ABSTRACT
Campylobacter is a major agent of gastroenteritis worldwide. The incidence and prevalence of campylobacteriosis have been increasing in both developed and developing countries over the last decade. In this study, 197 strains of successive Campylobacter-like were identified in French laboratories in September 2018. Bacterial isolates from clinical samples were identified with a mass spectrometer (Ultraflex III TOF/TOF and the BIOTYPER database from Bruker Daltonics). Of the 197 isolates tested, 143 were identified as Campylobacter jejuni (72.59%), 28 as Campylobacter coli (14.21%), 2 as Arcobacter butzleri (1.02%), 1 as Campylobacter fetus and 1 as Campylobacter lari with (0.51% each) by the MALDI-TOF mass spectrometry. Isolation rate of Campylobacter was highest in the 0 - 9 age group (22%). The proportion of male and female patients was 59.4% (CI 95% = 52.2-66.3) and 40.6% (CI 95% = 33.7-42.8) respectively. Sixty strains (30.5%) were resistant to tetracycline and 52 (26.4%) resistant to ampicillin. This study showed that the MALDI-TOF mass spectrometry is a rapid and accurate identification method of Campylobater spp in patients treated in private French laboratories.
Key words: Campylobacter, identification, MALDI-TOF, patients, France.
Campylobacter enteritis was first identified by Butzer in the early 1970s. This pathogen is considered as one of the leading bacterial species of foodborne diseases in humans around the world (Abdi-Hachesoo et al., 2014; CNRCH, 2018). As a result, campylobacteriosis is a major public health concern in many developed countries (Wardak et al., 2007) and in developing countries infection has strikingly increased in recent years (Ewnetu and Mihret, 2010; Gwimi et al., 2015). Human campylobacteriosis has been linked to mishandling and consumption of contaminated poultry (Humphrey et al., 2007). Among the pathogenic species, Campylobacter jejuni and Campylobacter coli are leading causes of foodborne gastroenteritis and enteritis in humans worldwide (Friedman et al., 2000; Reddy and Zishiri 2007). In most European countries, the majority of Campylobacter infections are domestically acquired (EFSA, 2010). Thus, in 2017 several species of Campylobacter with a dramatic increase of C. jejuni were isolated in many blood cultures of patients. Nevertheless, C. jejuni along with C. coli and C. fetus, mostly isolated in stool, remain the common Camplylobacter of human pathogens (CNRCH, 2018). Similarly, other Campylobacter spp. such as Campylobacter lari and Campylobacter upsaliensis have been implicated in human gastrointestinal infections (Obeng et al., 2012; CDC, 2013).
Most Campylobacter enteric infections are self-limited and do not require antimicrobial drug treatment. However, because of severe or long-lasting Campylobacter infections their treatment may require antimicrobial drug therapy (Gallay et al., 2007). Therefore, macrolides as first-line therapy and fluoroquinolones as alternative therapy are recommended (Nachamkin and Blaser, 2000; Gallay et al., 2007). However, the resistance of Campylobacter to antimicrobial agents has substantially increased during the past two decades and become a matter of concern in severe human Campylobacter infections (Lucey et al., 2002; Nachamkin et al., 2002). The objectives of the present study were therefore 1) to identify Campylobacter species in patients consulted in private laboratories in France, using the MALDI-TOF method and 2) to test the bacteria's susceptibility to antimicrobials. With the low identification rates and continuous resistance of pathogenic bacteria species to antibiotics, an accurate and efficient analytical method such as MALDI-TOF MS will be a robust tool for controlling the extend of bacterial infections in both developed and developing countries.
Bacterial strains
A total of 197 Campylobacter-like strains were collected in September 2018 by CNR. Each strain was identified after being subcultured on a trypticase soy blood agar plate (bioMérieux, Marcy l’Etoile, France) and incubated overnight in a microaerobic atmosphere at 37°C. A typical Campylobacter colonies obtained were used for mass spectrometry identification.
Mass spectrometry identification
Sample preparation
A part of a colony of each isolate, taken directly from the agar plate after 18-24 h of incubation to obtain fresh bacteria, was deposited on a microtitre 384 target plate ground steel T F, (Bruker Daltonics, Bremen, Germany) in a single spot and allowed to dry at room temperature. One microlitre of matrix solution (saturated solution of a cyano-4-hydroxycinnamic acid in 50% acetonitrile) was added to the sample and was then crystallized through air-drying at room temperature for 5 min.
MALDI-TOF mass spectrometry measurements
MALDI-TOF mass spectrometry measurements were performed with an Ultraflex III TOF/TOF mass spectrometer (Bruker Daltonics) equipped with a 200-Hz smartbeam 1 laser. The parameter settings were as follows: delay, 80 ns; ion source, 1 volt, 25 kV; ion source, 2 volts, 23.4 kV; lens voltage, 6 kV; and mass range, 0-20 137 kDa. Each run included an Escherichia coli control sample provided by Bruker Daltonics where the presence of eight specific proteins insured that the spectrometer was set properly. Raw spectra of the strains were analysed by MALDI BIOTYPER 2.0 software (Bruker Daltonics) using the default settings (all of the settings were potentially adjustable). The whole process from MALDI-TOF mass spectrometry measurement to identification was performed automatically without any user intervention. Briefly, the software generated a list of peaks up to 100. The threshold for peak acceptance was a signal-to-noise ratio of 3. After alignment, peaks with a mass-to-charge ratio difference of <250 ppm were considered to be identical. The peak list generated was used for matches against the reference library, by directly using the integrated pattern-matching algorithms of the software. All parameters were the same regardless of the presumptive bacterial species analysed. Concerning Campylobacter and related species, the BIOTYPER 2.0 database was composed of four Arcobacter butzleri, two A. cibarius, two A. cryaerophilus, one A. halophilus, one A. nitrofigilis, two A. skirrowii, three Campylobacter coli, five C. fetus, four C. helveticus, two C. hyointestinalis, six C. jejuni, four C. lari, one C. sputorum and four C. upsaliensis. The spectra were obtained in the positive linear mode after 1000 shots (size, 61 794 points; delay, 232 points). A score was attributed to each identification. When this score was >2.00, the identification was considered correct at the species level; between 1.7 and 1.999, the identification was considered correct at the genus level; and <1.7, the identification was not similar enough to a spectrum to draw a conclusion.
Antimicrobial susceptibility test
The antimicrobial susceptibility was performed by the agar diffusion method according to the criteria proposed by the CA-SFM and harmonized according to the criteria proposed by EUCAST (EUCAST, 2018): MH-F medium (Mueller-Hinton + 5% defibrinated horse blood and 20 mg/L β-NAD) (bioMérieux, Marcy l’Etoile, France) was used with an inoculum corresponding to 0.5 McFarland. Six antibiotics belonging to five families were tested: Ampicillin, Amoxicillin- clavulanic acid (beta-lactams), ciprofloxacin (quinolones), erythromycin (macrolides), tetracycline (cyclines) and gentamicin (aminosides). The plates were incubated in microaerobic atmosphere conditions at 35 ± 2°C, 24 h in microaerobic jar conditions (generation of atmosphere using a Anoxomat (Smart)). The reading at 24 h (or 48 h) was performed using the SIRScan system (I2A, Montpellier, France) then visual verification of the diameters read on the camera. A biologist always checks the values read. At the validation, any discrepancy with the result reported by the correspondent was verified and if necessary indicated on the final report. Campylobacter jejuni ATCC 33560 was used as quality control.
Data processing
Data were analyzed using the software package Epi Info 7.1.2.0 (Centers for Disease Control and Prevention [CDC], Atlanta). Multivariable logistic regression was used to estimate odds ratios (ORs) with 95% confidence intervals (95% CI) also calculated. The statistical significance was evaluated using the Fischer exact 2-tailed p value, and a p ≤ 0.05 was considered significant.
Campylobacter isolated in patients
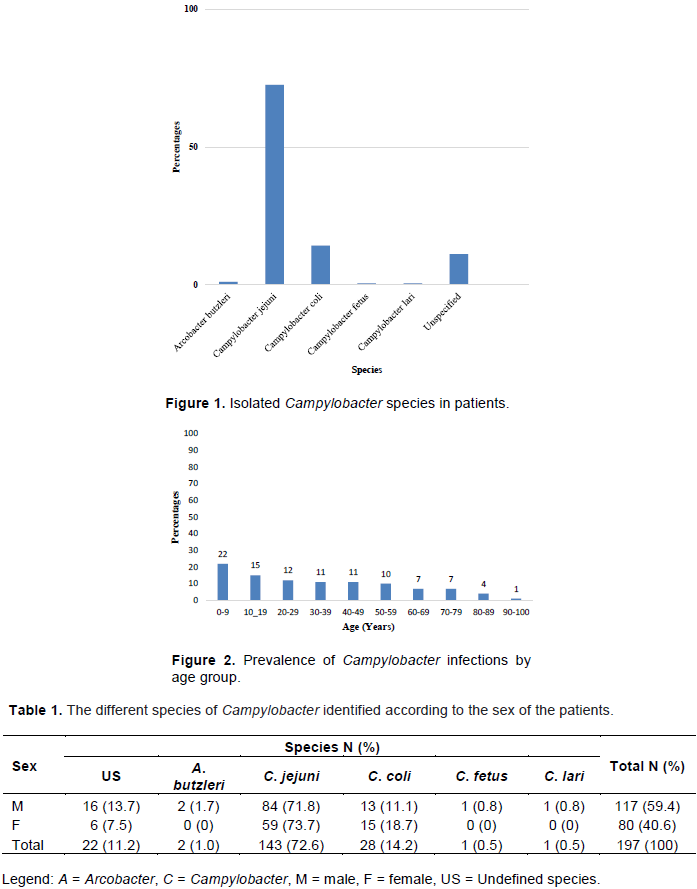
Of the 197 isolates tested, 143 were identified as Campylobacter jejuni (72.59%), 28 as C. coli (14.21%), 2 as Arcobacter butzleri (1.02%), 1 as C. fetus and 1 as C. lari with (0.51% each). Twenty-two (11.2 %) of the isolates were undefined species (Figure 1). At least, 175 (88.8%) were culture positive and 22 (11.2%) were culture negative.
Age and sex distribution of Campylobacter infections
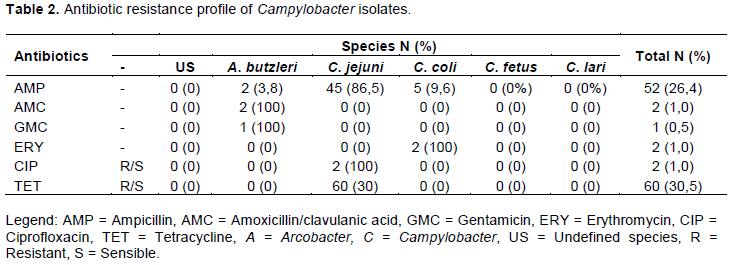
The isolation rate of Campylobacter was highest in the 0 - 9 (22%) age group, followed by 10-19 (15%), 20 - 29 (12%), 30 - 39 and 40-49 (10% each). Age group above 50 recorded the least isolation rate (≤10%) (Figure 2). The proportion of male and female patients was 59.4% (CI 95% = 52.2-66.3) and 40.6% (CI 95% = 33.7-42.8) respectively. Table 1 shows a breakdown of the different species isolated according to the sex of the patient.
The identification of Campylobacter species and related organisms at the species level has always been difficult using phenotypic methods because of their low metabolic activity, whereas molecular methods are more reliable but time-consuming (Bessède et al., 2011). The development of MALDI-TOF MS, a rapid and cost effective analytical method, has profoundly improved the bacterial identification process (Mandrell et al., 2005; Kolinska et al., 2008; Alispahic et al., 2010). In overall, we isolated about 88.8% of a combined species of Campylobacter. This is consistent with reported percentages of Campylobacter isolated in Nigeria (62.7%; Ewnetu and Mihret, 2010) and in Ethiopia (72.7%; Gwimi et al., 2015). The relative high percentage of Campylobacter's identification may be attributed to the use of mass spectrometry by the CNR. Several studies, (e.g. 20%, Coker et al., 2002; 5.8 - 9%, Girgis et al., 2014; 17.3%, Karikari et al., 2017), have also reported much lower identification rates of Campylobacter than those recorded in this study. The incidence of Campylobacter-associated food poisoning has gradually increased, and this organism is now considered as the leading cause of bacterial gastroenteritis worldwide (Bessède et al., 2011). A study has shown that campylobacteriosis incidences have been globally in rise in the past decade. Thus, the numbers of campylobacteriosis incidences have increased in North America, Europe and Australia (Kaakoush et al., 2015).
Incidences and number of cases may substantially vary among countries or regions or within a given country (Kubota et al., 2011; Sadkowska-Todys and Kucharczyk 2012). These variations are attributable to several factors such as sensitivity of detection methodologies, geographic locations, target population, differences in the standard and stringency of biocontrol protocols, surveillance bias, food practices as well as the availability of natural reservoirs of Campylobacter species (Kaakoush et al., 2015).
In contrast, the identified species were C. jejuni (72.59%), C. coli (14.21%), Arcobacter butzleri (1.02%), C. fetus and C. lari (0.51% each). These results are similar to those previously reported in France: C. jejuni (78%), C. coli (14%) and C. fetus (4%) (Bessède et al., 2011). Because of the low identification rates of the analytical methods, incidences of C. jejumi and C. coli infections are likely to be underestimated (Wagenaar et al., 2013). In most industrialized countries, Campylobacter organisms are, along with Salmonella, the most common cause of foodborne bacterial gastroenteritis (Allos and Blaser, 1995; Frost, 2001). Furthermore, consumption of undercooked (raw, rare, or “pink”) chicken and beef was the most important food-specific risk factor for Campylobacter infection in France (Gallay et al., 2008; Berthenet et al., 2019). In the present study, high rates (22%) of Campylobacter were identified in children under 10 years old. This result was consistent with those reported in 2017 by French National Reference Centre for Campylobacter and by developing countries (Coker et al., 2002). While infection with C. jejuni or C. coli can occur in patients of all ages, a recent study in Denmark showed that infection is more prevalent in toddlers (1 to 4 years) and young adults (15 to 24 years) than in other age groups (Nielsen et al., 2013).
Our study also showed that Campylobacter infections were more prevalent in male (59.4%) than in female (40.6%) patients. This is corroborated by previous studies, which reported high campylobacter prevalent in male patients compared to female patients (Friedman et al., 2000; Fitzgerald et al., 2011). However, some studies found that females have higher risk of getting infected by Campylobacter than males (Gillespie et al., 2006; Karikari et al., 2017).The isolated strains in our study showed considerable resistance to ampicillin (26.4%), to tetracycline (30.5%) whereas the resistances to ciprofloxacin, erythromycin and gentamicin were relatively low (0.5-1%). These results are in agreement with 30.7% resistance to tetracycline, 26.9% to ciprofloxacin, 1.7% to erythromycin and 0.9% to gentamicin previously reported in France (Gallay et al., 2008). A similar resistance to tetracycline (22%) was documented in Ethiopia (Ewnetu and Mihret, 2010). Furthermore, our results are lower than 48.0% resistant to ampicillin reported by Gallay et al. (2008). High resistance rates to tetracycline have been described in Ghana (92.3 - 100%, Karikari et al., 2017), in Spain (72%; Prats et al., 2000) in human isolates. At the global scale, the tetracyclines are a heavily used class of antibiotics both in human and in veterinary medicine (Iovine, 2013). The discovery in 1950 that the addition of antibiotics to animal feed at sub therapeutic levels could lead to increased growth rates of these animals. This results in research into methods to improve or stabilize meat supplies to the consumer (Kaakoush et al., 2015). For instance, by the turn of the 20th century, the majority of antibiotic used in the United States was for agricultural purposes. This approach has led to a dramatic increase in antibiotic resistance in several human pathogens that originate from domesticated animals, including Campylobacter species (Barton, 2014). Since the beginning of the 1990s, the resistance of Campylobacter organisms to antibiotics has increased (Gallay et al., 2008). Thus, a strong relationship has been observed between the amounts of fluoroquinolone in animal feed and the presence of pathogen strains of Campylobacter in humans (Kaakoush et al., 2015). Although the Campylobacter infection is self-limiting, the extra-intestinal infection or septicaemia may occur, and thereby requiring treatment using appropriate antibiotics.
The identification by MALDI-TOF mass spectrometry is particularly efficient for the identification of campylobacters (should be campylobacters, low cas for c) and makes it possible to identify genera and species difficult to access by traditional identification tests (phenotypic and molecular methods): C. lari, C. upsaliensis, C. "anaerobic" "(C. ureolyticus in particular), Arcobacters and enterohepatic Helicobacters, some of whose pathogenesis is close to Campylobacter (especially Helicobacter pullorum, Helicobacter cinaedi). The systematic identification by mass spectrometry, a quick and inexpensive method, of several colonies (including of atypical aspect) pushing on the selective media increases the rate of detection. Therefore, it seems that the results using mass spectrometry correlates with the profiles of the control strains using mass spectrometry but further confirmation is needed.
The authors have not declared any conflict of interests.
REFERENCES
|
Abdi-Hachesoo B, Khoshbakht R, Sharifiyazdi H, Tabatabaei M, Hosseinzadeh S, Asasi K (2014). Tetracycline Resistance Genes in Campylobacter jejuni and C. coli Isolated From Poultry Carcasses. Jundishapur Journal of Microbiology 7(9):e12129.
Crossref
|
|
|
|
Alispahic M, Hummel K, Jandreski-Cvetkovic D, Nobauer K, Razzazi- Fazeli E, Hess M, Hess C (2010). Species-specific identification and differentiation of Arcobacter, Helicobacter and Campylobacter by fullspectral matrix-associated laser desorption/ionization time of flight mass spectrometry analysis. Journal of Medical Microbiology 59:295-301.
Crossref
|
|
|
|
|
Allos BM, Blaser MJ (1995). Campylobacter jejuni and the expanding spectrum of related infections. Clinical Infectious Diseases 20:1092-1099.
Crossref
|
|
|
|
|
Barton MD (2014). Impact of antibiotic use in the swine industry. Current Opinion in Microbiology 19:9-15.
Crossref
|
|
|
|
|
Berthenet E, Thépault A, Chemaly M, Rivoal K, Ducournau A, Buissonnière A, Bénéjat L, Bessède E, Mégraud F, Sheppard SK, Lehours P (2019). Source attribution of Campylobacter jejuni shows variable importance of chicken and ruminants reservoirs in noninvasive and invasive French clinical isolates. Scientific Reports 9(1):8098.
Crossref
|
|
|
|
|
Bessède E, Solecki O, Sifré E, Labadi L, Megraud F (2011). Identification of Campylobacter species and related organisms by matrix-assisted laser desorption ionization-time of flight (MALDI-TOF) mass spectrometry. Clinical Microbiology and Infection 17:1735-1739.
Crossref
|
|
|
|
|
Centers for Disease Control and Prevention (CDC) (2013). Incidence and trends of infection with pathogens transmitted commonly through food - Foodborne diseases active surveillance network, 10 U.S. sites, 1996-2012. Morbidity and Mortality Weekly Report, 62: 283-287.
|
|
|
|
|
Centre National de Référence des Campylobacters et des Hélicobacters (CNRCH) (2018). Rapport annuel d'activité -année d'exercice 2017.
|
|
|
|
|
Coker AO, Isokpehi RD, Thomas BN, Amisu KO, Obi CL (2002). Human Campylobacteriosis in Developing Countries. Emerging Infectious Disease 8:237-244.
Crossref
|
|
|
|
|
EFSA (2010). The community Summary Report on Trends and Sources of Zoonoses, Zoonotic Agents and Food-borne Outbreaks in the European Union in 2008. EFSA Journal 8(1):1496.
Crossref
|
|
|
|
|
European Committee on Antimicrobial Susceptibility Testing (EUCAST), (2018). View
|
|
|
|
|
Ewnetu D, Mihret A (2010). Prevalence and Antimicrobial Resistance of Campylobacter Isolates from Humans and Chickens in Bahir Dar, Ethiopia. Foodborne Pathogens and Disease 7:667-670.
Crossref
|
|
|
|
|
Fitzgerald C, Patrick M, Jerris R, Watson R, Tobin-D'Angelo M, Gonzalez A, Polage C, Wymore K, Gillim-Ross L, Sadlowski J, Monahan J, Hurd S, Dahlberg S, De Martino M, Pentella M, Razeq J, Leonard C, Jung C, Juni B, Robinson T, Gittelman R, Garrigan C, Nachamkin I, Campylobacter Diagnostics Working Group (2011). Multicenter Study to Evaluate Diagnostic Methods for Detection and Isolation of Campylobacter from Stool. Annual Meeting of the American Society for Microbiology, New Orleans, 20 September 2011.
|
|
|
|
|
Friedman CR, Neimann J, Wegener HC, Tauxe RV (2000). Epidemiology of Campylobacter jejuni infections in the United States and other industrialized nations, p. 121 138. In I. Nachamkin and M. J. Blaser (ed.), Campylobacter, 2nd ed. ASM Press, Washington, DC.
|
|
|
|
|
Frost JA (2001). Current epidemiological issues in human campylobacteriosis. Symposium Series Society for Applied Microbiology 90:85-95.
Crossref
|
|
|
|
|
Gallay A, Prouzet-Mauléon V, Kempf I, Lehours P, Labadi L, Camou C, Denis M, de Valk H, Desenclos J-C, Mégraud F (2007). Campylobacter antimicrobial drug resistance among humans, broiler chickens, and pigs, France. Emerging Infectious Diseases13(2):259-266.
Crossref
|
|
|
|
|
Gallay A, Bousquet V, Siret V, Prouzet-Mauléon V, de Valk H, Vaillant V, Simon F, Le Strat Y, Mégraud F, Desenclos J-C (2008). Risk Factors for Acquiring Sporadic Campylobacter Infection in France: Results from a National Case-Control Study. The Journal of Infectious Diseases 197:1477-1484.
Crossref
|
|
|
|
|
Gillespie IA, O'Brien SJ, Frost JA, Tam C, Tompkins D, Neal KR, Syed Q, Farthing MJG, the Campylobacter Sentinel Surveillance Scheme Collaborators (2006). Investigating Vomiting and/or Bloody Diarrhea in Campylobacter jejuni Infection. Journal of Medical Microbiology 55 Article ID: 741746.
Crossref
|
|
|
|
|
Girgis SA, Rashad SS, Othman HB, Bassim HH, Kassem NN, El-Sayed FM (2014). Multiplex PCR for identification and differentiation of campylobacter species and their antimicrobial susceptibility pattern in Egyptian patients. International Journal of Current Microbiology and Applied Sciences 3:861-875.
|
|
|
|
|
Gwimi PB, Faleke O, Salihu MD, Magaji AA, Abubakar MB, Nwankwo IO, Ibitoye EB (2015). Prevalence of Campylobacter Species in faecal samples of pigs and humans from Zuru Kebbi State, Nigeria. International Journal of One Health 1: 1-5.
Crossref
|
|
|
|
|
Humphrey T, O'Brien S, Madsen M (2007). Campylobacters as zoonotic pathogens: a food production perspective. International Journal of Food Microbiology 117(3):237-257.
Crossref
|
|
|
|
|
Iovine NM (2013). Resistance Mechanisms in Campylobacter jejuni. Virulence 4:230-240.
Crossref
|
|
|
|
|
Kaakoush NO, Castaño-Rodríguez N, Mitchell HM, Man SM (2015). Global epidemiology of Campylobacter infection. Clinical Microbiology Reviews 28:687-720.
Crossref
|
|
|
|
|
Karikari AB, Obiri-Danso K, Frimpong EH, Krogfelt KA (2017). Antibiotic Resistance in Campylobacter Isolated from Patients with Gastroenteritis in a Teaching Hospital in Ghana. Open Journal of Medical Microbiology 7:1-11
Crossref
|
|
|
|
|
Kolinska R, Drevinek M, Jakubu V, Zemlickova H (2008). Species identification of Campylobacter jejuni ssp. jejuni and C. coli by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry and PCR. Folia Microbiologica 53:403-409.
Crossref
|
|
|
|
|
Kubota K, Kasuga F, Iwasaki E, Inagaki S, Sakurai Y, Komatsu M, Toyofuku H, Angulo FJ, Scallan E, Morikawa K (2011). Estimating the burden of acute gastroenteritis and foodborne illness caused by Campylobacter, Salmonella, and Vibrio parahaemolyticus by using population based telephone survey data, Miyagi Prefecture, Japan, 2005 to 2006. Journal of Food Protection 74:1592-1598.
Crossref
|
|
|
|
|
Lucey B, Cryan B, O'Halloran F, Wall PG, Buckley T, Fanning S (2002). Trends in antimicrobial susceptibility among isolates of Campylobacter species in Ireland and the emergence of resistance to ciprofloxacin. Veterinary Record 151:317-320.
Crossref
|
|
|
|
|
Mandrell RE, Harden LA, Bates A, Miller WG, Haddon WF, Fagerquist CK (2005). Speciation of Campylobacter coli, C. jejuni, C. helveticus, C. lari, C. sputorum, and C. upsaliensis by matrix-assisted laser desorption ionization- time of flight mass spectrometry. Applied and Environmental Microbiology 71:6292-6307.
Crossref
|
|
|
|
|
Nachamkin I, Blaser MJ (2000). Campylobacter. 2nd ed. Washington: ASM Press.
|
|
|
|
|
Nachamkin I, Ung H, Li M (2002). Increasing fluoroquinolone resistance in Campylobacter jejuni, Pennsylvania, USA, 1982-2001. Emerging Infectious Diseases 8:1501-3503.
Crossref
|
|
|
|
|
Nielsen HL, Ejlertsen T, Engberg J, Nielsen H (2013). High incidence of Campylobacter concisus in gastroenteritis in North Jutland, Denmark: a population-based study. Clinical Microbiology and Infection 19:445-450.
Crossref
|
|
|
|
|
Obeng AS, Rickard H, Sexton M, Pang Y, Peng H, Barton M (2012). Antimicrobial susceptibilities and resistance genes in Campylobacter strains isolated from poultry and pigs in Australia. Journal of Applied Microbiology 113:294-307.
Crossref
|
|
|
|
|
Prats G, Mirelis B, Llovet T, Muñoz C, Miro AE, Navarro F (2000). Antibiotic resistance trends in enteropathogenic bacteria isolated in 1985-87 and 1995-98 in Barcelona. Antimicrobial Agents and Chemotherapy 44:1140-1145.
Crossref
|
|
|
|
|
Reddy S, Zishiri OT (2017). Detection and prevalence of antimicrobial resistance genes in Campylobacter spp. isolated from chickens and humans. Onderstepoort Journal of Veterinary Research 84(1):a1411.
Crossref
|
|
|
|
|
Wardak S, Duda U, Szych J (2007). Epidemiological analysis of campylobacteriosis reported by sanitary epidemiological station in Bielsko-Biala, Silesia, in Poland. Przegla̧d Epidemiologiczny 61(2):417-424.
|
|