ABSTRACT
Food borne diseases (FBDs) can occur due to the health status of the food handlers. The present study aimed to assess food hygiene knowledge, attitude and practices among hospital food handlers of ElManagil City, Sudan. A cross-sectional study was administered to evaluate knowledge, attitudes, and practices, in food hygiene among hospital food handlers through a questionnaire. The food handlers expressed a level of knowledge, attitude, and practice of 70.1, 63.81 and 74.40%, respectively. The food handlers lacked knowledge regarding the transmission of hepatitis A virus and the working of infected food handler. They demonstrated poor attitude regarding the continuous evaluation of their health status, as well as the importance of training courses in the prevention of food contamination. They exhibited a low practice rate regarding removing nail polish and covering the head while preparing food. Statistically significant differences were found when comparing the educational level with washing the utensils with a detergent, along with wearing gloves while working. It was concluded that the hospitals food handlers in ElManagil expressed moderate level of knowledge, positive attitude, and good practice in food hygiene. Generally, there is an urgent need to improve on food hygiene in health care systems in Sudan. Food hygiene training programs should be implemented among health care food handlers.
Key words: Attitude, Elmanagil City, food handlers, food hygiene, hospitals, knowledge, practice.
Food-borne diseases (FBDs) have been reported by the World Health Organization to be one of the main causes of morbidity and mortality in developing countries (WHO, 2015).Factors such as unhygienic practices, insufficient sanitation, inadequate cooking, improper storage, cross-contamination and purchasing food from unsafe sources can lead to food poisoning. Improper food handling practices are the most common factor associated with FBD outbreaks (Nyachuba, 2010; Koopmans and Duizer, 2004; Al Suwaidi et al., 2015). In African countries, FBDs have a negative health impact in hospitals. In Sudan, there is a considerable public health burden due to FBDs. Many different pathogens and toxins are known to cause FBDs, with newer ones occasionally emerging, especially among restaurant workers. Pathogenic organisms are carried widely among food handlers in Sudan. In one study, 30.1% of food handlers were found to be carriers of pathogenic organisms, such as Staphylococci, Salmonella, and Shigella in addition to other pathogens (Saeed and Hamid, 2010), hence the food handlers may play a key role in the spread and transmission of food communicable diseases. FBDs occur for many reasons, but most cases are related to the health status of the food handler and his/her personal hygiene, knowledge, attitude and practices (Mudey et al., 2010). A food handler is anyone who handles food, whether preparing or serving it (Isara and Isah, 2009). Personal hygiene, such as hand washing, wearing gloves and masks, covering the head and sanitizing/cleaning surfaces, could be a preventive procedure to reduce FBDs in hospitals. Food handlers could also play a significant role by implementing food hygiene measures to ensure food safety (Mudey et al., 2010). In hospitals, medical staffs as well as patients and their relatives consume food from the hospital kitchen, so there should be some level of awareness regarding the health status of food handlers in hospitals (Aycicek et al., 2004). Generally, Food handlers in the hospitals of Sudan, do not have sufficient food-hygiene-related awareness or knowledge regarding the implementation of food safety measures (Honua, 2018). Implementing food safety measures can reduce the risk of FBD occurrences among hospital staffs, patients and even people who eat at hospitals. Therefore, the aim of this study is to assess food hygiene knowledge, attitude and practices among food handlers in ElManagil city, Sudan.
A cross-sectional study was performed from July 2016 to July 2018 in ElManagil City, Sudan, to evaluate the knowledge, attitude and practices related to food hygiene among hospital food handlers. ElManagil is a city in Al Jazirah State, Sudan, where the agricultural sector is the main practice of the population. The target population included food handlers in hospital kitchens and cafeterias at ElManagil Teaching Hospital. The distribution of the socio-demographic data for the hospital food handlers at ElManagil included gender, age, marital status, educational level and work experience. A questionnaire was used to gather data on the demographic variables and food-hygiene-related knowledge (22 items), attitude (16 items) and practices (10 items) of the participants. Consent was obtained from all subjects under study, and approval was taken from the National Ethics Committee of the Ministry of Health of Sudan. IBM SPSS Statistics was used for Windows (version 21; IBM Corp., Armonk, NY, USA) for data entry and analysis. Categorical data are presented as numbers and percentages. Chi-squared test also was used to study the associations between the variables of higher levels in knowledge, attitude and practices and the educational level of the food handlers. P-value of < 0.05 was considered as statistically significant.
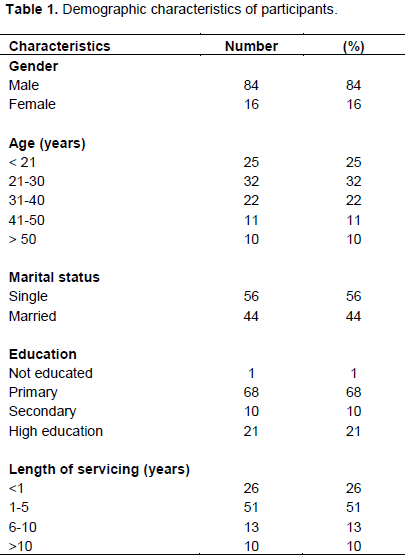
Table 1 shows the distribution of the socio-demographic data for 100 food handlers at ElManagil Teaching
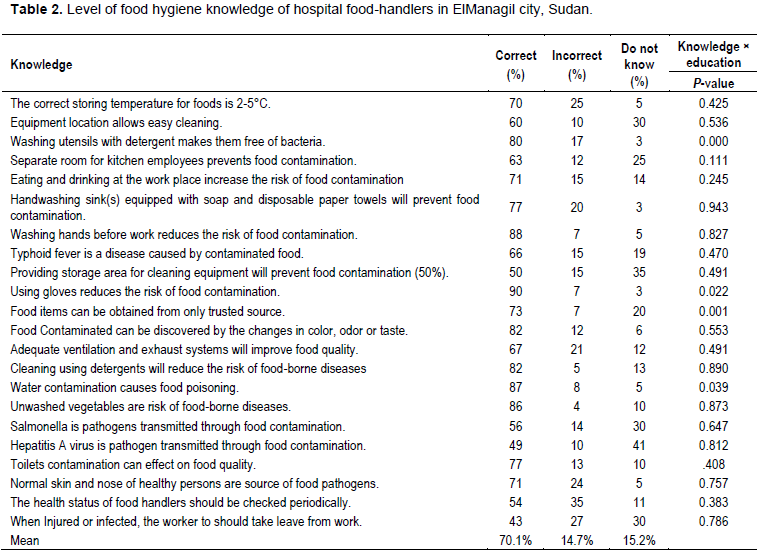
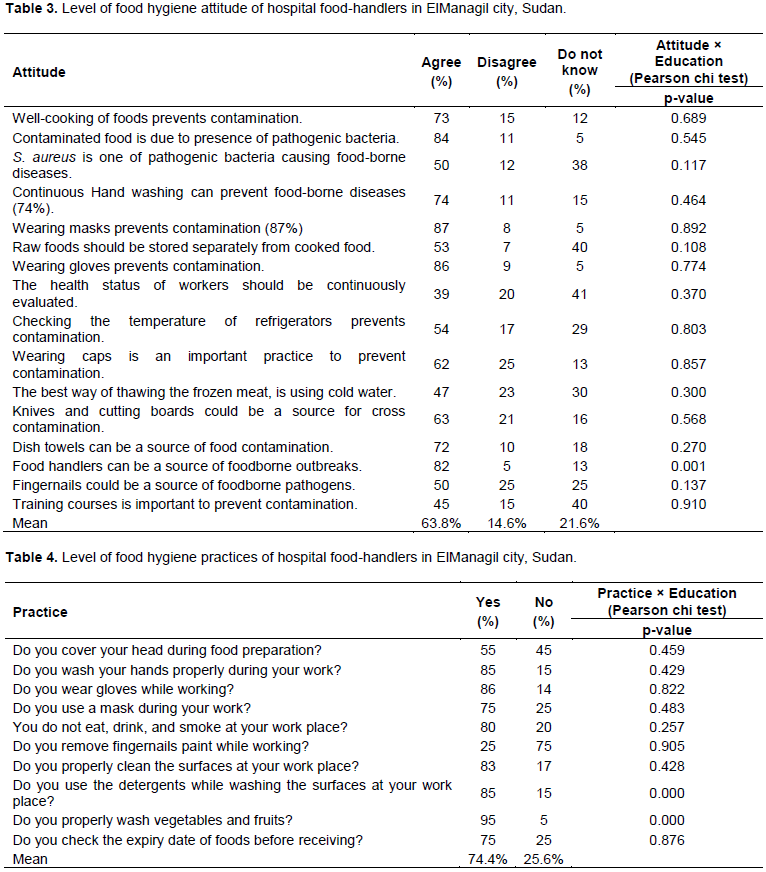
Hospital as follows; among the study population, 84 (84%) were males and 16 (16%) were females. Our results show that, most of the participants (32 participants, 32%) were in the 21–30 years’ age group, followed by the <21 years’ age group (25 participants, 25%) and 31-40 years’ age group (22 participants, 22%). Also, among the study population, 56 (56%) were married and 44 (44%) were unmarried. Primary education constituted the most frequent educational category investigated (68 participants, 68%), followed by higher education (21 participants, 21%).The most frequent category of servicing years for the food handlers was 1–5 years (51 participants, 51%), followed by less than one year (26 participants, 26%), whereas the least frequent category was more than 10 years (10 participants, 10%), followed by 6-10 years (13 participants, 13%) (Table 1). The food handlers in the study population expressed a moderate level of knowledge, with a mean of 70.1%. Among the study population, according to Table 2, the level of knowledge of the food handlers was high regarding the notion that wearing gloves reduces the risk of food contamination (90.0%), followed by the notions that washing hands before work reduces the risk of food contamination (88%) and that water contamination causes food contamination (87%). Also the knowledge of the food handlers was poor in terms of four food contamination scenarios: (i) when a worker gets injured or infected, he/she should take a leave from work (43%); (ii) hepatitis A virus is a pathogen transmitted through food contamination (49%); (iii) providing a storage area for cleaning equipment prevents food contamination (50%); and (iv) the health status of food handlers should be checked periodically (54%).Differences between the educational levels and knowledge variables (e.g., washing the utensils with a detergent makes them free of bacteria; wearing gloves reduces the risk of food contamination; food should be obtained only from a trusted source) were found to be statistically significant ( ) (Table 2). All food handlers in our study expressed positive attitude with a mean of 63.8%. Among the study population, as shown in Table 3, the level of attitude among food handlers toward food contamination was high regarding the notion that wearing a mask prevents contamination (87%), followed by the notions that wearing gloves prevents contamination (86%), that food contamination is caused by pathogenic bacteria (84%) and that food handlers could be a source of food-borne outbreaks (82%). Our results show that, the attitude of the food handlers was poor regarding the following food contamination scenarios: the health status of all workers should be continuously evaluated (39%); training courses are important to prevent contamination (45%); the best way to thaw frozen meat is to use cold water (47%); fingernails are a potential source of food-borne pathogens (50%); and Staphylococcus aureus remain one of the pathogenic bacteria that cause food-borne diseases (50%). The difference between the educational level and the notion that food handlers could be a source of food-borne outbreaks was statistically significant ( ) (Table 3). All food handlers at hospitals in ElManagil expressed good practice in food hygiene, with a mean of 74.4%. Table 4 presents the responses of the food handlers to the practice questions on food contamination. The highest-ranked practice among the respondents was the practice of properly washing vegetables and fruits (95%), followed by the practices of wearing gloves while working (86%); using detergents while washing any surface at the workplace (85%); washing hands properly during work (85%); properly cleaning the surfaces at the workplace (83%) and eating, drinking and smoking at the workplace (80%). In addition, the lowest-ranked food contamination practice among the food handlers was the practice of removing nail polish while working (25%), followed by the practice of covering the head while preparing food (54%).Differences between the educational level and practice variables(e.g. using detergents while working, washing the surfaces and washing vegetables and fruits)were statistically significant ( ), as shown in Table 4.
Food handlers are regarded as the main source of food contamination, either through manual contact or through respiratory secretions. In particular, food handlers in hospitals may contaminate food and, hence, cause outbreaks of food-borne infections in hospitals(Maguire et al., 2000). The results indicated that the majority of the study subjects were men, which is in contrast to those of many studies that reported a higher proportion of females (Isara and Isah, 2009; Baluka et al., 2015). Regarding age distribution, results from similar studies carried out in India indicated that most food handlers ages were from the15–30 years’ age group (Prabhu and Shah, 2014).In total,67.5% of the subjects had an educational level of primary school; thus, the performance of employees regarding food safety might not be satisfactory and, thus, may cause public health problems(Webb and Morancie, 2015). A larger number of participants (51%) had one to five years of experience working in foodservices, followed by participants with less than one year of experience(26 participants, 26%), which is similar to findings from Turkey (Bas et al., 2006). Having good knowledge of food-handling practices and hospital-related infections will definitely improve the experience of workers at hospital kitchens. The food handlers in the study population showed a moderate level of food hygiene knowledge. Similar to our results, it has been found in one study that food handlers had good knowledge regarding personal hygiene and the relationship of food-borne diseases (Hassan and Dimassi, 2014). In general, food handlers had sufficient knowledge regarding the purpose of wearing loves and washing hands and the effect of water contamination, but they lacked knowledge regarding the transmission of hepatitis A virus and whether injured or infected food handlers should work. Similar studies showed that food handlers have poor knowledge regarding many food-hygiene-related issues (Allam et al., 2016; Akabanda et al., 2017).It is important that food handlers at hospitals be knowledgeable about food safety, food hygiene and infection control to make sure that the food is prepared and handled safely to the patients (Mudey et al., 2010; Lestantyo et al., 2017). In our study, food handlers expressed positive attitude towards food hygiene. Similar studies showed that all participants agree that food handlers should be regularly medically examined (Iwu et al., 2017; Bamidele et al., 2015). It is very important that food safety training programs be implemented for food handlers working in the healthcare sector in Sudan, because education and training in hygienic practices may reduce the morbidity and mortality associated with FBDs in hospitals (Ansari and Khan, 2012). Statistically significant associations were found between the educational level and the attitude regarding the notion that food handlers are a potential source of food-borne outbreaks. In Dessie town, Ethiopia, Adane et al. (2018) reported a significant association between the availability of service training and medical check-up with the levels of food hygiene and safety practices. The attitude regarding thawing frozen meat using cold water was found to be poorly rated among the studied food handlers. Re-freezing food causes bacteria to multiply and could result in outbreaks of food-borne illnesses (Julie, 2012). The food handlers in the study population showed good food-hygiene-related practices. Similarly, it has been shown in a study (Park et al., 2010)that food handlers practiced cleaning and disinfection procedures properly. Other studies reported that some food handlers would even keep working even when they get sick (Mudey et al., 2010; Lestantyo et al., 2017). Statistically significant associations were found between the educational level and the practices of using detergents to clean surfaces while working as well as washing surfaces and washing vegetables and fruits before consumption. It can, hence, be concluded that food handlers at hospitals in ElManagil city expressed a moderate level of knowledge, positive attitude and good practices regarding food hygiene. There is an urgent need to improve the level of food safety in the healthcare system across Sudan. It is also important to implement food safety training programs for food handlers working in the healthcare sector to improve their knowledge, attitude and practices.
The authors have not declared any conflict of interests.
REFERENCES
|
Adane M, Teka B, Gismu Y, Halefom G, Ademe M (2018). Food hygiene and safety measures among food handlers in street food shops and food establishments of Dessie town, Ethiopia: A community-based cross-sectional study. PlosONE 13(5):e0196919.
Crossref
|
|
|
|
Akabanda F, Hlortsi EH, Owusu-Kwarteng J (2017).Food safety knowledge, attitudes and practices of institutional food-handlers in Ghana. BMC Public Health 17(1):40.
Crossref
|
|
|
|
|
Allam H, Al-Batanony MA, Seif AS, Awad ET (2016). Hand Contamination among Food Handlers. British Microbiology Research Journal13:1-8.
Crossref
|
|
|
|
|
Al Suwaidi A, Hussein H, Al Faisal W, El SawafE, Wasfy A (2015). Hygienic Practices among Food Handlers in Dubai. International Journal of Preventive Medicine Research1(3):101-108.
|
|
|
|
|
Ansari MA, Khan Z (2012). An Evaluation of Health Education Intervention on Hygienic Status of Food Handlers in Aligarh - A Three Year Experience. Journal of Community Medicine and Health Education 2:142.
Crossref
|
|
|
|
|
Aycicek H, Aydogan H, Kucukkaraaslan A, Baysallar M, Celal BA (2004). Assessment of the bacterial contamination on hands of hospital food handlers. Food Control 15(4):253-259.
Crossref
|
|
|
|
|
Baluka SA, Miller R, Kaneene JB (2015). Hygiene practices and food contamination in managed food service facilities in Uganda. African Journal ofFood Science9(1):31-42.
Crossref
|
|
|
|
|
Bamidele J, Adebimpe W, Oladele E, Adeoye O (2015). Hygiene practices among workers in local eateries of Orolu community in south Western Nigeria. Annals of Medical and Health Sciences Research 5(4):235-240.
Crossref
|
|
|
|
|
Bas M, SafakA,Ersun, Go¨khanKıvanc (2006). The evaluation of food hygiene knowledge, attitudes, and practices of food handlers' in food businesses in Turkey; Food control 17:317-322.
Crossref
|
|
|
|
|
Hassan HF, Dimassi H (2014).Food safety and handling knowledge and practices of Lebanese university students.Food Control 40(1):127-133.
Crossref
|
|
|
|
|
HonuaMHM (2018). The bacterial contamination of food handlers hands in Wad madani city restaurants, Sudan. International Journal Of Community Medicine and Public Health 5(4):1270-1273.
Crossref
|
|
|
|
|
Isara AR, Isah EC (2009). Knowledge and practice of food hygine and safety among food handlers in fast food restaurants in Benin City, Edo state, Niger. Postgraduate Medical Journal 16(3):207-212.
|
|
|
|
|
Iwu AC, Uwakwe KA, Duru CB, Diwe KC, Chineke HN, Merenu IA, Oluohaet UR,MadubuezeUC,Ndukwu E, Ohale I (2017). Knowledge, Attitude and Practices of Food Hygiene among Food Vendors in Owerri, Imo State, Nigeria. Occupational Diseases and Environmental Medicine 5(01):11-25.
Crossref
|
|
|
|
|
Julie GR (2012). Food Safety Basics. A Reference Guide for Food Services Operators 1:5-6.
|
|
|
|
|
Koopmans M, Duizer E (2004). Foodborne viruses: an emerging problem. InternationalJournal of Food Microbiology 90:23-41.
Crossref
|
|
|
|
|
Lestantyo D, Husodo AH, Iravati S, Shaluhiyah Z (2017).Safe Food Handling Knowledge, Attitude and Practice of Food Handlers in Hospital Kitchen. International Journal of Public Health Science 6(4):324-330.
Crossref
|
|
|
|
|
Maguire H, Pharoah P, Walsh B, Davison C, BarrieeD,Threlfall EJ, Chambers S (2000). Hospital outbreak of Salmonella virchow possibly associated with a food handler.Journal of Hospital Infection 44(4):261-266.
Crossref
|
|
|
|
|
Mudey AB, Kesharwani N, Mudey GA, Goyal RC, Ajay K, Dawale AK, Vasant V, Wagh VV (2010). Health status and personal hygiene among food handlers working at food establishment around a rural teaching hospital in Wardha District of Maharashtra, India. Global Journal of Health Science2(2):198-206.
Crossref
|
|
|
|
|
Nyachuba DG (2010). Foodborne illness: Is it on the rise? Nutrition Reviews 68(5):257-269.
Crossref
|
|
|
|
|
Park SH, Kwak TK, Chang HJ (2010). Evaluation of the food safety training for food handlers in restaurant operations. Nutrition Research and Practice4(1):58-68.
Crossref
|
|
|
|
|
Prabhu PM,Shah RS (2014). Study of Food Handlers in Public Food Establishments in Maharashtra, India.International Journal of Science and Research 3(7):1485-1489.
|
|
|
|
|
Saeed HA, Hamid HH (2010).Bacteriological and parasitological assessment of food handlers in the Omdurman area of Sudan.Journal of Microbiology, Immunology and Infection43(1):70-73.
Crossref
|
|
|
|
|
Webb M, Morancie A (2015). Food safety knowledge of foodservice workers at a university campus by education level, experience, and food safety training. Food Control50:259-264.
Crossref
|
|
|
|
|
WHO (2015).Report on global burden of foodborne disease. 2015.
|
|



