Full Length Research Paper

ABSTRACT
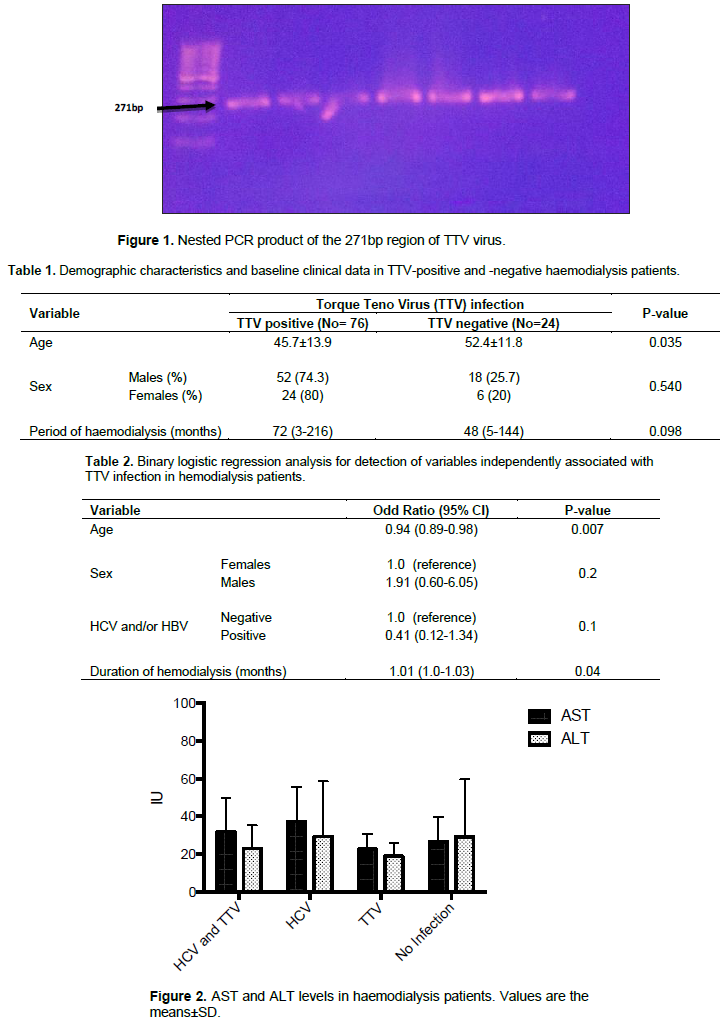
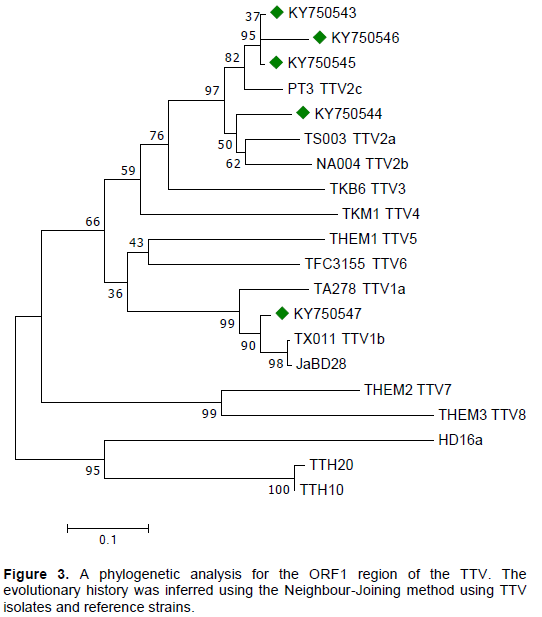
Very little reports are yet available for the infection rate of Torque Teno virus (TTV) among hemodialysis patients in Upper Egypt. Thus, the aim of this study was to assess the frequency and the possible genotypes of TTV in chronic renal failure patients undergoing dialysis. This cross-sectional study was carried out between August 2016 and February 2017 in three haemodialysis units in Minia, Egypt. Blood samples were collected for serological detection of Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV) and for detection of TTV. Nested polymerase chain reaction (PCR) was used to detect TTV. Isolates genotypes were identified by sequencing of the N22 region and phylogenetic analysis was also performed. Out of 100 dialysis patients, 76 were TTV positive (52 males and 24 females), with no significant association with gender. TTV was significantly more common among young adults than in older patients. Increased period of haemodialysis posed a high risk for acquiring TTV: Odd Ratio (OR) = 1 and 95% Confidence Interval (CI)= 1.01-1.03. No association was noted between TTV infection and either HCV or HBV infection. Genogroup 1, especially genotype 2 was the most frequently found type in hemodialysis patients. TTV is vastly predominant among Egyptian haemodialysis patients with no significant association with HCV or HBV. Further analyses are recommended to associate the renal failure outcome with the virus load.
Key words: Torque Teno virus, dialysis, phylogenetic biogeography.
INTRODUCTION
PATIENTS AND METHODS
RESULTS
DISCUSSION
CONCLUSION
The frequency of TTV is relatively high among dialysis patients, especially younger dialysis patients with no significant association with either sex, period of transfusion or HCV/HBV infection. Interestingly, genotype 2 was more frequently found than genotype 1 with high relationship between the viruses. Future measurement of the virus titre could help in evaluating the immunological status of dialysis patients.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abou-Donia H, Selim H, El-Koraei A, Ghazal A, Kabbary N (2007). TT virus DNA among hemodialysis patients in Alexandria. Egyptian Journal of Medical Microbiology 16:1-8. |
|
|
Akbari H, Piroozmand A, Dadgostar E, Nikoueinejad H, Chitsazian Z, Einollahi B, Mahabadi JAJ (2018). Prevalence of Transfusion-transmitted Virus (TTV) Infection and its Association with Renal Post-transplantation Complications in Iran. International Journal of Organ Transplantation Medicine 9:126. |
|
|
Al-Qahtani AA, Alabsi ES, AbuOdeh R, Thalib L, Nasrallah GK (2016). Prevalence of anelloviruses (TTV, TTMDV, and TTMV) in healthy blood donors and in patients infected with HBV or HCV in Qatar. Virology Journal 13:208. |
|
|
Amen N, Maria M, Azam M, Aziz A, Qamar R, Bostan NJTB (2018). Low Seroprevalence of Torque Teno Virus in HCV positive patients and phylogenetic analysis from Pakistani isolates. Tropical Biomedicine 35(1):205-220. |
|
|
Atwa ZT, Wahed WYA (2017). Transfusion transmitted infections in frequently transfused thalassemic children living in Fayoum Governorate, Egypt: Current prevalence and risk factors. Journal of Infection and Public Health 10:870-874. |
|
|
Brajao de Oliveira K (2015). Torque teno virus: a ubiquitous virus. Revista Brasileira de Hematologia e Hemoterapia 37:357-358. |
|
|
Chan YJ, Hsu YH, Chen MC, Wong WW, Wu JC, Yang WC, Liu CY (2000). TT virus infection among hemodialysis patients at a medical center in Taiwan. Journal of Microbiology, Immunology and Infection 33:14-18. |
|
|
Chen T, Vaisanen E, Mattila PS, Hedman K, Soderlund-Venermo M (2013). Antigenic diversity and seroprevalences of Torque teno viruses in children and adults by ORF2-based immunoassays. Journal of General Virology 94:409-417. |
|
|
Diniz-Mendes L, Devalle S, Niel C (2004). Genomic characterization of a Brazilian TT virus isolate closely related to SEN virus-F. Memórias do Instituto Oswaldo Cruz 99:301-306. |
|
|
Elzorkany KMA, Zahran A (2017). Hepatitis C virus status in hemodialysis patients in Menoufia Government, Egypt, five years apart: Do we have any improvement? Saudi Journal of Kidney Diseases and Transplantation 28:1126. |
|
|
Felsenstein J (1985). Confidence limits on phylogenies: an approach using the bootstrap. Evolution pp. 783-791. |
|
|
Focosi D, Antonelli G, Pistello M, Maggi F (2016). Torquetenovirus: the human virome from bench to bedside. Clinical microbiology and infection. The official publication of the European Society of Clinical Microbiology and Infectious Diseases 22:589-593. |
|
|
Gad A, Tanaka E, Orii K, Rokuhara A, Nooman Z, El-Hamid Serwah A, El-Sherif A, El-Essawy M, Yoshizawa K, Kiyosawa K (2002). Clinical significance of T.T. virus infection in maintenance hemodialysis patients of an endemic area for hepatitis C infection. Hepatology Research 22:13-19. |
|
|
Hassoba HMMMAGAA, Khudyakov YE (2005). TTV infection among hemodialysis patients in Egypt: relation to schistosomiasis and Hepatitis C virus co-infections. Molecular Diagnosis and Vaccines 3:1-9. |
|
|
Hassuna NA, Mohamed ZM, Abo-Eleuoon SM, Abdel-Hamid M (2015). Prevalence of Hepatitis B Virus (HBV), Hepatitis C Virus (HCV) Infections and their Co-infection among Blood Donors in Minia Governorate, Egypt. British Journal of Medicine and Medical Research 5:987. |
|
|
Hassuna NA, Naguib E, Abdel-Fatah M, Mousa SMO (2017). Phylogenetic Analysis of Torque Teno Virus in Thalassemic Children in Egypt. Intervirology 60:102-108. |
|
|
Hazanudin SN, Othman Z, Sekawi Z, Kqueen CY, Rasdi R (2019). Torque Teno Virus and Hepatitis: A review on correlation. Life Sciences, Medicine and Biomedicine 3(6). |
|
|
Hettmann A, Demcsák A, Bach Á, Decsi G, Dencs Á, Pálinkó D, Rovó L, Nagy K, Minarovits J, Takács M (2016). Detection and Phylogenetic Analysis of Torque Teno Virus in Salivary and Tumor Biopsy Samples from Head and Neck Carcinoma Patients. Intervirology 59:123-129. |
|
|
Hsiao K-L, Wang L-Y, Lin C-L, Liu H-F (2016). New Phylogenetic Groups of Torque Teno Virus Identified in Eastern Taiwan Indigenes. PloS one 11:e0149901. |
|
|
Irshad M, Mandal K, Singh S, Agarwal SK (2010). Torque teno virus infection in hemodialysis patients in North India. International Urology and Nephrology 42:1077-1083. |
|
|
Jalali H, Mahdavi MR, Zaeromali N (2017). Torque Teno Virus (TTV) Among beta-Thalassemia and Haemodialysis Patients in Mazandaran Province (North of Iran). International Journal of Molecular and Cellular Medicine 6:56-60. |
|
|
Kheradpezhouh M, Taremi M, Gachkar L, Aghabozorgi S, Khoshbaten M (2007). Presence and significance of transfusion-transmitted virus infection in Iranian patients on maintenance hemodialysis. Journal of Microbiology, Immunology and Infection 40:106-111. |
|
|
King AMQ, Adams MJ, Lefkowitz EJ (2011). Virus taxonomy: ninthreport of the international committee on taxonomy ofviruses. In. Amsterdam. Virus Taxonomy pp. 331-334. |
|
|
Kumar S, Stecher G, Tamura K (2016). MEGA7: Molecular Evolutionary Genetics Analysis version 7.0 for bigger datasets. Molecular Biology and Evolution 33(7):1870-1874. |
|
|
Maggi F, Andreoli E, Riente L, Meschi S, Rocchi J, Delle Sedie A, Vatteroni M, Ceccherini-Nelli L, Specter S, Bendinelli M (2007). Torquetenovirus in patients with arthritis. Rheumatology 46:885-886. |
|
|
Maggi F, Fornai C, Morrica A, Casula F, Vatteroni ML, Marchi S, Ciccorossi P, Riente L, Pistello M, Bendinelli M (1999). High prevalence of TT virus viremia in Italian patients, regardless of age, clinical diagnosis, and previous interferon treatment. Journal of Infectious Diseases 180:838-842. |
|
|
Maggi F, Pifferi M, Fornai C, Andreoli E, Tempestini E, Vatteroni M, Presciuttini S, Marchi S, Pietrobelli A, Boner A (2003). TT virus in the nasal secretions of children with acute respiratory diseases: relations to viremia and disease severity. Journal of Virology 77:2418-2425. |
|
|
Martinez NM, Garcia F, Garcia-Valdecasas J, Bernal C, Garcia Jr F, López I, Alvarez M, Piédrola G, Maroto MC (2000). Prevalence and viral persistence of TT virus in patients on hemodialysis. European Journal of Clinical Microbiology and Infectious Diseases 19:878-880. |
|
|
Najafimemar Z, Tabarraei A, Talei G, Moradi A (2018). Prevalence and Genotyping of Torque Teno Virus in HBV/HIV and Chronic HBV Patients in Iran. Iranian Biomedical Journal 22:338-344. |
|
|
Nishizawa T, Okamoto H, Konishi K, Yoshizawa H, Miyakawa Y, Mayumi M (1997). A novel DNA virus (TTV) associated with elevated transaminase levels in posttransfusion hepatitis of unknown etiology. Biochemical and Biophysical Research Communications 241:92-97. |
|
|
Peng J, Fang Y, Zhao X, Peng YJVS (2015). New prevalence estimate of Torque Teno virus (TTV) infection in healthy population and patients with chronic viral hepatitis in Jiujiang, China. Virologica Sinica 30:218-220. |
|
|
Saitou N, Nei M (1987). The neighbor-joining method: a new method for reconstructing phylogenetic trees. Molecular Biology and Evolution 4:406-425. |
|
|
Simonetta F, Pradier A, Masouridi-Levrat S, van Delden C, Giostra E, Morard I, Mueller N, Muellhaupt B, Valli PV, Semmo N, Seebach J, Chalandon Y, Kaiser L, Roosnek E (2017). Torque Teno Virus Load and Acute Rejection After Orthotopic Liver Transplantation. Transplantation 101:e219-e221. |
|
|
Spandole S, Cimponeriu D, Berca LM, Mihaescu G (2015a). Human anelloviruses: an update of molecular, epidemiological and clinical aspects. Archives of Virology 160:893-908. |
|
|
Spandole S, Cimponeriu D, Berca LM, Mihăescu G (2015b). Human anelloviruses: an update of molecular, epidemiological and clinical aspects. Archives of virology 160:893-908. |
|
|
Tamura K, Nei M, Kumar S (2004). Prospects for inferring very large phylogenies by using the neighbor-joining method. Proceedings of the National Academy of Sciences of the United States of America 101:11030-11035. |
|
|
Tanaka Y, Hayashi J, Ariyama I, Furusyo N, Etoh Y, Kashiwagi S (2000). Seroepidemiology of TT virus infection and relationship between genotype and liver damage. Digestive diseases and sciences 45:2214-2220. |
|
|
Utsunomiya S, Yoshioka K, Wakita T, Seno H, Takagi K, Ishigami M, Yano M, Watanabe K, Kobayashi M, Watanabe K, Kishimoto H, Kakumu S (1999). TT virus infection in hemodialysis patients. The American Journal of Gastroenterology 94:3567-3570. |
|
|
Vasilyev EV, Trofimov DY, Tonevitsky AG, Ilinsky VV, Korostin DO, Rebrikov DV (2009). Torque Teno Virus (TTV) distribution in healthy Russian population. Virology Journal 6:134. |
|
|
World Medical (2001). World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bulletin of the World Health Organization 79:373-374. |
|
|
Yokoyama H, Yasuda J, Okamoto H, Iwakura Y (2002). Pathological changes of renal epithelial cells in mice transgenic for the TT virus ORF1 gene. Journal of General Virology 83:141-150. |
|
|
Zuckerman M (2002). Surveillance and control of blood-borne virus infections in haemodialysis units. Journal of Hospital Infection 50:1-5. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


