ABSTRACT
Misuse of antibiotics in children is a major public health problem which may lead to increase antibiotic resistance in paediatric population. This study aims to evaluate parents’ knowledge and attitude toward antibiotic use in children with upper respiratory tract infections (URTIs) in the Western region of Saudi Arabia. A cross-sectional study was conducted using self-administered questionnaire on parents of school children. Statistical analysis was used to identify factors affecting parents’ knowledge and attitude toward antibiotic use. Of the 820 respondents, almost 98% agreed that misuse of antibiotics can lead to antibiotic resistance, and almost 74% stated that antibiotics are not useful for viral infections. However, 32.3% claimed that antibiotics can enhance the recovery from viral infections. Knowledge was better in Saudi than non-Saudi parents (p=0.001), parents with higher educational levels (p=0.00008), parents with higher monthly incomes (p=0.0001), and parents of children in private and international schools (p=0.0001). Almost 35% reported self-prescription of antibiotics for their children at least once, and about 13% self-prescribed leftover antibiotics. Positive attitude was reported in parents with high monthly income (p=0.0001), and parents whose children were in private or international schools (p=0.0001). There was no significant relation between positive attitude and parents’ nationality (p=0.114), nor educational levels (p=0.734). Good knowledge and positive attitude toward antibiotic use in children were reported in the Western region of Saudi Arabia. Future studies may be required to compare the current data to those after the ban of uncontrolled antibiotic prescription and dispensing in Saudi Arabia.
Key words: antibiotic, misuse, knowledge, attitude, Saudi Arabia, antimicrobial resistance, upper respiratory tract, infection.
Antimicrobial resistance (AMR) has become a major threat to health in both humans and animals in most parts of the world (Zowawi, 2016). Since the early discovery of antimicrobial agents in the last century, millions of
infected patients were cured after been treated with antimicrobial agents. However, the increasing resistance rates of most serious bacterial pathogens to these agents have limited the choices of treatment to few types of antimicrobials, making treatment of diseases caused by resistant pathogens more difficult. The use of antibiotics forces the exposed bacteria to generate mutations to overcome the effective mechanism of the antibiotic and become resistant (Zowawi et al., 2015). Many factors contribute in increasing AMR, including overuse and misuse of antibiotics, and self-medication (Austin et al., 1999; Steinke and Davey, 2001; Nepal and Bhatta, 2018). Several studies discussed the increase of AMR by various bacterial pathogens. These include taking insufficient dosage, noncompliance with treatment plan, using leftover medications, excessive use of antibiotics without medical advice, and taking antibiotics for viral infections (Levin, 2001; Alhomoud et al., 2017).
The threat of antibiotic resistance is now becoming more obvious and requires an implementation of a prompt global action plan to limit this resistance. The World Health Organization (WHO) in one of its recent reports stated that the world is directed to a ‘post-antibiotic era’, where common minor infections can be life-threatening (World Health Organization, 2015).
In children, inappropriate use of antibiotics is known to increase resistance in the paediatric population (Ab Rahman et al., 2016; Keohavong et al., 2019). Moreover, frequent exposure to antibiotics during childhood has been linked to unfavourable long-term metabolic problems, such as obesity and diabetes (Bailey et al., 2014; Boursi et al., 2015; Turta and Rautava, 2016). Commonly, antibiotics are inappropriately given to children with non-specific symptoms, urinary tract infections (UTIs), unexplained abdominal pain or upper respiratory tract infections (URTIs) (Gieteling et al., 2011; Ab Rahman et al., 2016; Jayaweera and Reyes, 2018). About 80% of URTIs in children are caused by viruses (Mahony, 2008). Therefore, excessive treatments with antibiotics may not be effective for most cases. A number of factors contribute in the misuse of antibiotics in children including lack of parents knowledge regarding antibiotic use, underestimation of the consequences of long-term resistance to antibiotics by physicians, physicians’ perception of being parents’/parents’ expectations, their fear of probable complications (Lopez-Vazquez et al., 2012), and self-medication, especially in countries that have no regulations to control pharmacies for dispensing antibiotics without prescriptions (World Health Organization, 2014). Self-medication with over-the-counter (OTC) medication is an acceptable practice globally. However, buying prescription medication without seeking medical consultation can be unsafe and dangerous self-medication (Aljadhey et al., 2015). The availability and non-restricted access to antibiotics as an OTC medication in community pharmacies in some countries can be linked to increase the risk of self-medication. Studies showed that self-medication is a common practice in developing countries, and antibiotics can be easily obtained without prescription (Sakeena et al., 2018; Zawahir et al., 2018). A study in Saudi Arabia revealed that 35% of patients visiting primary care centers have experienced self-medication (Alghanim, 2011). Another study in the Eastern region of Saudi Arabia reported that 67% of the parents tried self-medication once or more, and 37.7% of them used leftovers antibiotics (Al-Shawi et al., 2018). Fortunately, in early 2018, the Saudi Ministry of health regulated antibiotic dispensing protocols by the Executive Regulations of Health Practice Law, which prohibits pharmacists from dispensing any drug without a prescription issued by a doctor with a license to practice in the Kingdom.
Limited information regarding antibiotic use in Saudi children is known, particularly those with URTIs. To my best knowledge, no previous study was done on parents in the Western region of Saudi Arabia. As far as the use of antibiotics in children depends on their parents’ knowledge, awareness and attitude toward the correct use of these medications, this study aims to assess the level of parents’ knowledge and attitude toward antibiotic use in URTIs in the western region of Saudi Arabia.
Study design, data collection and analysis
A cross-sectional study using self-administered questionnaire was conducted between the period of May and July 2018. A total of 820 participants responded to this study. All participants were parents of school children from the Western Region of Saudi Arabia. The inclusion criteria were that participants had to be parents of children who attended, or have attended schools, and should be residents in the Western Region of Saudi Arabia. A structured, self‑administered questionnaire was designed based on recent literature reviews. The questionnaire was spread electronically via e-mails or through other social media platforms. To avoid duplication of participants’ responses, unique national identification number had to be submitted in the questionnaire, which was anonymized during and after the survey. An informed consent form was electronically attached to the questionnaire and had to be checked prior to start answering the questionnaire.
The questionnaire contained three sections; the first started with an introductory statement about the aim of the study and appreciation for participants. The second section was designed to collect demographic data of the participants. The third contained open- and close-ended questions to report participants’ knowledge, awareness and attitude toward antimicrobial use for URTI in children. In the demographic section, participants were asked to provide their age, gender, nationality, marital status, number of children, educational level, job title, monthly income and school type of their children. The knowledge and attitude section of the questionnaire was used to assess parents’ knowledge and attitude toward antibiotic use for URTI. Participants’ knowledge was assessed by asking 8 questions that require yes or no answers. To measure the participants’ knowledge a scoring system ranged from 1 to 8 was designed. A value one was given to the correct response, and a value of zero to each incorrect response. Participants’ knowledge was classified into three categories; poor knowledge for those who answered 0-2 questions correctly, intermediate for those who answered 3-5 questions correctly, and good knowledge for those who answered 6-8 questions correctly. The responses were quantitated and total score of knowledge was measured. Participants’ attitude toward antibiotic use in URTI was measured by asking 7 questions. The responses to the first five of these questions were scored as the following; 2 = never, 1 = sometimes, and 0 = always. The scores were inverted for the remaining two questions. The responses were quantitated and total score of attitude was measured. The total attitude score ranged from 0-14. A score of ≤ 7 represented negative attitude, while a score of > 7 represented positive attitude toward antibiotic use in URTI. Scoring scales were adapted from a previous study (Al-Shawi et al., 2018) with some modifications to fit the requirements of our questionnaire. Data were maintained confidential throughout the study. Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, USA) version 21 was used to analyse the study data. Descriptive statistics were used to demonstrate respondents’ demographic characteristics. The relations between categorical variables were determined using Mann-Whitney U test.
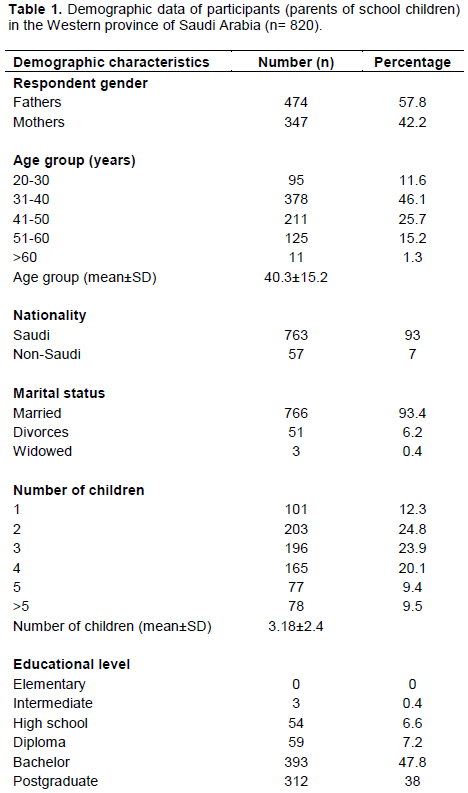
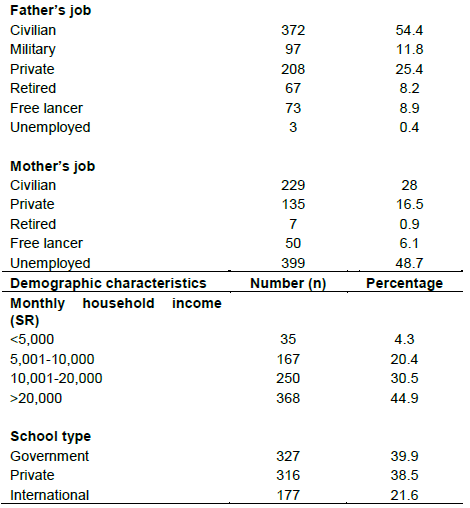
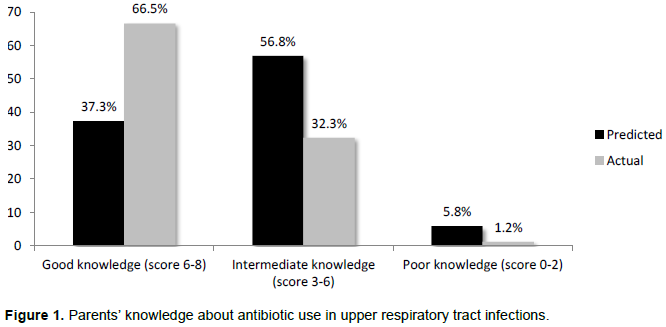
A total of 820 parents of school children completed the questionnaire, of whom 474 (57.8%) were fathers and 347 (42.2%) were mothers. The age group of most of participants was 31-40 (46.1%), followed by age group of 41-50 (25.7%), whereas the minority were above 60 years old (1.3%). The majority of respondents were Saudis (93.4%), and mostly were highly educated with Bachelor or higher degrees (85.8%). About 75% of the respondents’ household monthly income was higher than 10,000 Saudi Riyals (SR). Sociodemographic data of the respondents is summarized in Table 1. A high percentage of respondents (95.7%, n=784) answered correctly by stating that antibiotic misuse can result in developing bacterial generations that are resistant to antibiotics, and antibiotics are not useful to treat viral infections such as seasonal flu and common cold (73.8%, n=605). Almost two-third (61%, n=500) agreed that the most common causative agent for URTIs are viruses, and more than half (54%, n=443) agreed that URTIs can be cured without antibiotics. Nevertheless, about one-third of the respondents (32.3%, n=256) believed that antibiotics can enhance the recovery from viral infections. About 10% (n=85) only agreed that antibiotics can be stopped once the progression is noticed without the need for completing the course (Figure 2). Parents’ knowledge about antibiotic use in children with URTIs varied from poor to good. About 37% (n=306) of parents claimed that they have good knowledge, whereas more than half (57%, n=466) stated they have intermediate knowledge, and only 5.8% (n=47) acknowledged their poor knowledge (Figure 1).
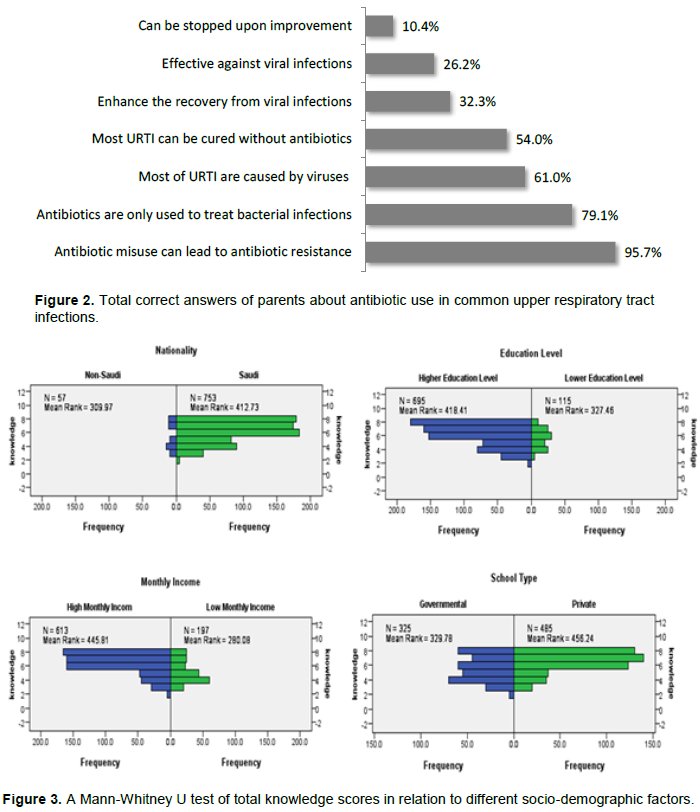
According to the total score of parents’ knowledge, 66.5% (n=545) of parents have good knowledge (score 6-8) about antibiotic use in URTIs, 32.3% (n=265) have intermediate knowledge (score 3-6), while only 1.2% (n=10) were shown to have poor knowledge (score 0-3) (Figure 1). A Mann-Whitney U test was performed to determine whether the differences in the knowledge scores are statistically significant in relation to different socio-demographic factors of parents. Higher knowledge scores were found in Saudi than non-Saudi parents (p = 0.001), parents with higher educational levels (p = 0.00008), parents with higher monthly incomes (p = 0.0001), and parents whose children were in private and international schools (p = 0.0001). These differences were statistically significant. Figure 3 summarizes the significant differences of knowledge scores in relation to different socio-demographic factors.
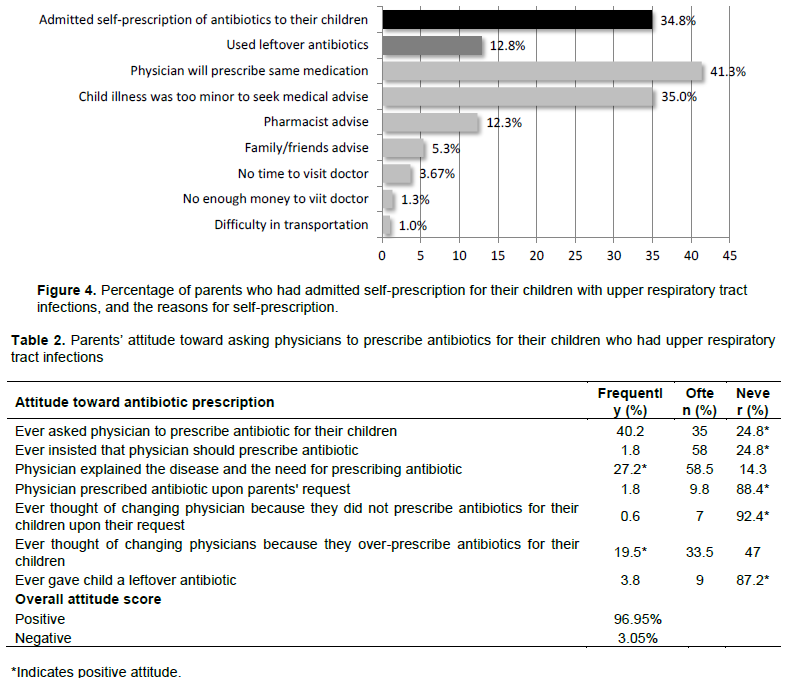
Almost 35% (n=285) of parents reported self-prescription of antibiotics for their children at least once, and about 13% (n=105) of them self-prescribed leftover antibiotics for their children. Many reasons were reported for self-prescription. The most common was that they already knew that physician will prescribe the same medication. The next common reason was that the symptoms were too minor to take the child to hospital, followed by that the antibiotic was given according to pharmacist’s advice (Figure 4).
In regards to different parents’ attitude toward asking physicians to prescribe antibiotics, about 75% stated they asked their physicians to prescribe antibiotics for their children at least once, and minority of them had insisted on it. About 10% of physicians prescribed antibiotics upon parents’ requests. In more than 85% of the cases, the physician explained whether the child needs an antibiotic for current illness. A very minor percentage thought of changing their physicians because they do not prescribe antibiotics upon their requests, while more than half thought to change physicians because they over-prescribe antibiotics for their children. According to the attitude score, almost 97% of parents had positive attitude toward antibiotic use in URTIs (Table 2).
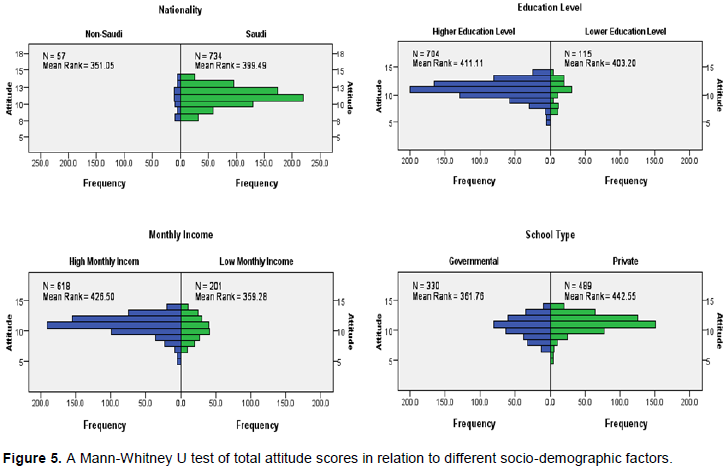
To determine if the differences in the attitude scores are statistically significant in the in relation to different socio-demographic factors of parents, Mann-Whitney U test was performed. There was a significant relation between positive attitude and high monthly income (p = 0.0001), and between positive attitude and parents whose children were in private or international schools (p = 0.0001). However, there was no significant relation between positive attitude and parents’ nationality (p = 0.114), nor educational levels (p = 0.734) (Figure 5).
In this study, the parental knowledge and attitude toward antibiotic use in URTIs was examined in the Western region of Saudi Arabia. The results show that some parents have misconception and poor to intermediate knowledge about antibiotic uses in children. The reported knowledge score shows that about two-third (66.5%) of parents has good knowledge toward antibiotic use in children with URTIs. Similar to the literature, the findings of this study shows that parents’ lower education, monthly income, and type of school were the main factors associates with poor knowledge toward antibiotic use in children (You et al., 2008; Togoobaatar et al., 2010; Rousounidis et al., 2011; Panagakou et al., 2012; Abobotain et al., 2013; Al-Shawi et al., 2018).
The majority of parents involved in this study admitted that antibiotic misuse can lead to antibiotic resistance (95.7%). This finding is much higher the ones reported in other studies in Saudi Arabia, and Hong Kong (You et al., 2008, Al-Shawi et al., 2018). Almost one-third of our respondents agreed that antibiotics can reduce symptoms and increase recovery from viral infections. A higher percentage (57.7%) was reported in the central region of Saudi Arabia (Abobotain et al., 2013). In addition, other studies reported high percentages of respondents claimed that antibiotic can accelerate the recovery of URTI (Rousounidis et al., 2011; Yu et al., 2014; Al-Shawi et al., 2018). Only around 10% of respondents believed that it is not required to complete the course once recovery is noticed. Higher percentages were reported in Riyadh (28.7%) (Abobotain et al., 2013), and Hong Kong (42%) (You et al., 2008).
Self-medication has been studied extensively worldwide. In more than a decades, a study conducted in Tanzania in 2004 (Kagashe and Francis, 2004) reported that 37% of medications that were bought from community pharmacies were prescription-only medication. A decade later, in a recent study in Riyadh (2015), the percentage increased to 49% (Aljadhey et al., 2015). More than one-third of parents in this study (34.8%) admitted self-prescription of antibiotics for their children. Similar findings were reported in an urban Chinese area (36%) (Bi et al., 2000), while a higher percentage was reported in a study conducted in a rural Chinese area in 2014 (62%) (Yu et al., 2014), and Eastern region of Saudi Arabia (56.9%) (Al-Shawi et al., 2018), whereas a lower percentage was reported in Greece (23%) (Edwards et al., 2002). In our study, parents explained the main reasons of self-prescription as that physician will prescribe the same medication, and their children had minor illnesses that do not require hospital visit. Our findings were consistent with other studies in Saudi Arabia (Al-Shawi et al., 2018), Bahrain (James et al., 2006), Magnolia (Togoobaatar et al., 2010), Vietnam (Le et al., 2011), and China (Bi et al., 2000), in which less severe illnesses were the main reason for giving antibiotics to children. These reasons contradict with other findings in studies conducted in developing countries where low cost of antibiotics was considered as the main reason for self-medication (Saradamma et al., 2000; Suleman et al., 2009).
In our study, about three-quarters of parents requested antibiotics for their children at least once. This finding is higher than those reported in other studies in Saudi Arabia (Al-Shawi et al., 2018), and China (Yu et al., 2014). A very minor percentage (7.6%) thought of changing their physicians because they do not prescribe antibiotics upon their requests. Low percentages were also reported in Saudi Arabia (Al-Shawi et al., 2018) and Cyprus (Rousounidis et al., 2011). The majority of parents (88.4%) admitted that physicians did not prescribe antibiotics upon their request, and the majority of physicians (75.7%) explained the disease and the need for prescribing antibiotics; which is also similar to another Saudi study (Al-Shawi et al., 2018).
The use of leftover antibiotics is a part of antibiotic misuse, and can be a major source of increasing antibiotic resistance. The easy access to antibiotics in community pharmacies in Saudi Arabia, as many other Middle Eastern countries plays an important role in increasing the availability of the drug at homes. Over-prescription by physicians, dispensing prescription medication without prescription by pharmacists, or non-compliance with treatment dose by patients, are all involved in facilitating the use of leftover antibiotics (You et al., 2008; Togoobaatar et al., 2010; Abobotain et al., 2013). Therefore, it is important for physicians to prescribe exact doses that are required by patients, advice patients to complete the antibiotic course, and discard any excess drugs. Our study revealed that 12.8% of parents used leftover antibiotics for their children, which is similar to the finding of another Saudi study (Al-Shawi et al., 2018).
Although health services are mostly free for all citizens in Saudi Arabia, the availability of antibiotics has not been regulated until early 2018, where the Saudi Ministry of health sets regulatory protocols for antibiotic prescription by the Executive Regulations of Health Practice Law, which prohibit pharmacists from dispensing any drug without a prescription issued by a doctor with a license to practice in the Kingdom. Therefore, further studies are required to compare the status of parents’ knowledge and attitude toward antibiotic use after these regulations come into force.
This study revealed good knowledge and positive attitude toward antibiotic use in URTI in Children in parents in the Western region of Saudi Arabia. Emphasis to run more educational health programs about antibiotic use is needed, especially for parents who have children attending schools. Training for healthcare providers and pharmacists about proper antibiotic prescription should be considered to collaborate in increasing public awareness of antibiotic use, rather than only prescribing antibiotics. Running campaign in public areas should also be considered to improve the relationship between patients and healthcare providers for proper delivery and increasing the awareness of antibiotic use.
The authors have not declared any conflict of interests.
REFERENCES
|
Ab Rahman N, Teng CL, Sivasampu S (2016). Antibiotic prescribing in public and private practice: a cross-sectional study in primary care clinics in Malaysia. BMC Infectious Diseases 16:208.
Crossref
|
|
|
|
Abobotain AH, Sheerah HA, Alotaibi FN, Joury AU, Mishiddi RM, Siddiqui AR, Saeed AB (2013). Socio-demographic determinants of antibiotic misuse in children. A survey from the central region of Saudi Arabia. Saudi Medical Journal 34(8):832-840.
|
|
|
|
Al-Shawi MM, Darwish MA, Wahab MM, Al-Shamlan NA (2018). Misconceptions of Parents about Antibiotic use in Upper Respiratory Tract Infections: A survey in Primary Schools of the Eastern Province, KSA. Journal of Family and Community Medicine 25(1):5-12.
|
|
|
|
Alghanim SA (2011). Self-medication practice among patients in a public health care system. Eastern Mediterranean Health Journal 17(5):409-416.
Crossref
|
|
|
|
Alhomoud F, Aljamea Z, Almahasnah R, Alkhalifah K, Basalelah L, Alhomoud FK (2017). Self-medication and self-prescription with antibiotics in the Middle East-do they really happen? A systematic
Crossref
|
|
|
|
review of the prevalence, possible reasons, and outcomes. International Journal of Infectious Diseases 57:3-12.
|
|
|
|
Aljadhey H, Assiri GA, Mahmoud MA, Al-Aqeel S, Murray M (2015). Self-medication in Central Saudi Arabia Community pharmacy consumers' perspectives. Saudi Medical Journal 36(3):328-334.
Crossref
|
|
|
|
Austin DJ, Kristinsson KG, Anderson RM (1999). The relationship between the volume of antimicrobial consumption in human communities and the frequency of resistance. Proceedings of the National Academy of Sciences 96(3):1152-1156.
Crossref
|
|
|
|
Bailey LC, Forrest CB, Zhang P, Richards TM, Livshits A, DeRusso PA (2014). Association of antibiotics in infancy with early childhood obesity. JAMA Pediatrics 168(11):1063-1069.
Crossref
|
|
|
|
Bi P, Tong S, Parton KA (2000). Family self-medication and antibiotics abuse for children and juveniles in a Chinese city. Social Science and Medicine 50(10):1445-1450.
Crossref
|
|
|
|
Boursi B, Mamtani R, Haynes K, Yang YX (2015). The effect of past antibiotic exposure on diabetes risk. European Journal of Endocrinology 172(6):639-648.
Crossref
|
|
|
|
Edwards DJ, Richman PB, Bradley K, Eskin B, Mandell M (2002). Parental use and misuse of antibiotics: are there differences in urban vs. suburban settings? Academic Emergency Medicine 9(1):22-26.
Crossref
|
|
|
|
Kagashe GA, Francis L (2004). Dispensing of drugs with and without a prescription from private pharmacies in Dar es Salaam. Tanzania Medical Journal 19(1):36-39.
Crossref
|
|
|
|
Gieteling MJ, Lisman-van Leeuwen Y, van der Wouden JC, Schellevis FG, Berger MY (2011). Childhood nonspecific abdominal pain in family practice: incidence, associated factors, and management. Annals of Family Medicine 9(4):337-343.
Crossref
|
|
|
|
James H, Handu SS, Al Khaja KA, Otoom S, Sequeira RP (2006). Evaluation of the knowledge, attitude and practice of self-medication among first-year medical students. Medical Principles and Practice 15(4):270-275.
Crossref
|
|
|
|
Jayaweera JA, Reyes M (2018). Antimicrobial misuse in pediatric urinary tract infections: recurrences and renal scarring. Annals of Clinical Microbiology and Antimicrobials 17(1): 27.
Crossref
|
|
|
|
Keohavong B, Vonglokham M, Phoummalaysith B, Louangpradith V, Inthaphatha S, Kariya T, Saw YM, Yamamoto E, Hamajima N (2019). Antibiotic prescription for under-fives with common cold or upper respiratory tract infection in Savannakhet Province, Lao PDR. Tropical Medicine and Health 47(1):16.
Crossref
|
|
|
|
Le TH, Ottosson E, Nguyen TK, Kim BG, Allebeck P (2011). Drug use and self-medication among children with respiratory illness or diarrhea in a rural district in Vietnam: a qualitative study. Journal of Multidisciplinary Healthcare 4:329-336.
Crossref
|
|
|
|
Levin BR (2001). Minimizing potential resistance: a population dynamics view. Clinical Infectious Diseases 33 (Supplement 3):S161-169.
Crossref
|
|
|
|
Lopezâ€Vazquez P, Vazquezâ€Lago JM, Figueiras A (2012). Misprescription of antibiotics in primary care: a critical systematic review of its determinants. Journal of Evaluation in Clinical Practice 18(2):473-484.
Crossref
|
|
|
|
Mahony JB (2008). Detection of respiratory viruses by molecular methods. Clinical Microbiology Reviews 21(4):716-747.
Crossref
|
|
|
|
Nepal G, Bhatta S (2018). Self-medication with Antibiotics in WHO Southeast Asian Region: A Systematic Review. Cureus 10(4):e2428.
Crossref
|
|
|
|
Panagakou SG, Papaevangelou V, Chadjipanayis A, Syrogiannopoulos GA, Theodoridou M, Hadjichristodoulou CS (2012). Risk factors of antibiotic misuse for upper respiratory tract infections in children: results from a cross-sectional knowledge-attitude-practice study in Greece. ISRN Pediatrics 2012:685302.
Crossref
|
|
|
|
Rousounidis A, Papaevangelou V, Hadjipanayis A, Panagakou S, Theodoridou M, Syrogiannopoulos G, Hadjichristodoulou C (2011). Descriptive study on parents' knowledge, attitudes and practices on antibiotic use and misuse in children with upper respiratory tract infections in Cyprus. International Journal of Environmental Research and Public Health 8(8):3246-3262.
Crossref
|
|
|
|
Sakeena MH, Bennett AA, McLachlan AJ (2018). Non-prescription sales of antimicrobial agents at community pharmacies in developing countries: a systematic review. International Journal of Antimicrobial Agents 52(6): 771-782.
Crossref
|
|
|
|
Saradamma RD, Higginbotham N, Nichter M (2000). Social factors influencing the acquisition of antibiotics without prescription in Kerala State, south India. Social Science and Medicine. 50(6): 891-903.
Crossref
|
|
|
|
Steinke D, Davey P (2001). Association between antibiotic resistance and community prescribing: a critical review of bias and confounding in published studies. Clinical Infectious Diseases 33(Supplement 3):S193-205.
Crossref
|
|
|
|
Suleman S, Ketsela A, Mekonnen Z (2009). Assessment of self-medication practices in Assendabo town, Jimma zone, southwestern Ethiopia. Research in Social and Administrative Pharmacy 5(1):76-81.
Crossref
|
|
|
|
Togoobaatar G, Ikeda N, Ali M, Sonomjamts M, Dashdemberel S, Mori R, Shibuya K (2010). Survey of non-prescribed use of antibiotics for children in an urban community in Mongolia. Bulletin of the World Health Organization 88(12):930-936.
Crossref
|
|
|
|
Turta O, Rautava S (2016). Antibiotics, obesity and the link to microbes - what are we doing to our children? BMC Medicine 14(1):57.
Crossref
|
|
|
|
World Health Organization (2014). Antimicrobial resistance: Global report on surveillance 2014.
View
|
|
|
|
World Health Organization. (2015). Global action plan on antimicrobial resistance.
View
|
|
|
|
You JH, Yau B, Choi KC, Chau CT, Huang QR, Lee SS (2008). Public knowledge, attitudes and behavior on antibiotic use: a telephone survey in Hong Kong. Infection 36(2):153-157.
Crossref
|
|
|
|
Yu M, Zhao G, Lundborg CS, Zhu Y, Zhao Q, Xu B (2014). Knowledge, attitudes, and practices of parents in rural China on the use of antibiotics in children: a cross-sectional study. BMC Infectious Diseases 14:112.
Crossref
|
|
|
|
Zawahir S, Lekamwasam S, Aslani P (2018). Antibiotic dispensing practice in Sri Lankan community pharmacies: A simulated client study. Research in Social and Administrative Pharmacy, 2018.
Crossref
|
|
|
|
Zowawi HM (2016). Antimicrobial resistance in Saudi Arabia. An urgent call for an immediate action. Saudi Medical Journal 37(9): 935-940.
Crossref
|
|
|
|
Zowawi, HM, PN Harris, MJ Roberts, PA Tambyah, MA Schembri, MD Pezzani, DA Williamson and DL Paterson (2015). The emerging threat of multidrug-resistant Gram-negative bacteria in urology. Nature Reviews Urology 12(10):570-584.
Crossref
|