Full Length Research Paper

ABSTRACT
The SCCmec element is one of the recommended targets for MRSA characterization and several multiplex-PCR SCCmec typing methods have been developed over the past years. However, there are no data on the consistency of the SCCmec types in clinical isolates as detected by these methods. Using different previously published, commonly used M-PCR methods, this report describes the diversity of SCCmec elements in MRSA isolates in the Pretoria region of South Africa and the discrepancies observed in the assigned SCCmec types. Different SCCmec types were assigned to the same clinical MRSA isolates. The discrepancies included the assignment of composite SCCmec types [(SCCmec II and SCCmecury) 20.7% (40/193)] and [(SCCmec type II+IVc) 22.3% (43/193)] to some of the clinical MRSA isolates. Summarily, the combination of the result of the M-PCR methods showed that the MRSA genotypes circulating in the healthcare facility studied potentially carried SCCmec types I, II, IV (subtypes IVa, IVb and IVd) and V. No SCCmec types III or VIII was detected among the isolates. At least 25.91% of SCCmec type IV was detected in this study, thus corroborating previous findings of the global encroachment of MRSA strains into the hospital settings. The associated epidemiological significance of these observations is discussed and we also call for an African consensus SCCmec typing method in order to allow effective epidemiological data comparison across the countries.
Key words: MRSA genotype, SCCmec elements, multiplex-polymerase chain reaction (PCR), variation.
INTRODUCTION
MATERIALS AND METHODS
RESULTS AND DISCUSSION
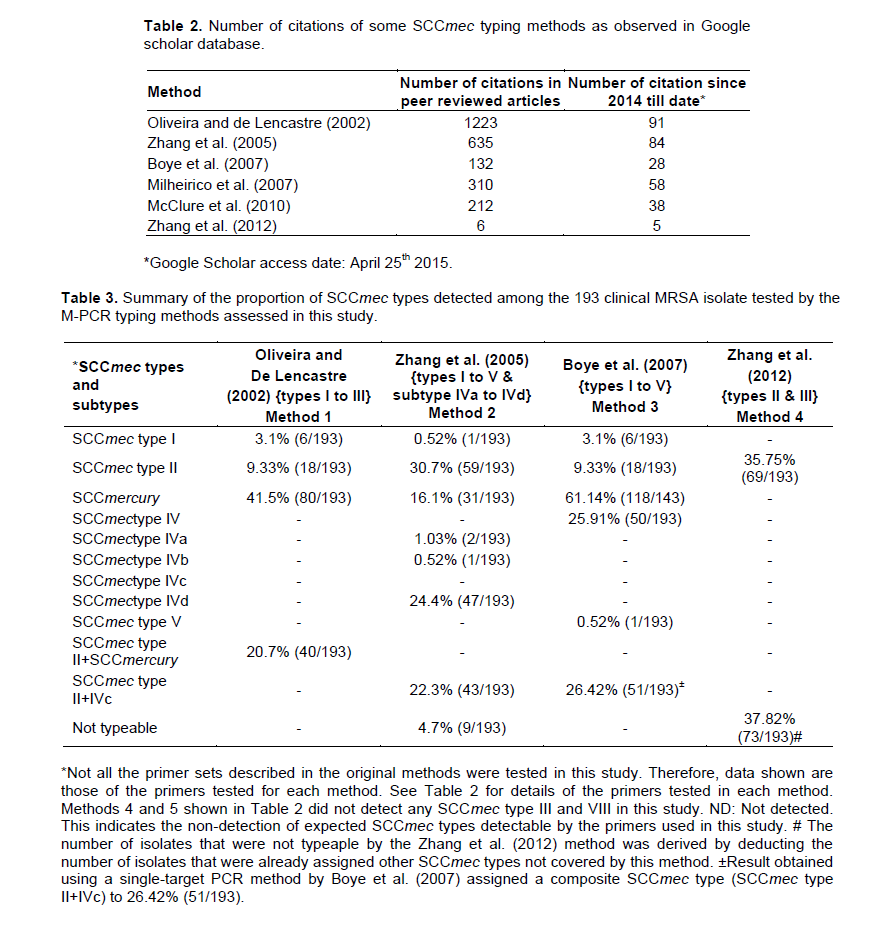
All the 193 previously determined MRSA samples were reconfirmed using the S. aureus specific primers (McClure et al., 2006). The 16S rRNA and the mecA gene were detected in all the samples tested. However, variations were observed in the proportion of samples designated as a specific SCCmec type or untypable by each SCCmec typing method assessed (Table 3). The electrophoretic pattern of the M-PCR amplicons used for the assignment of the SCCmec types is shown in supplementary material (Figure S1-S7). Table 3 shows that methods1 and 3 were able to designate equal number and same set of MRSA isolates as SCCmec I (3.1%) and SCCmec II (9.33%). The number of isolates assigned as SCCmercury by methods 1, 2 and 3 were different, with method 3 designating 61.14% (118/193) of the isolates as SCCmercury followed by method 1 {(41.5% (80/193)} and method 2 {16.1% (31/193)}.
The number of MRSA isolates designated as SCCmec I, II and SCCmercury by method 2 did not correspond to any of the other methods tested. Method 4, an updated version of method 2 designated 10 additional MRSA isolates as SCCmec II, giving a total of 35.75% (69/193) SCCmec type II MRSA isolates as compared to method 2 which assigned SCCmec type II to 30.7% (59/193) to the isolates. Method 2 was able to subtype the same set of isolates [SCCmec type IVa, 1.03% (2/193); SCCmec type IVb, 0.52% (1/193); SCCmec type IVd, 24.4% (47/193)] designated as SCCmec type IV [25.91% (50/193)] by Method 3. Moreover, one isolate was designated as SCCmec type V by Method 3.
The rest of the MRSA isolates were designated as composite SCCmec types. These included SCCmec type II+SCCmercury, 20.7% (40/193) assigned by method 1; SCCmec type II+IVc, 22.3% (43/193) and 26.42% (51/193) assigned by method 2 and 3 respectively. As SCCmercury was detected by methods 1, 2 and 3 and also in composite SCCmec type detected by method 1, it is possible that the SCCmercury is carried in separate plasmid within the bacterial cell. No SCCmec type III or type VIII was detected by the methods 4 and 5, respectively. The proportion of untypable MRSA isolates was 4.7% [(9/193); (Method 2)] and 37.82% {(73/193); (Method 4)}.
Table 4 shows the number of clinical MRSA isolates that were designated the same SCCmec type by different M-PCR methods. Methods 2 and 4 assigned SCCmec type II to 30.57% (59/193) of the same set of MRSA isolates. This was the highest number of isolates designated the same SCCmec type by the different methods investigated. Moreover, about 26% (50/193) of the same isolates were assigned SCCmec type IV by methods 2 and 3, while 15.54% (30/193) of the MRSA isolates were designated as SCCmecury by methods 1, 2 and 3.
These observations indicated that the assessed M-PCR methods were able to assign a specific SCCmec type to the same MRSA isolates, most of the remaining isolates were designated different SCCmec types by the methods investigated. In a separate experiment, an attempt to categorize the SCCmec types defined by each SCCmec typing method in this study revealed that there was no specific distribution pattern of SCCmec type(s) among the pulsed field gel electrophoresis derived pulsotypes (data not shown) suggesting that there was no specific association between the chromosomal DNA content of the MRSA isolates and the SCCmec type assigned by the methods evaluated.
A spectacular instance of misassigned ST398-SCCmec III MRSA isolates that took about two years to be reassigned as SCCmec type V has been previously reported (van Loo et al., 2007; Jansen et al., 2009) Such incidence would include a redesignation of the isolates from SCCmec III to SCCmec V based on the molecular typing criteria (Ito et al., 2001, 2004). This report showed that at least 25.91% of the MRSA isolates was of SCCmec type VI and correlates with a number of recent reports which have indicated an increase in the number of infections associated with SCCmec type IV, V, VII or VIII in the hospital setting (Magilner et al., 2008; David et al., 2010) including the presence of the different genotypes in specific environments (Marchese et al., 2009). Although, the overall epidemiological picture presented in these reports may still be biologically relevant based on the general pattern observed across the different countries involved, the estimated statistics may be misrepresented due to the lack of a unified standard method for SCCmec classification.
The need for standardization of SCCmec typing and genotype designation is evident by a number of reports including: (i) the continuous blurring of the clinical and genetic distinctions between CA-MRSA and HA-MRSA (David et al., 2010; Prosperi et al., 2013) (ii) the probability that CA-MRSA isolates might displace HA-MRSA in future and become the most prevalent strains in clinical settings (Popovich et al., 2008) and (iii) the likelihood for the eventual co-existence of the two MRSA genotypes based on epidemiological modeling (Kouyos et al., 2013). Therefore, the lack of a consensus typing method will make it difficult to predict the actual genetic changes and evolution of the SCCmec elements in S. aureus. A standard and consensus typing method will
ensure accurate epidemiological assessments within and across different countries and effective management and control of MRSA infections.Currently, the classification of SCCmec elements in S. aureus is based on the combination of mec and ccr genes which have variations upon which the different classes of SCCmec elements are inferred (IWG-SCC, 2009).
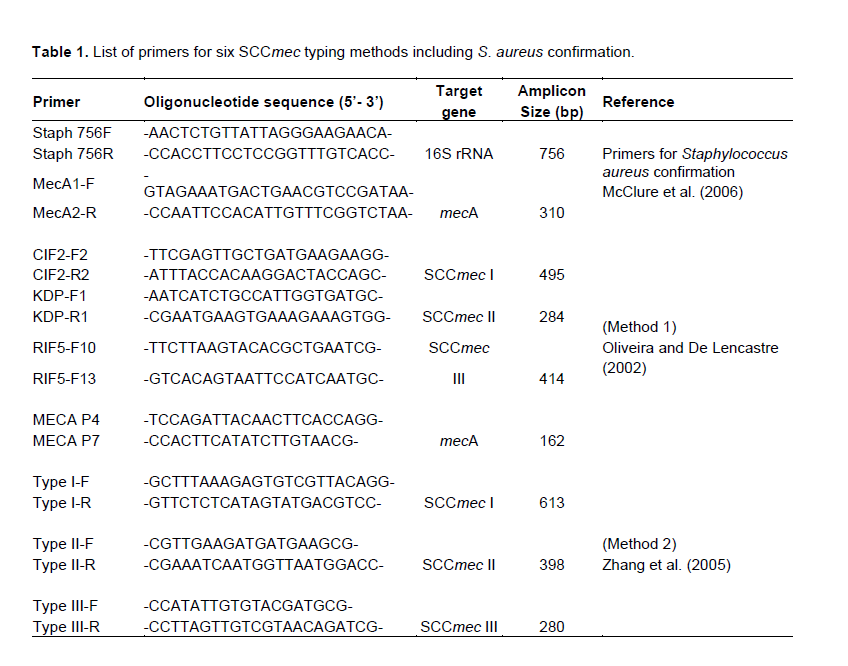
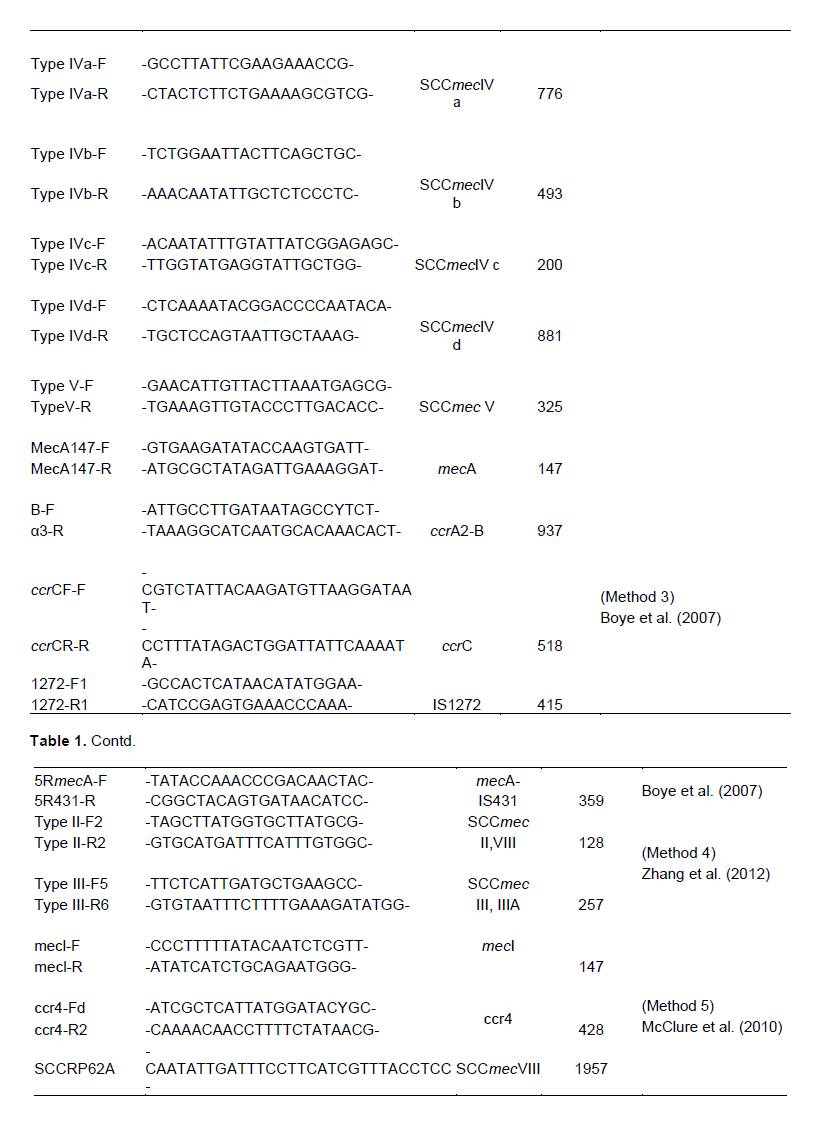
The multiplex PCR method described by Kondo et al. (2007) attempts to improve the accuracy of detection by an initial PCR identification of the mec and cassette chromosome recombinases (ccr) types followed by identifying the genes in the “joining regions” (J-regions). Accordingly, sequence variations in the joining regions are then used to classify SCCmec I-V. There is an ongoing effort to test the performance of this method on clinical MRSA isolates from a number of African countries, in our laboratory. Despite this continuous improvement, consensus criteria for choosing a typing method for SCCmec typing is required.Based on the variations observed in the designation of SCCmec types by various methods targeting different sites and genes within the SCCmec elements, it is obvious that the designation of SCCmec types across different laboratories around the world may not be in synchrony. This is epitomized in the fact that laboratories across the globe adopt different SCCmec typing methods (Table 1).
A recent review indicated that SCCmec typing was recommended as one of the methods for the monitoring of the molecular epidemiology of MRSA at national and international levels (IWG-SCC, 2009). The current study presents one of the challenges in the practicality of such endeavor. A more detailed study primarily designed to compare all published SCCmec typing methods on MRSA strains with known SCCmec sequence information would be required to make informed decision on a consensus M-PCR characterization of the SCCmec element.
While the SCCmec elements described to date include types I-XI, this study focused on the SCCmec types I-V and VIII based on our laboratory dataset on the prevalence of the SCCmec types in Pretoria, South Africa. This work attempts to paint a practical picture of the difficulties encountered in low income laboratories that are still using M-PCR for MRSA genotyping and hence focuses on the mostly reported M-PCR methods as presented in Table 2. Therefore, not all reported M-PCR methods could be covered for an in-depth comparative study.
In conclusion, this report shows the differences in the assigned SCCmec types by the different M-PCR methods as observed in our laboratory. The fact that in spite of the extensive coverage of the variable regions as observed for each method, some clinical isolates could not be SCCmec-typed in the original reports by the authors of these methods was also highlighted.The M-PCR detection of composite SCCmec types in clinical MRSA isolates (SCCmec II + SCCmecury and SCCmec type II+IVc)) was also reported. A plan is underway to investigate the whole genome sequence of these isolates in order to confirm this finding.
From the above discussion, a number of questions thus arise: Is the inability to type clinical strains by SCCmec method attributed to different structural types or rearrangement and/or recombination of known SCCmec elements? Is there still a clinical-epidemiological relevance of HA-MRSA and CA-MRSA differentiation using SCCmec element, considering the reported blurring of the distinction (Peterson et al., 2012) between these two categories? If yes, do we have a consensus algorithm for making this distinction? Is SCCmec element still a reliable tool for typing MRSA isolates as previously suggested (IWG-SCC, 2009) taking into consideration the variations in the nucleic acid content of this element and the associated discrepancies in identification? While it is obvious that diagnostic microarray, sequencing of SCCmec elements and whole genome sequencing are among the modern methods of choice that may resolve this problem, majority of the laboratories in low income countries of Africa are still not able to afford the routine use of these methods. As a way forward, the adoption of a consensus method in South Africa and Africa in general is recommended, in order to allow effective epidemio-logical data comparison.
CONFLICT OF INTERESTS
ACKNOWLEDGEMENT
REFERENCES
|
Boye K, Bartels MD, Andersen IS, Moller JA, Westh H (2007). A new multiplex PCR for easy screening of methicillin-resistant Staphylococcus aureus SCCmec types I-V. Clin. Microbiol. Infect. 13:725-727. |
|
|
Daum RS, Ito T, Hiramatsu K, Hussain F, Mongkolrattanothai K, Jamklang M, Boyle-Vavra S (2002). A novel methicillin-resistance cassette in community-acquired methicillin-resistant Staphylococcus aureus isolates of diverse genetic backgrounds. J. Infect. Dis. 186:1344-1347. |
|
|
David MZ, Daum RS (2010). Community-associated methicillin-resistant Staphylococcus aureus: epidemiology and clinical consequences of an emerging epidemic. Clin. Microbiol. Rev. 23:616-87. |
|
|
International Working Group on the Classification of Staphylococcal Cassette Chromosome Elements (IWG-SCC) (2009). Classification of staphylococcal cassette chromosome mec (SCCmec): guidelines for reporting novel SCCmec elements. Antimicrob. Agents Chemother. 53:4961-4967. |
|
|
Ito T, Katayama Y, Asada K, Mori N, Tsutsumimoto K, Tiensasitorn C, Hiramatsu K (2001). Structural comparison of three types of staphylococcal cassette chromosome mec integrated in the chromosome in methicillin-resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 45:3677. |
|
|
Ito T, Ma XX, Takeuchi F, Okuma K, Yuzawa H, Hiramatsu K (2004). Novel type V staphylococcal cassette chromosome mec driven by a novel cassette chromosome recombinase, ccrC. Antimicrob. Agents Chemother. 48: 2637-2651. |
|
|
Jansen MD, Box ATA, Fluit AC (2009). SCCmec typing in methicillin-resistant Staphylococcus aureus strains of animal origin. Emerg. Infect. Dis. 15:136. |
|
|
Kim J (2009). Understanding the evolution of methicillin resistant Staphylococcus aureus. Clin. Microbiol. Newsletter. 31:17-23. |
|
|
Kondo Y, Ito T, Ma X X, Watanabe S, Kreiswirth B N, Etienne J, Hiramatsu K (2007). Combination of multiplex PCRs for staphylococcal cassette chromosome mec type assignment: rapid identification system for mec, ccr, and major differences in junkyard regions. Antimicrob. Agents Chemother. 51:264-274. |
|
|
Kouyos R, Klein E, Grenfell B (2013). Hospital-community interactions foster coexistence between methicillin-resistant strains of Staphylococcus aureus. PLOS Pathog. 9:e1003134. |
|
|
Lo WT, Wang CC (2011). Panton-Valentine leukocidin in the pathogenesis of community-associated methicillin resistant Staphylococcus aureus infection. Pediatr. Neonatol. 52:59-65. |
|
|
Magilner D, Byerly MM, Cline DM (2008). The prevalence of community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) in skin abscesses presenting to the pediatric emergency department. NC Med. J. 69:351-354. |
|
|
Marchese A, Gualco L, Maioli E, Debbia E (2009). Molecular analysis and susceptibility patterns of meticillin-resistant Staphylococcus aureus (MRSA) strains circulating in the community in the Ligurian area, a northern region of Italy: emergence of USA300 and EMRSA-15 clones. Int. J. Antimicrob. Ag. 34:424-428. |
|
|
McClure JA, Conly JM, Elsayed S, Zhang K (2010). Multiplex PCR assay to facilitate identification of the recently described Staphylococcal cassette chromosome mec type VIII. Mol. Cell. Probe 24:229-232. |
|
|
McClure JA, Conly JM, Lau V, Elsayed S, Louie T, Hutchins W, Zhang K (2006). Novel multiplex-PCR assay for detection of the staphylococcal virulence marker Panton- Valentine leukocidin genes and simultaneous discrimination of methicillin susceptible from resistant staphylococci. J. Clin. Microbiol. 44: 1141-1144. |
|
|
Milheiriço C, Oliveira DC, de Lencastre H (2007). Multiplex PCR strategy for subtyping thestaphylococcal cassette chromosome mec type IV in methicillin-resistant Staphylococcus aureus: 'SCCmec IV multiplex'. J. Antimicrob. Chemother. 60:42-48. |
|
|
Morrison MA, Hageman JC, Klevens RM (2006). Case definition for community-associated methicillin-resistant Staphylococcus aureus. J. Hosp. Infect. 62:241. |
|
|
Moussa IMI, Kabli SA, Hemeg HA, Al-Garni SM, Shibl AM (2012). A novel multiplex PCR for molecular characterization of methicillin resistant Staphylococcus aureus recovered from Jeddah, Kingdom of Saudi Arabia. Indian J. Med. Microbiol. 30:296-301. |
|
|
Naimi TS, LeDell K.H, Como-Sabetti K, Borchardt SM, Boxrud DJ, Etienne J, Susan K, Lynfield R (2003). Comparison of community-and health care–associated methicillin-16 resistant Staphylococcus aureus infection. JAMA. 290:2976-2984. |
|
|
O'Brien FG, Pearman JW, Gracey M, Riley TV, Grubb WB (1999). Community strain of methicillin-resistant Staphylococcus aureus involved in a hospital outbreak. J. Clin. Microbiol. 37:2858-2862. |
|
|
Oliveira DC, de Lencastre H (2002). Multiplex PCR strategy for rapid identification of structural types and variants of the mec element in methicillin-resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 46:2155-2161. |
|
|
Paterson GK, Harrison EM, Holmes MA (2013). The emergence of mecC methicillin-resistant Staphylococcus aureus. Trends Microbiol. 22:42-47. |
|
|
Peterson AE, Davis MF, Julian KG, Awantang G, Greene WH, Price LB, Andrew W, Whitener CJ (2012). Molecular and phenotypic characteristics of healthcare-and community associated methicillin-resistant Staphylococcus aureus at a rural hospital. PloS one. 7:e38354. |
|
|
Popovich KJ, Weinstein RA, Hota B (2008). Are community-associated methicillin-resistant Staphylococcus aureus (MRSA) strains replacing traditional nosocomial MRSA strains. Clin. Infect. Dis. 46:787-794. |
|
|
Prosperi M, Veras N, Azarian T, Rathore M, Nolan D, Rand K, Cook RL, Johnson J, Morris JG, Jr., .Salemi M (2013). Molecular epidemiology of community-associated methicillin-resistant Staphylococcus aureus in the genomic era: a cross-sectional study. Sci Rep. 3:1902. |
|
|
Saiman L, O'Keefe M, Graham PL, Wu F, Said-Salim B, Kreiswirth B, LaSala A, Schlievert PM, Della-Latta P (2003). Hospital transmission of community-acquired methicillin-resistant Staphylococcus aureus among postpartum women. Clin. Infect. Dis. 37:1313-1319. |
|
|
Shore AC, Coleman DC (2013). Staphylococcal cassette chromosome mec: Recent advances and new insights. Int. J. Med. Microbiol. 303:350-359. |
|
|
Song JH, Hsueh PR, Chung DR, Ko KS, Kang CI, Peck KR, Yeom JS., Kim SW,Chang HH, Kim YS, Jung SI, Son JS, So TMK, Lalitha MK, Yang YH, Huang SG,Wang H, Lu QA, Carlos CC, Perera JA, Chiu CH, Liu JW, Chongthaleong A,Thamlikitkul V, Van PH, Grp AS (2011). Spread of methicillin-resistant Staphylococcus aureus between the community and the hospitals in Asian countries: an ANSORP study. J. Antimicrob. Chemother. 66:1061-1069. |
|
|
Stefani S, Chung, DR, Lindsay J A, Friedrich AW, Kearns AM, Westh H, MacKenzie FM (2012). Meticillin-resistant Staphylococcus aureus (MRSA): global epidemiology and harmonisation of typing methods. Int. J. Antimicrob. Agents 39:273-282. |
|
|
van Loo I, Huijsdens X, Tiemersma E, de Neeling A, van de Sande-Bruinsma N, Beaujean D, Voss A, Kluytmans J (2007). Emergence of methicillin-resistant Staphylococcus aureus of animal origin in humans. Emerg. Infect. Dis. 13:1834-1839. |
|
|
Weber JD (2005). Community-associated methicillin resistant Staphylococcus aureus. Clin. Infect. Dis. 41:269-72. |
|
|
Zhang KY, McClure JA, Conly JM (2012). Enhanced multiplex PCR assay for typing of staphylococcal cassette chromosome mec types I to V in methicillin-resistant Staphylococcus aureus. Mol. Cell Probe. 26:218-221. |
|
|
Zhang KY, McClure JA, Elsayed S, Louie T, Conly JM (2005). Novel multiplex PCR assay for characterization and concomitant subtyping of staphylococcal cassette chromosome mec types I to V in methicillin-resistant Staphylococcus aureus. J. Clin. Microbiol. 43:5026-5033. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


