundred and thirty (230) S. aureus isolates from different clinical samples were included in our study. 164 were MSSA (71.3%) and 66 were MRSA (28.7%).
MSSA and MRSA were most frequently isolated from Pus (26.9%), wound swab (26.1%), followed by blood culture (13.04) (Table 2). Twenty-five MSSA (15.2%), and 37 MRSA (56.1%) isolates were erythromycin resistant. Clinical isolates that displayed erythromycin resistance were tested for inducible resistance by D test (Figure 2).
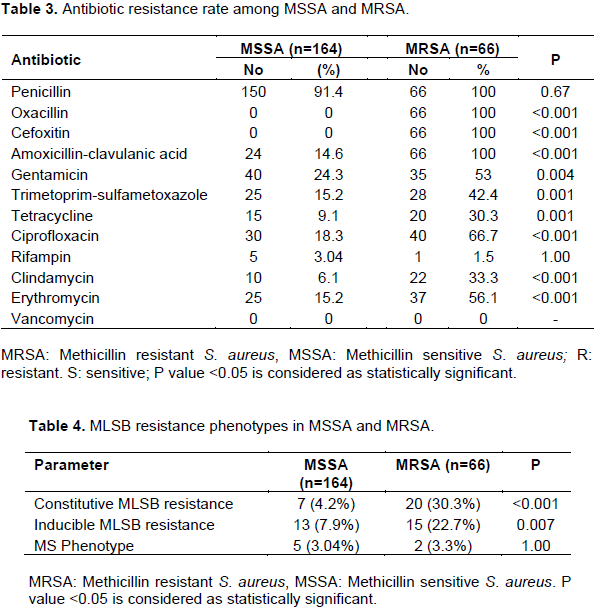
Antimicrobial resistance rate to gentamicin, trimetoprim-sulfametoxazole, ciprofloxacin and clindamycin showed statistically high significant differences between MRSA and MSSA isolates. Also, no antibiotic resistance was observed against vancomycin in both MRSA and MSSA (Table 3).Regarding D-zone test, cMLSB phenotype (30.3 and 4.2%), iMLSB phenotype (22.7 and 7.9%) and MS phenotype (3.3 and 3.04%) were observed in MRSA and MSSA, respectively (Table 4).
The rate of iMLSB phenotype and cMLSB phenotype was significantly higher in MRSA isolates; P value = 0.007 and P <0.001, respectively.
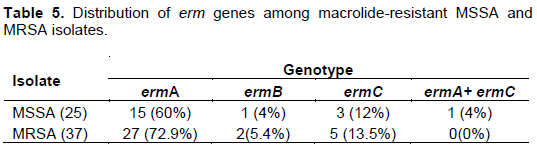
The frequency of ermA, ermB and ermC genes detected in MRSA and MSSA isolate were 72.9, 5.4, 13.5% and 60, 4, 12%, respectively (Table 5).
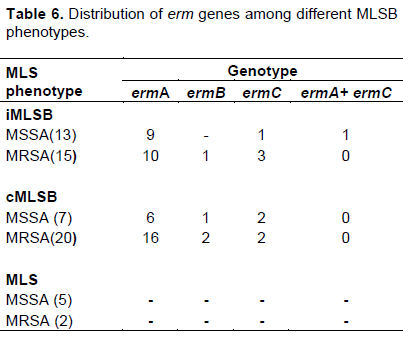
Distribution of erm genes among different MLSB phenotypes is as shown in Table 6.
Antimicrobial resistance is a worldwide problem, particularly among hospital acquired pathogens. Staphylococci have become one of the most common causes of both hospital acquired and community acquired infection (Navaneeth et al., 2006).
The increasing prevalence of methicillin resistance among Staphylococci resulted in renewed interest in the usage of Macrolide-Lincosamide-Streptogramin B (MLSB) antibiotics to treat S. aureus infections (Gupta et al., 2009).
Nevertheless, extensive usage of MLS B antibiotics has led to an increase in the number of Staphylococcal strains acquiring resistance to MLSB antibiotics (Cetin et al., 2010).
In the current study, 27.8% isolates were found to be MRSA that is comparable with a study conducted in Iran by Seifi et al. (2012). On contrary, higher result (48%) was reported by Ghanbari et al. (2016).
In the present study, erythromycin resistance was detected in 56.1 and 15.2% of MRSA and MSSA isolates, respectively. These results are in accordance with previous other studies (Ciraj et al., 2009; Prabhu et al., 2011).
In our study, cMLSB phenotype predominated over iMLSB phenotype in MRSA isolate (30.3% vs. 22.7%) that is similar to the finding of Gadepalli et al. (2006) and Dardi and Khare (2013).
Constitutive and inducible resistance clindamycin resistance phenotype was significantly higher in MRSA isolate as compared to MSSA isolate. Similar results were reported in other studies (Prabhu et al., 2011; Gadepalli et al., 2006; Dardi and Khare, 2013; Mahesh et al., 2013; Memariani et al., 2009). However, Schreckenberger et al. (2004) showed higher percentage of inducible resistance in MSSA as compared to MRSA.
Regarding MS phenotype, there was no statistical significance between MRSA and MSSA isolates. Erythromycin resistance in Staphylococci is encoded by erm genes. The frequency of erm A, erm B, erm C in MRSA and MSSA were 72.9, 5.4, 5% and 60, 4, 12%, respectively.
The frequency of erm genes is variable in different studies. In our study, erm A was the most frequent gene detected in MRSA (72.9%) and MSSA isolate (60%); this in accordance with study conducted by Saderi et al. (2011). Contrary to our result, erm C was the most common gene detected in other studies conducted in Iran, Turkey and Brazil (Ghanbari et al., 2016; Aktas et al., 2007; da Paz Pereira et al., 2016). Also, Zmantar et al. (2011) reported erm B was the most common genes detected from S. aureus isolates.
In accordance with another study conducted by Otsuka et al. (2007), our study showed that phenotypic method by D-test and genotypic detection of erm genes was in parallel for detection of macrolide resistance in S. aureus.
Since treatment of S. aureus infections with iMLSB phenotype by clindamycin can lead to the expansion of constitutive resistance (cMLSB) and therapy failure, screening test for iMLSB‑resistant strains is very essential by double disk diffusion test. This phenotypic test is a simple, accessible and reliable method that can be done in every laboratory and research facility, without the need of costly genetic tests.
The authors have not declared any conflict of interests.
REFERENCES
|
Aktas Z, Aridogan A, Kayacan CB, Aydin D (2007).Resistance to macrolide, lincosamide and streptogramin antibiotics in Staphylococci isolated in Istanbul, Turkey. J. Microbiol. 45:286-290.
|
|
|
|
Baddour MM, Abuelkheir MM, Fatani AJ (2006). Trends in antibiotic susceptibility patterns and epidemiology of MRSA isolates from several hospitals in Riyadh, Saudi Arabia. Ann. Clin. Microbiol. Antimicrob. 5(1):1.
Crossref
|
|
|
|
|
Bannerman TL, Peacock SJ. Staphylococcus, Micrococcus and other catalase-positive cocci. In: Murray PR, Baron EJ, Jorgensen JH, Landry ML, Pfaller MA, editors. Manual of clinical microbiology. 9th ed. Washington [DC]: ASM Press; 2007. Pp. 390-411.
|
|
|
|
|
Cetin ES, Gunes H, Kaya S, Aridogan BC, Demirci M (2010). Distribution of genes encoding resistance to macrolides, lincosamides and streptogramins among clinical staphylococcal isolates in a Turkish university hospital. J. Microbiol. Immunol. Infect. 43(6):524-529.
Crossref
|
|
|
|
|
Ciraj AM, Vinod P, Sreejith G, Rajani K (2009). Inducible clindamycin resistance among clinical isolates of staphylococci. Indian J. Pathol. Microbiol. 52:49-51.
Crossref
|
|
|
|
|
Clinical and Laboratory Standards Institute (CLSI) (2013). Performance Standards For Antimicrobial Susceptibility Testing, Twenty-Third Informational Supplement, M100-S21. Clin. Lab. Stand. Inst. 32:1-184.
|
|
|
|
|
Coutinho VD, Paiva RM, Reiter KC, de-Paris F, Barth AL, Machado AB (2010). Distribution of erm genes and low prevalence of inducible resistance to clindamycin among staphylococci isolates. Brazilian Journal of Infectious Diseases 14(6):564-568.
Crossref
|
|
|
|
|
da Paz Pereira JN, Rabelo MA, da Costa Lima JL, Neto AM, de Souza Lopes AC, Maciel MA (2016). Phenotypic and molecular characterization of resistance to macrolides, lincosamides and type B streptogramin of clinical isolates of Staphylococcus spp. of a university hospital in Recife, Pernambuco, Brazil. Braz. J. Infect. Dis. 20(3):276-81.
Crossref
|
|
|
|
|
Dardi CK, Khare AS (2013).Inducible clindamycin resistance in Staphylococcus aureus in a tertiary care rural hospital. Indian J. Basic Appl. Med. Res. 7(2):686-693.
|
|
|
|
|
Gadepalli R, Dhawan B, Mohanty S, Kapil A, Das BK, Chaudhry R (2006). Inducible clindamycin resistance in clinical isolates of Staphylococcus aureus. Indian J. Med. Res.123(4):571-573.
|
|
|
|
|
Ghanbari F, Ghajavand H, Havaei R, Jami MS, Khademi F, Heydari L, Shahin M, Havaei SA (2016). Distribution of erm genes among Staphylococcus aureus isolates with inducible resistance to clindamycin in Isfahan, Iran. Adv. Biomed. Res. 5
|
|
|
|
|
Gherardi G, De Florio L, Lorino G, Fico L, Dicuonzo G (2009). Macrolide resistance genotypes and phenotypes among erythromycin-resistant clinical isolates of Staphylococcus aureus and coagulase-negative staphylococci, Italy FEMS Immunol. Med.Microbiol. 55(1):62-67.
Crossref
|
|
|
|
|
Goudarzi G, Tahmasbi F, Anbari K, Ghafarzadeh M (2016). Distribution of Genes Encoding Resistance to Macrolides Among Staphylococci Isolated From the Nasal Cavity of Hospital Employees in Khorramabad, Iran. Iran. Red Crescent Med. J.18(2).
|
|
|
|
|
Gupta V, Datta P, Rani H, Chander J (2009). Inducible clindamycin resistance in Staphylococcus aureus: A study from North India. J. Postgrad. Med. 55(3):176.
Crossref
|
|
|
|
|
Mahesh CB, Ramakant BK, Jagadeesh VS (2013).The prevalence of inducible and constitutive clindamycin resistance among the nasal isolates of staphylococci. J. Clin. Diagn. Res. 7:1620-1622.
Crossref
|
|
|
|
|
Martineau F, Picard FJ, Lansac N, Ménard C, Roy PH, Ouellette M, Bergeron MG (2000). Correlation between the Resistance Genotype Determined by Multiplex PCR Assays and the Antibiotic Susceptibility Patterns of Staphylococcus aureus and Staphylococcus epidermidis. Antimicrob. Agents Chemother. 44(2):231-238.
Crossref
|
|
|
|
|
Memariani M, Pourmand MR, Shirazi MH, Soltan Dallal MM, Abdolsamadi Z, Mardani N (2009).The importance of inducible clindamycin resistance in enterotoxin positive S. aureus isolated from clinical samples. Tehran Univ. Med. J. 67:250-256.
|
|
|
|
|
Nascimento TC, Silva VL, Araújo ML, Campos MB, Ferreira-Machado AB, Ferreira DC, Oliveira MG, Diniz CG (2015). Epidemiology and antimicrobial susceptibility trends of methicillin-resistant Staphylococcus aureus in a tertiary hospital. Int. Arch. Med. 8.
Crossref
|
|
|
|
|
Navaneeth BV (2006). A preliminary in vitro study on inducible and constitutive clindamycin resistance in Staphylococcus aureus from a South Indian tertiary care hospital. Int. J. Infect. Dis.10(2):184-185.
Crossref
|
|
|
|
|
Otsuka T, Zaraket H, Takano T, Saito K, Dohmae S, Higuchi W, Yamamoto T (2007). Macrolide–lincosamide–streptogramin B resistance phenotypes and genotypes among Staphylococcus aureus clinical isolates in Japan. Clin. Microbiol. Infect. 13(3):325-327.
Crossref
|
|
|
|
|
Prabhu K, Rao S, Rao V (2011). Inducible clindamycin resistance in Staphylococcus aureus isolated from clinical samples. J. Lab. Phys. 3:25-27.
Crossref
|
|
|
|
|
Saderi H, Emadi B, Owlia P (2011). Phenotypic and genotypic study of macrolide, lincosamide and streptogramin B (MLSB) resistance in clinical isolates of Staphylococcus aureus in Tehran, Iran. Med. Sci. Monit. 17:BR48-BR53.
Crossref
|
|
|
|
|
Schreckenberger PC, Ilendo E, Ristow KL (2004). Incidence of constitutive and inducible clindamycin resistance in Staphylococcus aureus and coagulase-negative Staphylococci in a community and a tertiary care hospital. J. Clin. Microbiol. 42(6):2777-2779.
Crossref
|
|
|
|
|
Seifi N, Kahani N, Askari E, Mahdipour S, Naderi-Nasab M (2012). Inducible clindamycin resistance in Staphylococcus aureus isolates recovered from Mashhad, Iran. Iran. J. Microbiol. 4(2):82-86.
|
|
|
|
|
Valle DL, Paclibare PA, Cabrera EC, Rivera WL (2016). Molecular and phenotypic characterization of methicillin-resistant Staphylococcus aureus isolates from a tertiary hospital in the Philippines. Trop. Med. Health 44(1):1.
Crossref
|
|
|
|
|
Zmantar T, Kouidhi B, Miladi H, Bakhrouf A (2011). Detection of macrolide and disinfectant resistance genes in clinical Staphylococcus aureus and coagulase-negative staphylococci. BMC Res. Notes 4(1):453.
Crossref
|
|