Full Length Research Paper

ABSTRACT
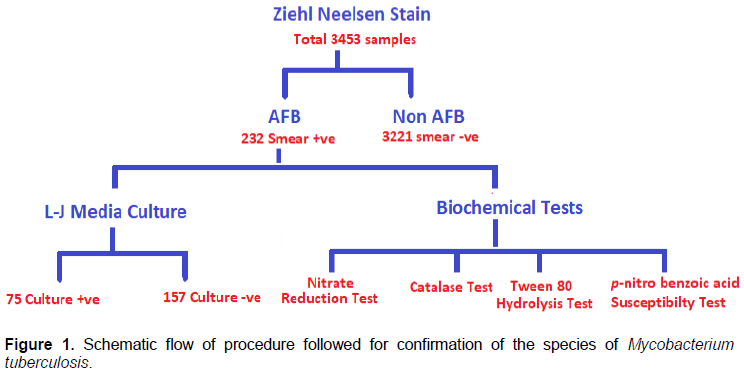
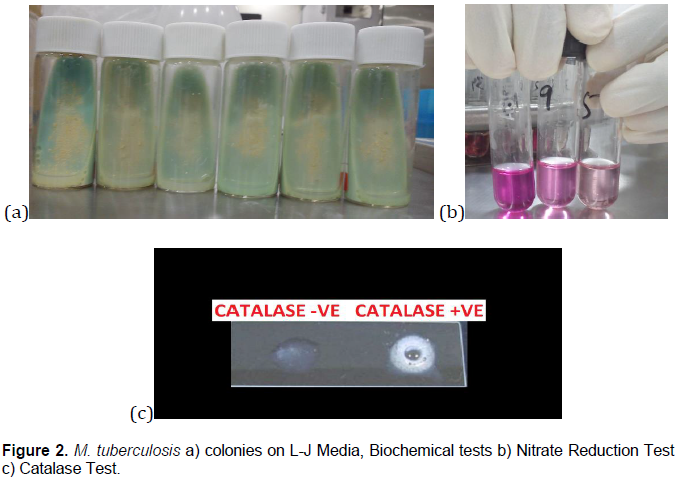
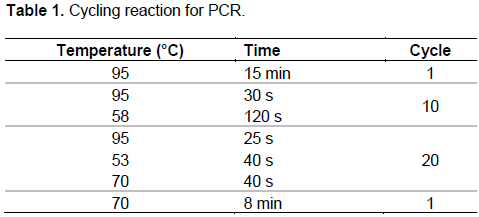
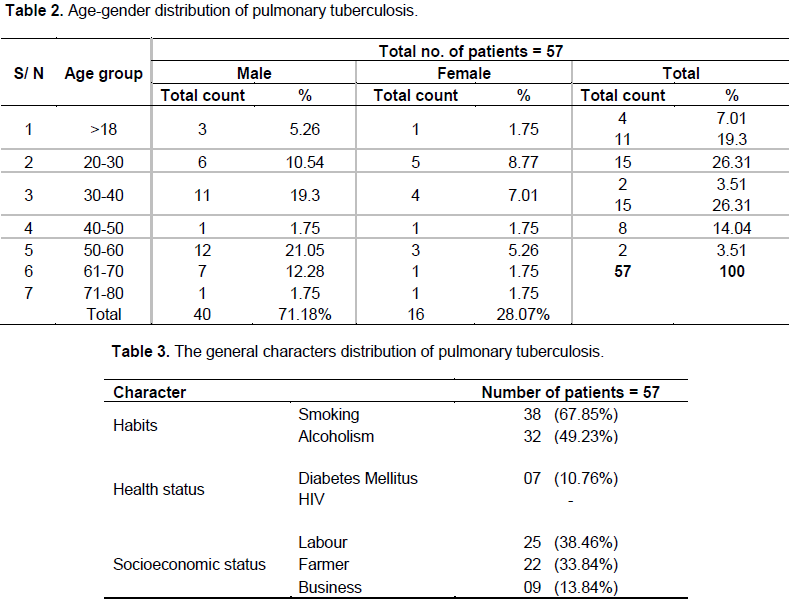
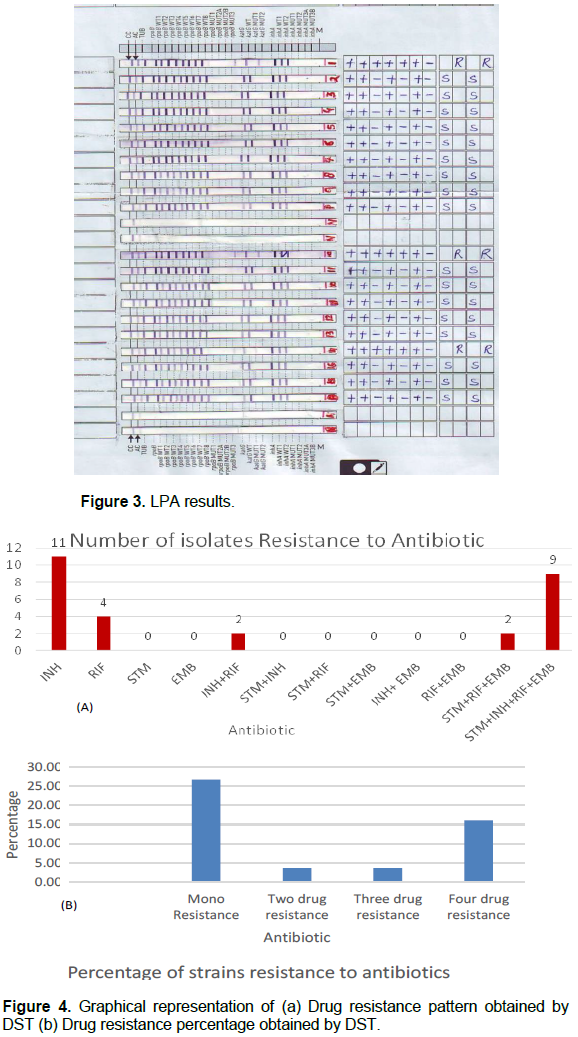
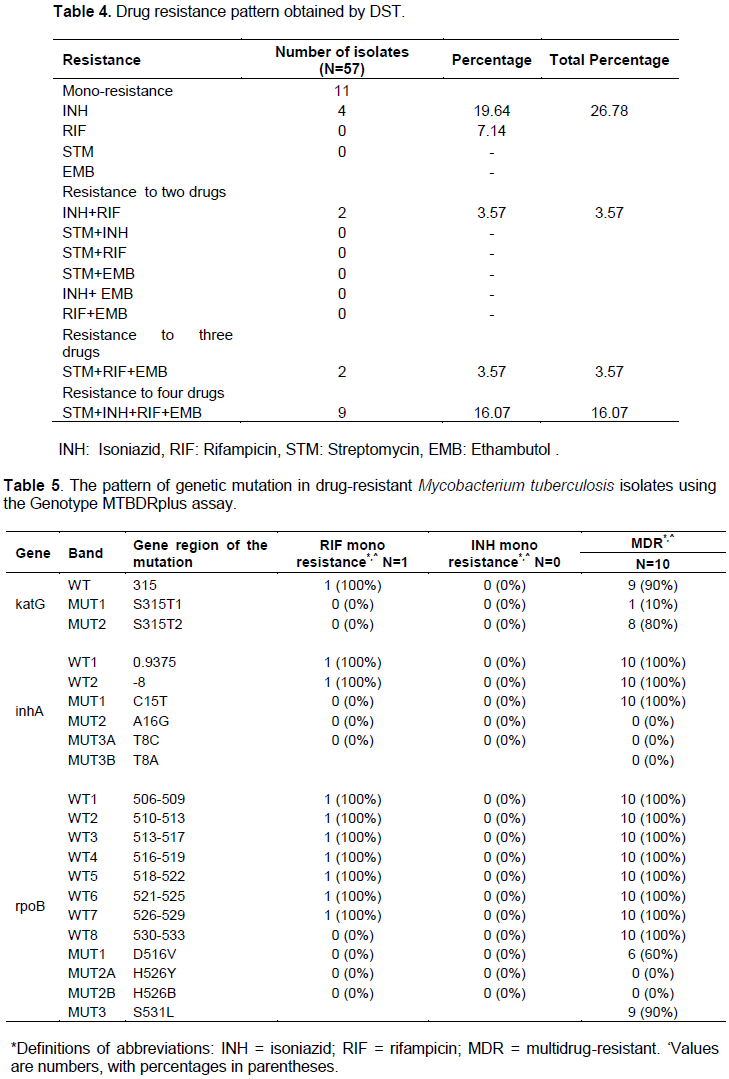
The control of tuberculosis (TB) has become a global health challenge due to the emergence of multidrug-resistant tuberculosis (MDR-TB) in Mycobacterium tuberculosis (MTB). This highlights the need for faster and more accurate detection of tuberculosis cases. The study aims to detect MDR-TB strains of pulmonary tuberculosis using resistance ratio method and to compare the diagnostic value of drug susceptibility testing (DST) with line probe assay (LPA) using Genotype MTBDRplus. All the sputum samples were tested for Acid Fast Bacilli (AFB) by Ziehl-Neelsen’s staining method and were cultured on Lowenstein-Jensen (L-J) media. The identification and confirmation of M. tuberculosis were done using various biochemical tests. DST was carried against the first line of anti-TB drugs. MTB positive samples were subjected to LPA. A total of 57 samples were subjected to DST and LPA for the detection of drug resistance of MTB to RIF and INH after conventional detection methods were applied to all the samples. Among these 57 MTB samples, 11 (19.29%) were resistant to INH, 4 (7.14%) were resistant to RIF; eleven (19.29%) isolates were identified as MDR-TB. LPA revealed 54 MTB positive among 57 MTB culture-positive samples and 3 showed invalid results. In LPA, MDR-TB was found in10 samples (17.54%) in which one was RIF-resistant. The study concludes risk factors that resulted in the development of TB are biomedical, socio-cultural, and behavioral interactions. LPA can be used as a rapid diagnostic technique for the detection of MDR-TB.
Key words: Tuberculosis (TB), multidrug resistance (MDR-TB), drug susceptibility testing (DST), line probe assay (LPA).
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
CONFLICT OF INTERESTS
ACKNOWLEDGMENTS
REFERENCES
|
Acharya S, Ghimire P, Khadka D, Nepali S (2010). Comparison of Proportion and Resistance Ratio Methods for Drug Susceptibility Testing of Mycobacterium tuberculosis isolated from Patients Attending National Tuberculosis Centre, Nepal. SAARC Journal of Tuberculosis, Lung Diseases and HIV/AIDS 5(1):13-20. |
|
|
Ahmed S, Shukla I, Fatima N, Varshney SK, Shameem M (2017). Evaluation of genotype MTBDRplus line probe assay in detection of rifampicin and isoniazid resistance in comparison to solid culture drug susceptibility testing in a tertiary care centre of western Uttar Pradesh. Indian Journal of Medical Microbiology 35:568-574. |
|
|
Balaji V, Daley P, Anand AA, Sudarsanam T, Michael JS, Sahni DR, Chordia P, George IA, Thomas K, Ganesh A, John KR (2010). Risk Factors for MDR and XDR-TB in a Tertiary Referral Hospital in India. PLoS ONE 53:e9527. |
|
|
Barnard M, Parsons L, Miotto P, Cirillo D, Feldmann K, Gutierrez C, Somoskovi A (2012). Molecular detection of drug resistant tuberculosis by line probe assay-Laboratory manual for resource-limited settings. Geneva: FIND. |
|
|
Bhawan N (2009). Training Manual for Mycobacterium tuberculosis Culture and Drug susceptibility testing. National Tuberculosis Institute, Bangalore. |
|
|
Cavusoglu C, Hilmioglu S, Guneri S, Bilgic A (2002).Characterization of rpoB mutations in rifampin-resistant clinical isolates of Mycobacterium tuberculosis from Turkey by DNA sequencing and line probe assay. Journal of Clinical Microbiology 40(12):4435-4438. |
|
|
Central TB Division (2005). Directorate General of Health Services, Ministry of Health & family Welfare, Government of India. |
|
|
Chakravorty S, Tyagi J (2005). Novel Multipurpose Methodology for Detection of Mycobacteria in Pulmonary and Extrapulmonary Specimens by Smear Microscopy, Culture, and PCR. Journal of Clinical Microbiology 43:2697-2702. |
|
|
Chauhan LS, Arora VK (2004). Central TB Division, Directorate General of Health Services, Ministry of Health and Family Welfare; Indian Academy of Paediatrics, Management of Paediatric Tuberculosis under the Revised National Tuberculosis Control Program (RNTCP). Indian Paediatrics 41:901-905. |
|
|
Chauhan MM, Mahadev B, Balasangameshwara, VH (1998). Manual on isolation, identification and sensitivity testing of Mycobacterium tuberculosis. National Tuberculosis Institute, Bangalore, India. |
|
|
de Viedma DG, Infantes MDSD, Lasala F, Chaves F, AlcaláL, Bouza E (2002). New real-time PCR able to detect in a single tube multiple rifampin resistance mutations and high-level isoniazid resistance mutations in Mycobacterium tuberculosis. Journal of Clinical Microbiology 40(3): 988-995. |
|
|
Deodhar LL, Miskeen P, Chomal S (1999). Drug resistance in tuberculosis. Bombay Hospital Journal 41:253. |
|
|
Desikan P, Panwalkar N, Mirza SB, Chaturvedi A, Ansari K, Varathe R, Chourey M, Kumar P, Pandey M (2017). Line probe assay for detection of Mycobacterium tuberculosis complex: An experience from Central India. The Indian Journal of Medical Research 145(1):70. |
|
|
Fleming MF, Krupitsky E, Tsoy M, Zvartau E, Brazhenko N, Jakubowiak, W, McCaul ME (2006). Alcohol and drug use disorders, HIV status and drug resistance in a sample of Russian TB patients. International Journal of Tuberculosis Lung Diseases 10:565-570. |
|
|
Gaude GS, Hattiholli J, Kumar P (2014). Risk factors and drug-resistance patterns among pulmonary tuberculosis patients in the northern Karnataka region, India. Nigerian Medical Journal 55:327-333. |
|
|
HainLifesciences GmbH Germany (2012). GenoType MTBDR Plus VER 2.0. Instructions for Use IFU-304A-02 |
|
|
Gupta S, Shenoy VP, Mukhopadhyay C, Bairy I, Muralidharan S (2011). Role of risk factors and socioeconomic status in pulmonary tuberculosis: A search for the root cause in patients in a tertiary care hospital, South India. Tropical Medicine and International Health 16:74-78. |
|
|
Haldane JBS (1945). On a method of estimating frequencies. Biometrika 33(3):222-225. |
|
|
Havumaki J, Hillemann D, Ismail N, Omar SV, Georghiou SB, Schumacher SG, Boehme C, Denkinger CM (2017). Comparative accuracy of the REBA MTB MDR and HainMTBDRplus line probe assays for the detection of multidrug-resistant tuberculosis: A multicenter, non-inferiority study. PloS ONE 12(3):0173804. |
|
|
Hillemann D, Weizenegger M, KubicaT, Richter E, Niemann S (2005). Use of the genotype MTBDR assay for rapid detection of rifampin and isoniazid resistance in Mycobacterium tuberculosis complex isolates. Journal of Clinical Microbiology 43(8):3699-3703. |
|
|
Iqbal S, Iqbal, R, Khan MM, Hussain I, Akhtar A, Shabbir I (2003). Comparison of Two Conventional Techniques used for the Diagnosis of Tuberculosis. International Journal of Agriculture and Biology 5:545-547. |
|
|
Kent PT, Kubica GP (1985). Public health Mycobacteriology: A guide for the level III laboratory. US Department of Health and Human Services, Public health service, CDC, Georgia. |
|
|
Khanna A, Raj VS, Tarai B, Sood R, Pareek PK, Upadhyay DJ, Sharma P, Rattan A, Saini, KS, Singh H (2010). Emergence and molecular characterization of extensively drug-resistant Mycobacterium tuberculosis clinical isolates from the Delhi Region in India Antimicrobial agents and chemotherapy 54(11):4789-4793. |
|
|
Manual on Isolation, Identification and Sensitivity (1998). Testing of Mycobacterium tuberculosisntiindia.kar.nic.in/cdc district level. |
|
|
Meaza A, Kebede A, Yaregal Z, Dagne Z, Moga S, Yenew B, Diriba G, Molalign H, Tadesse M, Adisse D, Getahun M (2017). Evaluation of genotype MTBDR plus VER 2.0 line probe assay for the detection of MDR-TB in smear-positive and negative sputum samples. BMC Infectious Diseases 17(1):280. |
|
|
Miotto P, Piana F, Penati V, Canducci F, Migliori GB, Cirillo DM (2006). Use of genotype MTBDR assay for molecular detection of rifampin and isoniazid resistance in Mycobacterium tuberculosis clinical strains isolated in Italy. Journal of Clinical Microbiology 44(7):2485-2491. |
|
|
Morcillo N, Zumarraga M, Alito A, Dolmann A, Schouls L, Cataldi A, Kremer K, Van Soolingen D (2002). A low-cost, home-made, reverse- line blot hybridization assay for rapid detection of rifampicin resistance in Mycobacterium tuberculosis. International Journal of Tuberculosis and Lung Disease 6:959-965. |
|
|
Nathavitharana RR, Cudahy PGT, Schumacher SG, Steingart KR, Pai M, Denkinger CM (2017). Accuracy of line probe assays for the diagnosis of pulmonary and multidrug-resistant tuberculosis: A systematic review and meta-analysis. European Respiratory Journal 18:49-51. |
|
|
Omer ZB, Mekonnen Y, Worku A, Zewde A, Medhin G, Mohammed T, Pieper R, Ameni G (2016). Evaluation of the GenoTypeMTBDRplus assay for detection of rifampicin-and isoniazid-resistant Mycobacterium tuberculosis isolates in central Ethiopia. International Journal of Mycobacteriology 5(4):475-481. |
|
|
Protocol for Processing Specimens for Culture (1998). |
|
|
Revised National TB Control Programme (2014). Training Manual for Mycobacterium tuberculosis Culture & Drug susceptibility testing. |
|
|
Revised National Tuberculosis Control Programme Laboratory Network (2005) Guidelines for quality assurance of smear microscopy for diagnosing tuberculosis. TBC India. |
|
|
Saribas Z, Kocagoz T, Alp A, Gunalp A (2003). Rapid Detection of Rifampin Resistance in Mycobacterium tuberculosis Isolates by Heteroduplex Analysis and Determination of Rifamycin Cross-Resistance in Rifampin-Resistant Isolates. Journal of Clinical Microbiology 41(2):816-818. |
|
|
Siddiqi N, Shamim M, Hussain S, Choudhary RK, Ahmed N, Prachee, Banerjee S, Savithri GR, Alam M, Pathak N, Amin A, Hanief M, Katoch VM, Sharma SK, Hasnain SE (2002). Molecular Characterization of Multidrug-Resistant Isolates of Mycobacterium tuberculosis from patients in North India. Antimicrobial Agents and Chemotherapy 46 (2):443-450. |
|
|
Sun Z, Chao Y, Zhang X, Zhang J, Li Y, Qiu Y, Liu Y, Nie L, Guo A, Li C (2008). Characterization of Extensively Drug-Resistant Mycobacterium tuberculosis Clinical Isolates in China. Journal of Clinical Microbiology 46(12):4075-4077. |
|
|
Taniguchi H, Aramaki H, Nikaido Y, Mizuguchi Y, Nakamura M, Koga T, Yoshida S (1996). Rifampicin resistance and mutations of the rpoB gene in Mycobacterium tuberculosis.FEMS Microbiology Letters 144:103-108. |
|
|
TB Statistics for India (National and State Statistics) |
|
|
Telenti A, Honoré N, Bernasconi C, March J, Ortega A, Heym B, Takiff HE, Cole ST (1997). Genotypic assessment of isoniazid and rifampin resistance in Mycobacterium tuberculosis: A blind study at reference laboratory level. Journal of Clinical Microbiology 35(3):719-723. |
|
|
Telenti A, Imboden P, Marchesi F, Lowrie D, Cole S, Colston MJ, Matter L, Schopfer K, Bodmer T (1993). Detection of rifampicin-resistance mutations in Mycobacterium tuberculosis. Lancet 341:647-650. |
|
|
Tripathy S, Kumar R, Singh SD (2015). Prevalence of Multidrug Resistant Pulmonary Tuberculosis in North Bihar. Journal of Clinical and Diagnostic Research 9:09-12. |
|
|
World Health Organization (2008). Molecular line probe assays for rapid screening of patients at risk of multi-drug resistant tuberculosis (MDR-TB). Policy statement WHO, Geneva, Switzerland TBC. |
|
|
World Health Organization (2009). Guidelines for surveillance of drug resistance in tuberculosis (No. WHO/HTM/TB/2009.422). Geneva: World Health Organization. |
|
|
World Health Organization (2016). Global Tuberculosis Report, WHO, Geneva, Switzerland. |
|
|
Yadav RN, Singh BK, Sharma SK, Sharma R, Soneja M, Sreenivas V, Myneedu VP, Hanif M, Kumar A, Sachdeva KS, Paramasivan CN, Vollepore B, Thakur R, Raizada N, Arora SK, Sinha S (2013). Comparative Evaluation of GenoTypeMTBDRplus Line Probe Assay with Solid Culture Method in Early Diagnosis of Multidrug-Resistant Tuberculosis (MDR-TB) at a Tertiary Care Centre in India. PLoS ONE 8(9):72036. |
|
|
Yue J, Shi W, Xie J, Li Y, Zeng E, Wang H (2003). Mutations in the rpoB Gene of Multidrug- Resistant Mycobacterium tuberculosis isolates from China. Journal of Clinical Microbiology 41(5):2209-2212. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


