ABSTRACT
Pharyngitis is an inflammation or irritation of the pharynx or palatine tonsil. The etiology is usually viruses which cause the majority of the pharyngitis but most bacterial cases are attributed to group A Streptococci (GAS). This study aimed to identify the frequency of bacterial pharyngitis especially GAS of children, according to epidemiological factors. Symptoms present and signs for each patient were recorded, following which a throat swab was collected. There were 237 cases of children aged between 1 and 14 years with inflammation; out of 394 cases that visited the ENT primary care at Souk Al-Kameess during the 12 months study period. From the incidence of 394 sore throat cases, GAS was observed in 237 cases (60.15%). Of these 110 (46.41%) were girls and 127 (53.59%) were boys. A higher proportion of children were found with GAS pharyngitis aged 5-9 and the lowest incidence of sore throat occurrence was 3-4 years. The highest incidence of children pharyngitis was recorded in January (Winter) and September (Autmn). The following factors showed independent positive correlation with GAS sore throat infection; patients visiting, months, year season, tonsillectomy, culture result, catalase test result and bacitracin test result with significant value of P<0.01, whereas sex, age and gram stain results with P˃ 0.01. In conclusion, the results of this study found that cases of bacterial sore throat were higher than non-bacterial sore throat. The main cause of bacterial pharyngitis was GAS. Therefore, this study suggested that the use of the effectiveness of antibiotics and recommended anti-bacterial pharyngitis therapy to prevent initial rheumatic fever and its complications.
Key words: Pharyngitis, tonsillitis, epidemiological factors, Streptococcus, children.
The most common etiology for Pharyngitis is by viral upper respiratory transmission. However, inflammatory processes of the nasopharynx are pharyngitis and tonsillitis can be caused by bacteria (Lin et al., 2003). The bacteria that cause pharyngitis and tonsillitis are beta-hemolytic Streptococcus
and Staphylococcus aureus
(Bhalla et al., 2019). Bacteria cause erythema of the nasopharynx mucosa along with an exudative membrane (Leung and Kellner, 2004).
Most bacterial cases are due to group A Streptococci (GAS) infection (Van Schoor, 2013). Other causes include allergic reaction, trauma, toxin and neoplastic (Hildreth et al., 2015). Symptoms may include a sore throat, fever, headache and a hoarse voice (Rutter and Newb, 2015). Gonorrhea, fungus, irritants such as smoke, allergies and gastro esophageal reflux cause Pharyngitis. Pharyngitis occurs mostly by people contact with nasal discharge, rather than by oral contacts (Kirkpatrick, 1996). Approximately 7.5% of people have a sore throat in any full three-months (Principi et al., 2013).
Identifying the cause of pharyngitis, especially group A Beta-Hemolytic Streptococcus (GABHS), is important to prevent the potentially life-threatening complications (Singer, 2001). Strep throat is a bacterial infection, which is the cause in about 25% of children and 10% of adults (Hildreth et al., 2015). An estimated 616 million cases of GABHS pharyngitis occur annually worldwide (Carapetis et al., 2005).
Rapid diagnosis and treatment of pharyngitis and tonsillitis patients with unnecessary antibiotic prescriptions in primary health care center lead to high costs and increased risk of antibiotic-resistance. Pharyngitis and its epidemiological factors are a public health problem. Since there is no such study in this area, this research was done in Souk Al-kamees, Libya. The aim of this study was: (i) to identify the frequency of childrens’ pharyngitis in Souk Al-kamees, Libya, (ii) to study the epidemiological factors of pharyngitis according to gender, age, seasonal variation, history of tonsillectomy and associated disease among the survey population, and (iii) to identify the bacterial pharyngitis especially GABH among the study population.
Study design
A study designed to be prospective of suspected cases of pharyngitis. The preliminary data collected by questionnaire from Souk Al-Kamees outpatient clinic, Alkhoms, Libya. The study was conducted for 12 month (February 2018 - January 2019). The study population age ranged between 1 and 14 years of those attending Souk Al-Kamees outpatient clinic with a suspected case of pharyngitis with throat-related complaints (sore throat).
Moreover, patient demographics clinical data include age, sex, race, blood sample, and patient symptoms were recorded. The samples were collected by the throat swab from just above the tonsils of an infected throat of the patients. The sample was immediately placed in a nutrient broth and incubated at 37°C for 24 h. The samples were transported to the laboratory for culture and identification.
Methods
The collected swabs from the patients were cultured on the Blood agar and incubated at 37°C in an anaerobic incubator for 24 to 48 h. The colonies were tested with Gram stain for morphology and identification (Biomaghret, Tunisia). Biochemical tests like catalase test were done with the slide test for the identification of Group A beta hemolytic Streptococcus. A bacitracin disc was added to a plate of blood agar to find the GABH sensitive to bacitracin (huge inhibition occurred around bacitracin disk). Streptococcus pyogenes are sensitive to bacitracin (Pires et al., 2009). The ASO serological methods like latex agglutination for the qualitative and semi-quantitative measurement of antibody to anti streptolysin-O in human serum were done (Biomaghret, Tunisia). The collected data were analysed by SPSS software version 1.3 and significance level of P< 0.01.
This study was done for a period of 12 months from February 2018 to January 2019 on 394 children. But 237 were found with acute pharyngitis in targeted-age (1-14 years). Samples were taken in Souk Al-Kamees Primary Clinic, throat swab were collected from patients for blood culture and biochemical tests and the blood samples were taken for Anti Streptolysin-O titre.
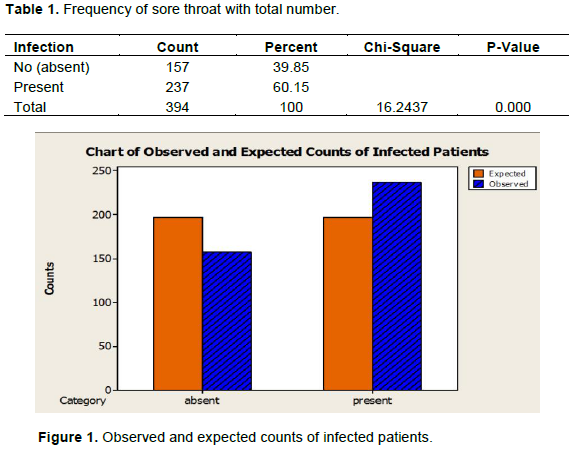
Frequency of sore throat cases from the total number of patients
Total number of patients who visited the clinic with age bracket of 1 to 14 years were 394. Table 1 shows the percent of sore throats from the total number of visited patients was 60.15%. Significant relationship between sore throat cases and the number of patients visiting primary health care units by P<0.01. Observed and expected counts of infected patients are as shown in Figure 1. The result indicates that sore throat is one of the most common reasons for visits to the clinic.
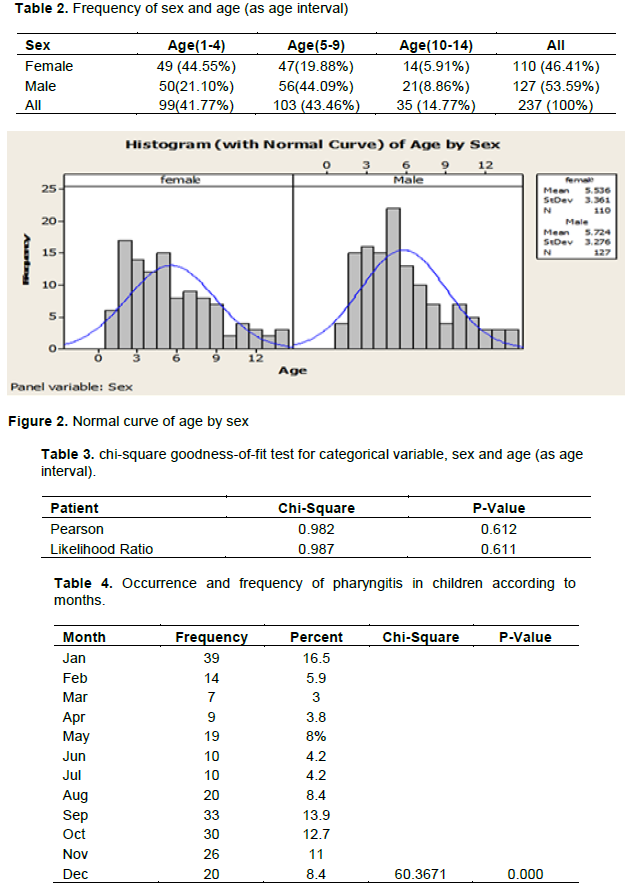
Frequency of sex and age (as age interval)
Table 2 shows age range 5-9 years, is the most affected by sore throat with 43.46% and age range 10-14 years is less affected by 14.77%. In females, the most affected by pharyngitis is age range 1-4 years by 44.55% and in male the most affected by pharyngitis is age range 5-9 years with 44.09%. The results also show that the cases of sore throat in males by 53.59% were higher than females by 46.41%. Figure 2 shows the shape of the distribution of the age by sex of the normal curve. No significant relation was found between age and sex and occurrence of pharyngitis in children by P˃0.01 (Table 3).
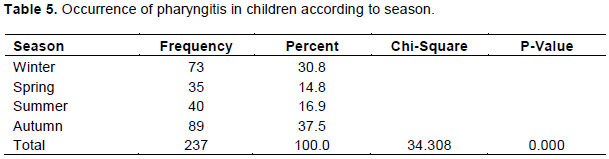
Occurrence pharyngitis in children according to months
Table 4 shows that during the different months of this study; January and September have the highest rate of acute pharyngitis in children by 16.5% and 13.9% respectively. While the lowest rate of acute pharyngitis in children in March and April by 3 and 3.8%, respectively, showing significant relation between occurrence pharyngitis in children and months by P- < 0.01.
Occurrence of pharyngitis in children according to season
Table 5 shows that acute pharyngitis in children peaked twice during autumn by 37.5% (November, October and September) and winter by 30.8% (December, January and February), showing a significant relation between occurrence pharyngitis in children and season by P- < 0.01.
Occurrence of pharyngitis in children according to symptoms
Table 6 shows that fever, cough, and running nose were the highest symptoms among children with acute pharyngitis (64% of fever, 47.7% of cough and 43% of running nose).
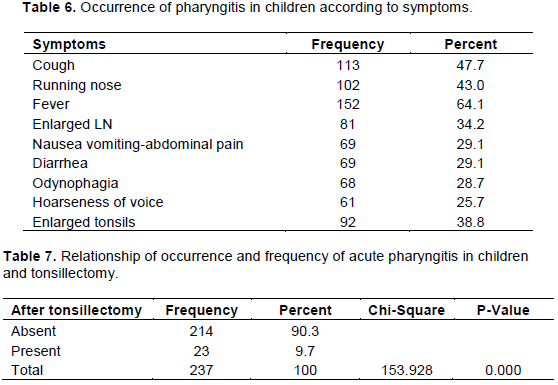
Relationship of occurrence of acute pharyngitis in children and tonsillectomy
Table 7 shows that only 23 patients from total of 237 patients had tonsillectomy. Most cases had viral sore throat; this means the tonsillectomy operation reduced GAS pharyngitis episodes in children. Showing significant relationship between occurrence of pharyngitis in children and operation of tonsillectomy by P < 0.01.
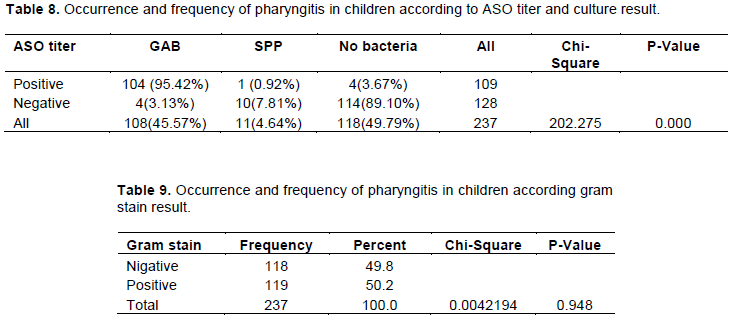
Occurrence of pharyngitis in children according to ASO titer and culture result
Table 8 shows that the ASO titer positive result associated with pharyngitis (GAS) by 95.42% more than anther causes of pharyngitis (SPP) by 0.92%. It also shows positive result with no bacteria by 3.67% in some carrier cases. Showing significant relation (P- < 0.01) between positive result of ASO titer in this study and pharyngitis by GAB.
Occurrence pharyngitis in children according to gram stain
Table 9 shows Gram positive bacteria as a cause of acute pharyngitis in children such as GAS that is most common then SPP. Showing No significant relationship between bacterial pharyngitis frequency in children and nonbacterial pharyngitis according to Gram stain results by P > 0.01.
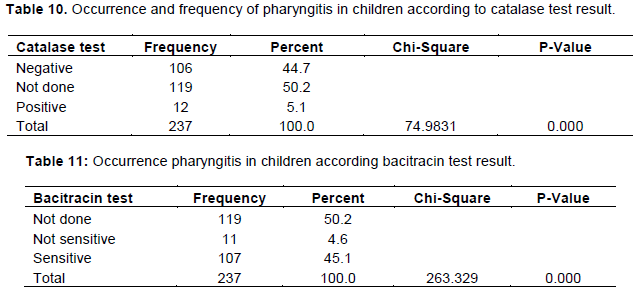
Occurrence pharyngitis in children according to catalase test
Table 10. shows catalase tests, more negative than positive results, which means that bacterial pharyngitis affects children with GAS type more than SPP. Non-bacterial samples were not tested. Showing significant relation (P- < 0.01) between bacterial pharyngitis and catalase test results. This result of catalase test can be used to differentiate between two types of Gram-positive bacteria in this study.
Occurrence pharyngitis in children according to bacitracin test
Table 11 shows the bacitracin test result indicating that the sensitive results are more than non-sensitive tests. This result shows bacterial pharyngitis in children by GAS is more sensitive than SPP in this study. Non-bacterial samples were not tested. Showing significant relation (P- < 0.01) between bacterial pharyngitis and bacitracin test results. So bacitracin test can be used to differentiate between two types of Gram-positive bacteria in this study.
Sore throat is still the most common reason for visits to physicians. In the present study the percent of sore throat from total number of visitor equals 60.15%. Similar result was found by Bisno et al. (2002) in America and also in another study by Linder and Stafford (2001).
In this study, the culture result shows the occurrence of bacterial pharyngitis in children was more than nonbacterial pharyngitis by 50.2%. Results have shown that the pharyngitis by GAS is the most common as a bacterial cause of pharyngitis in children by 45.6%. Previous studies have shown exudative pharyngitis in children with acute Streptococcal infection 86% in Spain (Baquero et al., 1999) and 54% in Latvia (Zavadska, 2010). Another study showed that the GAS disease prevalence ranged from 21.4 to 27% among children aged 1-15 years in northern Taiwan (Lin et al., 2003). In contrast, a study carried out by Chi et al. (2003) showed that virus caused most acute pharyngitis and that GAS pharyngitis was uncommon in Taipei and Jos, Nigeria. Previous reports have also shown that Streptococcal throat carriage rate was 9.78% amongst primary school pupils in Benin, Nigeria (Sadoh, 2001).
The highest occurrence rate was in the 5-9 years age group. This might be due to high exposure to the outer environment and lack of awareness. Several previous studies show similar results as pharyngitis is the highest at age 5-15 year by 37% in England (Bisno, 1996; Pichichero, 1997; Pickering et al., 2000). Evidence suggests that the prevalence of infection in this age-group may be due to the increased activity of children, giving a higher chance for the exposure to infection (Saleh, 2009). Besides, this school-age children may be making contact with each other in classrooms leading to increased infections. In the current study, an occurrence of pharyngitis in children among boys was 53.6%, compared to 46.4% in girls. A study in Sabha, Libya done by Soliman (2012) showed the pharyngitis infection rates for males was 64.3% and that of females was 35.7%. In contrast, a study in Syria found that distribution of pharyngitis in male was 47.4% and female was 53.6% (Cherith et al., 2005).
A monthly comparison showed that January (16.5%) and September (13.9%) contain the highest rate of occurrence of acute pharyngitis in children. While the lowest rate of occurrence of acute pharyngitis in children occurred in March (3%) and April (3.8%). In addition, the acute pharyngitis in children peaked twice during year in autumn 37.6% (November, October and September) and winter by 30.8% (December, January and February). This results may be due to children staying mostly indoors in crowded conditions, which may increase the rate of transmission of infection. In a similar study in Benghazi by Alhouni (2005), the peak incidence of infection was reported in winter and autumn. In contrast, previous studies in Taiz/Yemen by Saleh (2009), found the highest prevalence during winter season (November and December) as well as rainy season (July and August). In north India, a study by Nandi et al. (2001) showed that the relative incidence was higher during the winter (November to January) and rainy (August) months.
In the current study, results have shown that fever, cough, and running nose were the highest symptom among children with acute pharyngitis (64% of fever, 47.7% of cough and 43% of running nose). A study in Benin city showed fever and inflamed tonsils/pharynx were the most frequent signs or symptoms occurring in 89.04 and 87.67%, respectively (Wilson, 2008). Another study in Latvia showed pharyngeal erythema and fever were prevalent up to 90 and 85%, respectively (Zavadska, 2010).
The results of the study showed that only 23 patients out of the total number of patients have tonsillectomy, usually a viral sore throat, which means that the operation of tonsillectomy reduces the occurrence of pharyngitis in children. Similar to a study in Finland by Alho et al, (2007) reported that the tonsillectomy reduces the number of acute pharyngitis and symptoms.
Antistreptolysin-O (ASO) test is an accurate diagnosis of pharyngitis and, is necessary to rule out group A streptococcus (Vintilescu et al., 2020). In this study, the positive result of ASO titer is 46%; this percent represents previous infection by GAS and negative result by 54%. In similar study by Stollerman and Dale (2008), the ASO titer significantly elevated over normal levels during a Streptococcal infection. Therefore, the ASO titer is the standard serological assay for confirmation of Group A Streptococcal infection.
The study indicated both female and male have occurrence of pharyngitis in this age range (1-14 years), but no significant difference between the gender. The age range 5-9 years is the most affected with sore throat in patients. The January and September months contained the highest rate of occurrence of acute pharyngitis in children while the lowest rate of occurrence of acute pharyngitis in children was in March. Occurrence of acute pharyngitis in children peaked twice during the year in autumn and winter.
The clinical features like fever, cough, running nose were the highest symptoms among children with acute pharyngitis. Appearance of bacterial pharyngitis in children is more than non-bacterial pharyngitis and the most common is bacterial pharyngitis (GAS) in children. The positive results of ASO titer associated with pharyngitis by GAB are more than other causes of pharyngitis. However, this study shows two-Gram positive bacteria as a cause of bacterial pharyngitis in children, such as GAS, that is, the most common and Staphylococcus species.
The authors have not declared any conflict of interests.
REFERENCES
|
Alho O, Koivunen P, Penna T, Teppo H, Koskela M, Luotonen J ( 2007). Tonsillectomy versus watchful waiting in recurrent streptococcal pharyngitis in adults: randomised controlled trial. British Medical Journal 334(7600):939.
Crossref
|
|
|
|
Alhouni M (2005). Upper respiratory tract infection associated with streptococcus pigeon in Benghazi area M.S.C. Thesis. Faculty of science, Benghazi university-Libya.
|
|
|
|
|
Baquero F, Garcia-Rodriguez JA, de Lomas JG, Aguilar L (1999). Antimicrobial resistance of 914 beta-hemolytic streptococci isolated from pharyngeal swabs in Spain: results of a 1-year (1996-1997) multicenter surveillance study. The Spanish Surveillance Group for Respiratory Pathogens. Antimicrobial Agents and Chemotherapy 43:178-180.
Crossref
|
|
|
|
|
Bhalla K, Bhardwaj P, Gupta A, Mehra S, Nehra D Nanda S, (2019). Role of epidemiological risk factors in improving the clinical diagnosis of streptococcal sore throat in pediatric clinical practice. Journal of family medicine and primary care 8(10):3130.
Crossref
|
|
|
|
|
Bisno AL (1996). Group A streptococcal infection. Pediatrics 6:949-954.
|
|
|
|
|
Bisno AL, Michael AG, Jack M, Gwaltney Jr, Edward LK, Richard HS (2002). Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Clinical Infectious Disease 35(2):113-125.
Crossref
|
|
|
|
|
Carapetis JR, Steer AC, Mulholland EK, Weber M (2005). The global burden of group A streptococcal diseases. Lancet Infectious Diseases 5(11):685-694.
Crossref
|
|
|
|
|
Cherith A, Marweshia F, Moussa R (2005). Epidemiology of pharyngitis and tonsilitis in childern and clinical laboratory connection of proving bacterial diagnosis .Tishreen university journal for studies and scientific research 27(3):183-192.
|
|
|
|
|
Chi H, Chiu NC, Li WC, Huang FY (2003). Etiology of acute pharyngitis in children: Is antibiotic therapy needed? Journal of Microbiology, Immunology and Infection 36(1):26-30.
|
|
|
|
|
Hildreth A, Takhar S, Clark M, Hatten B (2015). Evidence-Based Evaluation And Management Of Patients With Pharyngitis In The Emergency Department. Emergency medicine practice 17(9):1-16; quiz 16-17.
|
|
|
|
|
Kirkpatrick GL (1996). The common cold. Primary Care 23(4):657-675.
Crossref
|
|
|
|
|
Leung AK, Kellner JD (2004). Group A β-hemolytic streptococcal pharyngitis in children. Advances in therapy 21(5):277-287.
Crossref
|
|
|
|
|
Lin MH, Chang PF, Fong WK, Yen CW, Hung KL, Lin SJ (2003). Epidemiological and clinical features of group A Streptococcus pharyngitis in children. Acta Paediatr Taiwan 44(5):274-278.
|
|
|
|
|
Linder JA, Stafford RS (2001) Antibiotic treatment of adults with sore throat bycommunity primary care physicians: a national survey 1989-1999. Journal of the American Medical Association 286:1181-1186.
Crossref
|
|
|
|
|
Nandi S, Kumar R, Ray P, Vohra H, Ganguly NK (2001). Group A streptococcal sore throat in a periurban population of northern India: a one-year prospective study. Bulletin of the World Health Organization 79:528-533.
|
|
|
|
|
Pichichero ME (1997). Sore throat after sore throat after sore throat. Are you asking the critical questions? Postgraduate Medical Journal 101(1):205-212.
Crossref
|
|
|
|
|
Pickering LK, Peter G, Baker CJ (2000). Group A streptococcal infections. In: Pickering LK, editor. Red Book: Report of the committee on Infectious Diseases. 25th ed. Elk Grove, Il: Academy of Pediatrics pp. 526-532.
|
|
|
|
|
Pires R, Rolo D, Mato R, Feio de Almeida, Johansson C, Henriques-Normark B, Morais A, Brito-Avô A, Gonçalo-Marques J, Santos-Sanches I (2009). Resistance to bacitracin in Streptococcus pyogenes from oropharyngeal colonization and noninvasive infections in Portugal was caused by two clones of distinct virulence genotypes. Federation of European Microbiological Societies 296(2):235-240.
Crossref
|
|
|
|
|
Principi N, Bianchini S, Baggi E, Esposito S (2013). No evidence for the effectiveness of systemic corticosteroids in acute pharyngitis, community-acquired pneumonia and acute otitis media. European journal of clinical microbiology & infectious diseases 32(2):151-160.
Crossref
|
|
|
|
|
Rutter P, Newb D (2015). Community Pharmacy ANZ-eBook: Symptoms, Diagnosis and Treatment: Elsevier Health Sciences 400 p.
|
|
|
|
|
Sadoh WE (2001). Streptococcal throat carriage rate amongst primary school pupils in Egor Local Government Area of Edo State of Nigeria. A dissertation submitted to the West African College of Physicians, in part fulfillment of the fellowship of the college.
|
|
|
|
|
Saleh MM (2009). Streptococcal throat infection among Yemeni children. Iraqi Journal of Science 50(1):126-135.
|
|
|
|
|
Singer K (2001). The 15-minute visit (acute pharyngitis). Patient Care 35:20-23.
Crossref
|
|
|
|
|
Soliman M (2012). Prevalence of Streptococcus Pyogenes in Children with Pharyngitis in Sabha City. Master science, thesis. The Libyan Academy-Benghazi-Libya.
|
|
|
|
|
Stollerman GH, Dale JB (2008). The importance of the group A Streptococcus capsule in the pathogenesis of human infections: a historical perspective. Clinical Infectious Diseases 46(7):1038-1045.
Crossref
|
|
|
|
|
Van Schoor J (2013). Colds, flu and coughing: over-the-counter products for pharyngitis and tonsillitis. South African Family Practice 55(4):330-333.
Crossref
|
|
|
|
|
Vintilescu BȘ, Ionita E, Niclescu EC, Stepan MD, Becheanu CA (2020). Analysis of Biochemical Parameters in Children with Chronic Tonsillitis. Current Health Sciences Journal 46(2).
|
|
|
|
|
Wilson ES (2008). Bacterial isolates of Tonsillitis and Pharyngitis in a Paediatric casualty setting. Journal of Medical and Biological Research: A Peer-review Journal of Biomedical Sciences 7:1-2.
Crossref
|
|
|
|
|
Zavadska D (2010). Group A beta haemolytic streptococcus infection in children in latvia PhD thesis. Internal medical science. Riga stradin university. dzirciema str.
View
|
|