Full Length Research Paper

ABSTRACT
Bacteria-parasite association has been documented as a factor that is responsible for continued and prolonged bacterial infection, such as typhoid and paratyphoid fever in schistosomiasis patients. This work aimed to determine the presence of typhoid and paratyphoid Salmonella among schistosomiasis patients and to evaluate the efficacy of Widal test on such population. A cross sectional descriptive study was conducted between November 2005 and May 2006 in Managil region, Gezira State, Sudan. A total of 203 males participated in the study. Urine, stool and blood samples were collected and processed for the investigation of schistosomiasis and Salmonella infection based on standard methods. Widal test was performed to estimate diagnostic cut-off value of enteric fever. Of the 203 studied subjects, 42 (20.7%) were diagnosed with Schistosoma haematobium, whereas eight (3.9%) had Schistosoma mansoni infection. Of these, Salmonella species were detected in 30 (60%) cases, of which Salmonella typhi represented 63.3%, followed by Salmonella paratyphi A and B (16.7%, each) and Salmonella paratyphi C (3.3%). Based on the culture results (n=30) as a diagnostic method used for enteric fever, Widal test was positive in 12 cases, with a sensitivity of 40% and specificity of 75%. Of the Widal positive cases, titers of 1:160, 1:320, 1:640 were detected in 58.3, 33.3 and 8.3% of samples, respectively. In schistosomiasis endemic regions, enteric fever was associated with schistosomiasis, which requires investigation of both infections concomitantly. Regardless of the low sensitivity of Widal test, titer of ≥1/160 is a diagnostic value for enteric fever in this study group.
Key words: Schistosomiasis, typhoid and paratyphoid Salmonella, detection, Widal test, Sudan.
INTRODUCTION
Typhoid and paratyphoid fever (enteric fever) is an acute systemic infection caused mainly by the bacterium, Salmonella enteric serotype typhi and other serotypes of Salmonella paratyphi A, B, and C (Chart et al., 2007; Buckle et al., 2012). It continues to be a global health problem, especially in the tropics and sub tropic countries; over 27 million persons suffer from this disease annually (Buckle et al., 2012). Schistosomiasis is atropical parasitic disease caused by blood fluke worms of the genus Schistosoma such as S. haematobium and S. mansoni (Dabo et al., 2011). Schistosoma infection is endemic in many sub-Saharan African countries where the introduction of river regulation and irrigated agriculture commonly results in increasing distribution and prevalence of schistosomiasis (King et al., 2005). The association between bacteria-parasite has been observed as a factor that results in prolonged bacterial infection, such as typhoid and paratyphoid fever in schistosomiasis patients (Lambertucci et al., 1998; Bouree et al., 2002). Concurrent Schistosoma-Salmonella infections appear when Salmonella species enter the systemic circulation and adhere to the tegument of adult Schistosoma through the fimbriae. This interaction can lead to a massive release of occult Salmonella (Barnhill et al., 2011). Examinations with the scanning electron microscope showed that pili function by joining Salmonella to the surface tegument of S. mansoni and S. haematobium (LoVerde et al., 1980). Typhoid and paratyphoid Salmonella is easily recovered from the blood, feces or urine samples of schistosomiasis patients (Lambertucci et al., 1998). Moreover, enteric fever can be diagnosed by different laboratory methods, including serological tests such as Widal agglutinations or ELISA, culture of clinical specimens of stool, blood and urine (Chart et al., 2007). The Widal test, which detects agglutinating antibodies to somatic lipopolysaccharide O antigens and flagella H antigens was introduced over a century ago and remains a widely used tool for the serological diagnosis of enteric fever (el-Shafie, 1991; House et al., 2001). In Sudan, despite the high endemicity of both schistosomiasis and enteric fever (el-Shafie, 1991; Ahmed et al., 2012; Ibrahim and Ibrahim, 2014), there is little available data on Schistosoma-Salmonella infections (Salih et al., 1977). Therefore, the present study aimed to determine the presence of typhoid and paratyphoid Salmonella among schistosomiasis patients in Managil region, Central Sudan and to detect the most common Salmonella serotypes that cause enteric fever. In addition, it aimed to evaluate the efficacy of the Widal agglutination test used for the diagnosis of enteric fever comparable to cultural methods.
MATERIALS AND METHODS
Study area and population
This is a descriptive cross sectional study conducted between November, 2005 and May, 2006 in Managil Region (156 km South of Khartoum Capital), Gezira State, Central Sudan. The state is an endemic area for schistosomiasis due to the agricultural activities of the populations in the Gezira-Managil irrigation schemes (Hilali et al., 1995). A total of 203 males between 10 to 55 years old participated in the study. The studied subjects were students of the Quran school (n = 148), employees (n = 28) and farmers (n = 27). Those who were previously infected with the infection or under treatment were excluded from the study. Each participant accepted and agreed to participate in the study after informing his parentsabout the importance of the study. The study was approved by the Committee of Research Council of Faculty of Medical Laboratory Sciences, University of Khartoum.
Samples processing
Clinical samples of urine, stool and blood were collected from each individual and processed for the investigation of schistosomiasis and typhoid and paratyphoid Salmonella infection. About 20 ml of urine was collected in sterile plastic container from each subject suspected to have urinary schistosomiasis. To obtain the stool samples, each individual was given a dry and clean container to provide at least 10 g of sample. Stool and urine samples were obtained from each individual, between 10 am and 2 pm, when highest egg excretion occurs (Cheesbrough, 2000b). The diagnosis of Schistosoma infection was carried out in the study field by applying direct microscopic examination of the samples. Two smears were prepared from each stool sample and examined for the presence of S. mansoni eggs using standard Kato-Katz method (Katz et al., 1972). The urine centrifugation technique was used to detect the presence S. haematobium eggs as previously described (Cheesbrough, 2000b). Then, about 5 ml of venous blood was collected from each subject, having schistosomiasis in a clean, dry sterile plain tube, and allowed to clot at room temperature. The sera were separated by centrifugation at 13,000 rpm for 5 min, transferred into clean, sterile plain tubes, and stored at -20°C for further Widal agglutination test.
Each sample of urine or stool yielded positive result; schistosomiasis was cultured immediately in 5 ml of sterile selenite F broth (SFB) (Oxoid, Basingstoke, England) for further isolation and identification of possible pathogens of typhoid and paratyphoid Salmonella at the Research Laboratory of Faculty of Medical Laboratory, University of Khartoum.
Isolation and identification of Salmonella species
Isolation of Salmonella species from urine and stool samples was done by following the standard laboratory methods (Cheesbrough, 2000a). All the samples containing SFB were sub-cultured on xylose lysine deoxycholate (XLD) (Oxoid, Basingstoke, England) and deoxycholate citrate agar (DCA) (Oxoid, Basingstoke, England). They were incubated overnight at 37°C. The plates were then examined for the presence of non-lactose fermenting colonies. Suspected colonies of Salmonella isolates were identified on the bases of colonial morphology, gram staining, biochemical tests, and they were confirmed serologically using monovalent and polyvalent antisera (Cheesbrough, 2000a).
Widal test for investigating enteric fever
Widal agglutination test was performed to examine Salmonella serotypes using O and H antigens of Salmonella typhi and Salmonella paratyphi A, B and C antigens as described by House et al. (2001). Before carrying out the test, the serum samples (n=50) were divided into two categories: group A collected from culture proven cases and group B from culture negative cases. Widal agglutination reagent kits (Plasmetec, UK) test was performed in both groups according to the manufacturer's instruction. Briefly, each serum sample was diluted serially starting from 1:80 to 1:1280 with 0.85 NaCl in two rows of test tubes for the detection of O and H agglutination. Single drops of O and H antigens were added to corresponding tubes and were incubated at 37°C in a water bath for 18-24 h. The tubes were examined macroscopically and microscopically for the presence of agglutination. Partial or complete agglutination with variabledegrees of clearing the supernatant fluid was recorded as a positive result.
Statistical analysis
Data were analyzed using SPSS for Windows version 10.0 (SPSS Inc., Chicago, IL, USA). The prevalence and descriptive analysis was calculated. Considering culture results as the standard method, the sensitivity and specificity of the Widal test results were interpreted and calculated using the following formulas:
Sensitivity is a/(a+c), specificity is d/(d+b),
Where, a is test positive and true culture positive, b is test positive and true culture negative, c is test negative and true culture positive, and d is test negative and true culture negative.
RESULTS
Of the 203 subjects whose urine and stool samples were screened for the presence of Schistosoma eggs, 50 (24.6%) were found to be infected with schistosomiasis. The majority of the positive cases were students (n = 46), followed by farmers (n = 3) and the employee (n = 1). Out of the 203-screened subjects, 42 (20.7%) cases were caused by S. haematobium, and 8 (3.9%) cases were due to S. mansoni infection.
Distribution of Salmonella serotypes among schistosomiasis patients
A total of 50 urine and stool samples were cultured for the presence of Salmonella organisms. Of these, 30 (60%) samples yielded positive results for different serotypes of Salmonella and were considered as a true positive for the presence of enteric fever. The most common Salmonella serotypes isolated from schistosomiasis patients were S. typhi (63.3%; 19/30), followed by S. paratyphi A and B (16.7%; 5/30, each) and S. paratyphi C (3.3%; 1/30) (Table 1).

Evaluation of Widal agglutination test
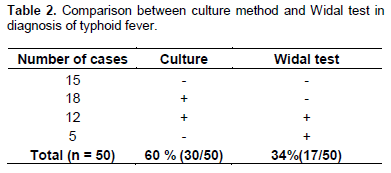
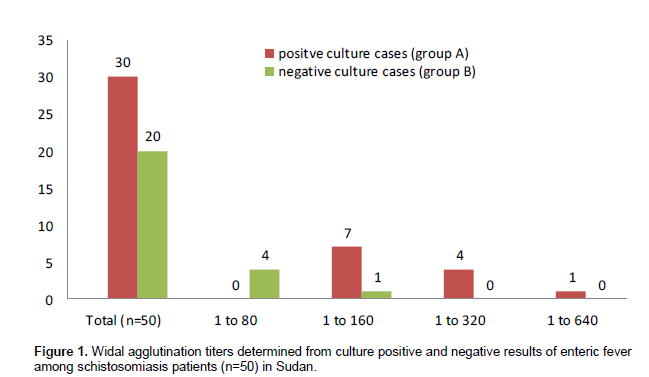
Table 2 summarizes the cultural and serological results obtained from the schistosomiasis patients. Based on the culture results (n = 30) as a diagnostic method for detecting the presence of enteric fever, Widal test was found to be positive in 12 cases (group 1), with a sensitivity of 40% (12/30) and specificity of 75% (15/20). Of the 12 Widal positive cases, titer of 1:160 was detected in seven (58.3%) samples, titer of 1/320 was detected in four (33.3%) samples and titer of 1:640 was detected in one (8.3%) sample. Among the 20 culture negative cases (group 2), four (20%) samples were given anti Salmonella antibody titer of 1:80, whereas titer of 1:160 was detected in one (5%) sample (Figure 1). These findings indicated that titer of equal or more than 1:160 value for both O and H agglutinins is a diagnostic titer for detecting the presence of enteric fever.
DISCUSSION
In our setting, we found that 60% of schistosomiasis patients carried typhoid and paratyphoid Salmonella. The presence of Salmonella organisms in schistosomiasis patients has been reported in other studies (Tuazon et al., 1985; Barnhill et al., 2011). Furthermore, Schistosoma-Salmonella interactions are seen in all species of Schistosoma, notably S. haematobium, S. mansoni, S. intercalatum and S. japonicum (Gendrel, 1993). This association may play an important role in the persistent or delayed Salmonella infections (Bouree et al., 2002). In an earlier study, Gendrel et al. (1986) reported that Salmonella infection was clinically prolonged by bilharziasis in 1 out of 3 patients. This could be explained by a decreased host immune response following schistosomiasis (Bouree et al., 2002). Therefore, bacterium-host-parasite interaction may in part explain why Salmonella infection and schistosomiasis clinically occur frequently together and present difficult therapeutic problem (Young et al., 1973). However, suchinfections need to be treated concomitantly (Gendrel et al., 1986).
Culture methods of clinical specimens remain the most accurate diagnostic procedure for isolating the causative organisms of suspected enteric fever (Chart et al., 2007; Wain and Hosoglu, 2008). In our setting, among the 50 schistosomiasis patients, positive culture results in different types of typhoid, and paratyphoid Salmonella was recorded in 60% (30/50) cases (Table 1). In this study, we found that S. typhi was the most frequent isolate that represented 63.3% of the isolates. Equal isolation rate was recorded for S. paratyphi A and B (16.7%, each), and one (3.3%) isolate was found to be S. paratyphi C. These findings indicate that the incidence of typhoid fever in schistosomiasis patients is more frequent than paratyphoid fever. Similar findings have been reported earlier among Sudanese patients (Salih et al., 1977). Other studies have reported different serotypes of Salmonella among the general population instead of schistosomiasis patients. Shetty et al. (2012) have reported that out of 103 Salmonella isolates, 85 (82.52%) were S. typhi, 16 (15.53%) were Salmonella paratyphi A and two (1.94%) were Salmonella paratyphi B. On the contrary, the isolation rate of S. paratyphi A was 1.5 times higher than that of S. typhi, as reported by others (Palit et al., 2006).
In the present study, among the 30 culture proven cases, 40% yielded significant Widal agglutination reactions. This level is similar to that recorded in Turkey (Hosoglu et al., 2008), but lower than that reported in Pakistan, where the Widal test was positive in 73.68% culture positive cases of enteric fever (Khoharo, 2011). Nevertheless, the Widal agglutination test has been widely used in many developing countries for diagnosing enteric fever, but it has a low sensitivity, specificity, which varies between the geographical areas (House et al., 2001; Omuse et al., 2010). In considering the cultural methods as a gold standard test for the diagnosis of enteric fever, we determined the reliability of the Widal test. We found that its sensitivity was 40%, with a specificity of 75%. This is in line with the results obtained in Bangladesh, where the Widal agglutination test yielded a sensitivity of 42.85% and a specificity of 85.0% (Begum et al., 2009). Likewise, many studies have evaluated the efficacy of the Widal agglutination test (Wain et al., 2008; Ley et al., 2010). Sharing of O and H antigens by other Salmonella serotypes and members of Enterobacteriaceae makes the role of Widal test even more controversial in diagnosing typhoid fever (Hosoglu et al., 2008). In this study, our findings indicated that Widal test has a low sensitivity and specificity; hence the need for alternative methods in order to improve laboratory diagnosis of enteric fever.
The interpretation of the Widal agglutination test becomes problematic, with a great number of articles reporting different diagnostic cut-off values (Wain and Hosoglu, 2008). Since there are no current data available regarding baseline titers of Widal test among schistosomiasis patients in the Sudan, this study was undertaken to compile the baseline titers for these specific populations. Widal agglutination titer of equal or more than 1:160 was represented among all the culture proven cases. These findings confirmed that the titer of equal or more than 1:160 is a diagnostic titer of enteric fever among schistosomiasis patients. In a previous study among healthy population in Sudan, el-Shafie et al. (1991) reported that a titer above 1:320 suggests the diagnosis of S. typhi; 1:160 for both S. paratyphi B and S. paratyphi A. Regardless of schistosomal infections, different cut-off values of Widal test have been recordedas a diagnostic titer for typhoid and paratyphoid fever in other studies (Ley et al., 2010; Omuse et al., 2010). Therefore, in order to use the Widal test effectively, each endemic area should determine the appropriate titer for the diagnosis of typhoid and paratyphoid Salmonella (Willke et al., 2002).
CONCLUSIONS
The study concludes that in schistosomiasis endemic areas, there is a direct relationship between Schistosoma - Salmonella infection that needs routine screening for the presence of typhoid and paratyphoid fever among schistosomiasis patients. In our setting, S. typyi was found to be the most Salmonella organisms causing this syndrome (63.3%). Bacteriological techniques are more sensitive and accurate than the serological test in the diagnosis of Schistosoma -Salmonella relationship. Regardless of the low sensitivity of Widal test, titer of equal or more than 1:160 is a diagnostic cut-off value for enteric fever in this study group.
CONFLICT OF INTERESTS
The authors did not declare any conflict of interest.
ACKNOWLEDGEMENT
The authors express gratitude to all staff members of the Departments of Medical Microbiology, Faculty of Medical Laboratory Science, and University of Khartoum.
REFERENCES
|
Ahmed AM, El Tash LA, Mohamed EY, Adam I (2012). High levels of Schistosoma mansoni infections among schoolchildren in central Sudan one year after treatment with praziquantel. J. Helminthol. 86(2):228-232. |
|
|
Barnhill AE, Novozhilova E, Day TA, Carlson SA (2011). Schistosoma-associated Salmonella resist antibiotics via specific fimbrial attachments to the flatworm. Parasit. Vectors 4:123. |
|
|
Begum Z, Hossain MA, Musa AK, Shamsuzzaman AK, Mahmud MC, Ahsan MM, Sumona AA, Ahmed S, Jahan NA, Alam M, Begum A (2009). Comparison between DOT EIA IgM and Widal Test as early diagnosis of typhoid fever. Mymensingh Med. J. 18:13-17. |
|
|
Bouree P, Botterel F, Romand S (2002). Delayed Salmonella bacteriuria in a patient infected with Schistosoma haematobium. J. Egypt Soc. Parasitol. 32(2):355-360. |
|
|
Buckle GC, Walker CL, Black RE (2012). Typhoid fever and paratyphoid fever: Systematic review to estimate global morbidity and mortality for 2010. J. Glob. Health 2(1):010401. |
|
|
Chart H, Cheasty T, de Pinna E, Siorvanes L, Wain J, Alam D, Nizami Q, Bhutta Z, Threlfall EJ (2007). Serodiagnosis of Salmonella enterica serovar Typhi and S. enterica serovars Paratyphi A, B and C human infections. J. Med. Microbiol. 56(9):1161-1166. |
|
|
Cheesbrough M (2000a) Microbiological tests. In: District Laboratory Practice in Tropical Countries Part II. Cambridge University Press, Cambridge. |
|
|
Cheesbrough M (2000b) Parasitological tests. In: District Laboratory Practice in Tropical Countries Part I. Cambridge University Press, Cambridge. |
|
|
Dabo A, Badawi HM, Bary B, Doumbo OK (2011). Urinary schistosomiasis among preschool-aged children in Sahelian rural unities in Mali. Parasit. Vectors 4:21. |
|
|
el-Shafie S (1991). The Widal test in a normal healthy population in the Sudan. East. Afr. Med. J. 68(4):266-269. |
|
|
Gendrel D (1993). [Salmonella-Schistosoma interactions]. Rev. Prat. 43(4):450-452. |
|
|
Gendrel D, Richard-Lenoble D, Nardou M, Moreno JL, Kombila M, Engohan E, Moussavou A, Galliot A, Toure R (1986). Interaction between Salmonella and Schistosoma intercalatum. Presse. Med. 15(15):689-692. |
|
|
Hilali AH, Madsen H, Daffalla AA, Wassila M, Christensen NO (1995). Infection and transmission pattern of Schistosoma mansoni in the Managil irrigation scheme, Sudan. Ann. Trop. Med. Parasitol. 89(3):279-286. |
|
|
Hosoglu S, BoÅŸnak V, Akalin S, Geyik MF, Ayaz C (2008). Evaluation of false negativity of the Widal test among culture proven typhoid fever cases. J. Infect. Dev. Ctries. 2(6):475-478. |
|
|
House D, Wain J, Ho VA, Diep TS, Chinh NT, Bay PV, Vinh H, Duc M, Parry ChM, Dougan G, White NJ, Hien TT, Farrar JJ (2001). Serology of typhoid fever in an area of endemicity and its relevance to diagnosis. J. Clin. Microbiol. 39(3):1002-1007. |
|
|
Ibrahim AM, Ibrahim ME (2014). Evaluation of microscopical and serological techniques in the diagnosis of Schistosoma mansoni infection at Sennar State, central Sudan, Asian Pac. J. Trop. Dis. 4:8-13. |
|
|
Katz N, Chaves A, Pellegrino J (1972). A simple device for quantitative stool thicksmear technique in schistosomiasis mansoni. Rev. Inst. Med. Trop. Sao Paulo 14(6):397-400. |
|
|
Khoharo HK (2011). A comparative study of the typhidot (Dot-EIA) and Widal tests in blood culture positive cases of typhoid fever. Trop. Doct. 41(3):136-138. |
|
|
King CH, Dickman K, Tisch DJ (2005). Reassessment of the cost of chronic helmintic infection: a meta-analysis of disability-related outcomes in endemic schistosomiasis. Lancet. 365(9470):1561-1569. |
|
|
Lambertucci JR, Rayes AAM, Serufo JC, Gerspacher-Lara R, Brasileiro-Filho G, Teixeira R, Antunes CMF, Goes AM, PCoelho PMZ (1998). Schistosomiasis and associated infections. Mem. Inst. Oswaldo Cruz. 93 (Suppl 1): 135-139. |
|
|
Ley B, Mtove G, Thriemer K, Amos B, von Seidlein L, Hendriksen I, Mwambuli A, Shoo A, Malahiyo R, Ame SM, Kim DR, Ochiai LR, Clemens JD, Reyburn H, Wilfing H, Magesa S, Deen JL (2010). B Evaluation of the Widal tube agglutination test for the diagnosis of typhoid fever among children admitted to a rural hdospital in Tanzania and a comparison with previous studies.MC Infect. Dis. 10:180. |
|
|
LoVerde PT, Amento C, Higashi GI (1980). Parasite-parasite interaction of Salmonella typhimurium and Schistosoma. J. Infect. Dis. 141(2):177-185. |
|
|
Omuse G, Kohli R, Revathi G (2010). Diagnostic utility of a single Widal test in the diagnosis of typhoid fever at Aga Khan University Hospital (AKUH), Nairobi, Kenya. Trop. Doct. 40(1): 43-44. |
|
|
Palit A, Ghosh S, Dutta S, Sur D, Bhattacharya MK, Bhattacharya SK (2006). Increasing prevalence of Salmonella enterica serotype Paratyphi-A in patients with enteric fever in a periurban slum setting of Kolkata, India. Int. J. Environ. Health Res. 16(6):455-459. |
|
|
Salih SY, Subaa HA, Asha HA, Satir AA (1977). Salmonellosis complicating schistosomiasis in the Sudan. J. Trop. Med. Hyg. 80(1):14-18. |
|
|
Shetty AK, Shetty IN, Furtado ZV, Antony B, Boloor R (2012). Antibiogram of salmonella isolates from blood with an emphasis on nalidixic Acid and chloramphenicol susceptibility in a tertiary care hospital in coastal karnataka: a prospective study. J. Lab. Physicians. 4(2): 74-77. |
|
|
Tuazon CU, Nash T, Cheever A, Neva F (1985). Interaction of Schistosoma japonicum with Salmonellae and other gram-negative bacteria. J. Infect. Dis. 152(4): 722-726. |
|
|
Wain J, Diep TS, Bay PV, Walsh AL, Vinh H, Duong NM, Ho VA, Hien TT, Farrar J, White NJ, Parry CM, Day NP (2008). Specimens and culture media for the laboratory diagnosis of typhoid fever. J. Infect. Dev. Ctries. 2(6):469-474. |
|
|
Wain J, Hosoglu S (2008). The laboratory diagnosis of enteric fever. J. Infect. Dev. Ctries. 2(6):421-425. |
|
|
Willke A, Ergonul O, Bayar B (2002). Widal test in diagnosis of typhoid fever in Turkey. Clin. Diagn. Lab. Immunol. 9(4):938-941. |
|
|
Young SW, Higashi G, Kamel R, el-Abdin AZ, Mikhail IA (1973). Interaction of salmonellae and schistosomes in host-parasite relations. Trans. R. Soc. Trop. Med. Hyg. 67:797-802. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


