ABSTRACT
The aim of this study was to use molecular methods to determine the profile of resistance to rifampicin (RMP or RIF) and isoniazid (INH) in mycobacteria from tuberculosis patients in Senegal. Sputum samples (48) received by the mycobacterial laboratory of the National Antituberculosis Program (NATP) in Senegal between 2012 and 2014 were studied. Most of these samples came from patients in treatment failure or relapse (58.33%). They were tested with the Xpert MTB/RIF or line-probe assays (LPAs) or both. 17 (35.41%) isolates resistant to INH, 16 (33.33%) resistant to RMP, and 16 that were multidrug-resistant (MDR) (33.33%) were identified. Two isolates (4.16%) were susceptible to INH, but resistant to RMP (INH-S/RIF-R). The molecular tests facilitated the rapid detection of MDR isolates. However, INH resistance should be assessed in all cases in which RIF resistance is detected, given the demonstrated existence of INH-S/RIF-R strains.
Key words: Tuberculosis, Xpert MTB/RIF, line-probe assays (LPA), resistance, Senegal.
With an annual incidence exceeding 300 cases per 100,000 inhabitants in some countries, particularly in sub-Saharan Africa, tuberculosis remains a major public health problem (Mbatchou et al., 2008). This disease is treated with a combination of four antituberculosis drugs: rifampicin (RMP), isoniazid (INH), ethambutol (EMB), and streptomycin (SM). Multi-resistance to antituberculous drugs (multidrug resistance or MDR) is defined as resistance to both RMP and INH (Kurbatova et al., 2012). The objective of this study was to use molecular methods to determine the profile of resistance to RMP and INH in the mycobacteria present in tuberculosis patients in Senegal.
Sputum samples received by the mycobacterial laboratory of the National Antituberculosis Program (NATP), thenational reference laboratory in Senegal, between 2012 and 2014 were studied. Clinical data (full name, age, sex, clinical diagnosis, history of antituberculous treatment, and referring structure) were obtained from the analysis reports accompanying the samples.
The procedure for analyzing these samples in the laboratory began with Ziehl-Neelsen staining and microscopy, to check that the sample contained acid-fast bacteria (AFB). All the samples included in this study yielded positive microscopy results. Two molecular tests recommended by the WHO (WHO Policy Statement (WHO, 2015; Rapid Implementation of Xpert MTB/RIF (WHO), 2011) and able to identify mycobacteria of the tuberculosis complex and the most frequent mutations conferring resistance to RMP and INH were then used: the line-probe assay (LPA) (FIND, 2015) and Xpert MTB/RIF (Rapid implementation of Xpert MTB/RIF (WHO), 2011).
The Xpert MTB/RIF test involves using polymerase chain reaction (PCR) to amplify directly the rpoB gene of tuberculosis complex mycobacteria present in the sample. It can also be used to detect the mutations associated with RMP resistance. This test is supplied in the form of ready-to-use cartridges. The sample (2 ml) is decontaminated, neutralized, and diluted in a specific solution and then added to the cartridge. The cartridge is then loaded into the machine, which carries out all the steps of the PCR. The result is obtained after about 2 h.
LPA is a molecular technique that can be used directly on samples to detect mutations of the katG and inhA genes (conferring high- or low-level resistance to INH) and rpoB gene (resistance to RMP). The result is obtained after about 5 h.
Depending on the availability of the reagents, the samples were tested with the Xpert MTB/RIF alone, the LPA alone, or with both. In cases in which both tests were used, the LPA was used principally to check the susceptibility to INH of the isolates resistant to RMP identified by Xpert MTB/RIF. The data were analyzed with Epi-Info version 7.
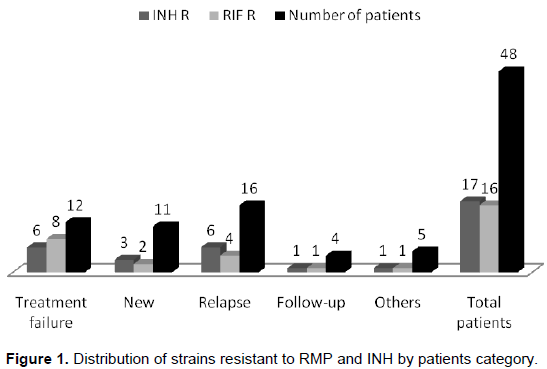
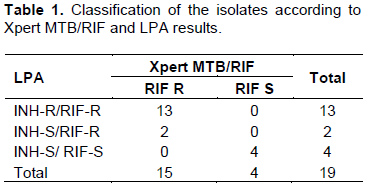
This study included a total of 48 sputum samples during the period studied. These samples came from patients aged between 9 and 89 years old (mean 36.06); the sex ratio (M/F) was 2.35. Most of these samples came from patients with treatment failure (25%) or relapses (33.33%) (Figure 1). Thirteen (13) of these samples were tested only with the Xpert MTB/RIF, 16 were tested only with the LPA, and 19 were tested with both (Table 1). Of the samples tested with the Xpert MTB/RIF, one was found to be resistant to RMP, 10 were susceptible to RMP and the other two negative. The LPA identified 3 isolates as INH-R/RIF-R, 3 as INH-R/RIF-S, 9 as INH-S/RIF-S and 1 sample to be negative. By combining Xpert MTB/RIF and LPA results, two isolates (4.16%) susceptible to INH and resistant to RMP (INH-S/RIF-R) were identified (Table 1).
In total, 16 MDR isolates were detected (33.33%). The rates of resistance were high among patients with relapses (37.5% resistant to INH and 25% resistant to RMP) or treatment failure (50% resistant to INH and 66.66% resistant to RMP) (Figure 1).
The emergence of resistance to antituberculous drugs is a major problem in most African countries (Sangaré et al., 2010). Two molecular techniques recommended by the WHO and suitable for use directly on samples and in laboratories in the field were used, because they do not require the extensive biosafety precautions needed for culture of the tuberculosis bacillus. In Senegal, the national resistance screening algorithm in use since 2014 involves the use of the Xpert MTB/RIF as the first-line diagnostic tool. Consequently, the NATP has equipped five regions (Kaolack, Saint Louis, Kolda, Fatick, and Diourbel) with Xpert MTB/RIF machines, to facilitate the detection of MDR strains (PNT, 2013). Most of our samples came from young male patients, as reported in other studies (Diop et al., 2014). Most presented treatment failure or relapse (58.33%), potentially accounted for the high frequency of MDR strain detection in this study (33.33%). Indeed, this frequency is higher than that reported for Senegal in 2010 (1% strains in new patients were MDR and 11% in treated patients) (Chevalier et al., 2010). However, it is lower than frequencies reported for the Central African Republic (40%) (Minime-Lingoupou et al., 2010), Burkina Faso (50.5%) (Sangaré et al., 2010) and Ivory Coast (79%) (Kouassi et al., 2004).
Some samples were positive for Ziehl-Neelsen staining, but tested negative with Xpert MTB/RIF or the LPA. This can be explained by the presence of a typical mycobacteria undetectable with these two techniques. Three INH-R/RIF-S isolates were identified, consistent with the suggestion that RMP is often the last antituberculous drug to be affected by resistance; note that the definition of multidrug resistance is the association of resistance to both RMP and INH (Kurbatova et al., 2012). Nevertheless, two isolates (4.16%) resistant to RMP were found, but susceptible to INH (RIF-R/INH-S). Other studies have reported the occurrence of such isolates, including that of Kurbatova et al. (2012), in which data from 14 supranational reference laboratories for cultures carried out in 112 laboratories in 80 countries were analyzed retrospectively. Isolates resistant to RMP and susceptible to INH were identified, with significantly lower levels of resistance to other first- and second-line antituberculous drugs (with the exception of rifabutin) than in MDR strains. A comparison of our results with published findings (Kurbatova et al., 2012) suggested that testing for resistance to RMP may not necessarily be the best approach to the diagnosis of probable MDR tuberculosis, with implications for the use of tests identifying only DNA mutations associated with RMP resistance (Kurbatova et al., 2012). Indeed, the two antibiotics considered here do not act on Mycobacterium tuberculosis in the same way. INH has powerful bactericidal activity against M. tuberculosis. This prodrug is activated by the KatG enzyme of M. tuberculosis, a catalase-peroxidase (Brossier, 2011). INH inhibits the synthesis of the mycobacterial cell wall, leading to cell death. About 80% of the strains resistant to INH carry point mutations or partial or complete deletions of the katG gene. Resistance to RMP is conferred by mutations of the rpoB gene (Brossier, 2011; Prasad et al., 2014).
With Xpert MTB/RIF and the LPA, high levels of resistance to RMP and INH in the patients studied were found, most of whom suffered from treatment failure or relapse. Xpert MTB/RIF is a high-performance test that is simple to use and can facilitate the detection of strains resistant to RMP, particularly in developing countries. The findings of this study demonstrate that some strains may be resistant to RMP, but susceptible to INH (4.16% in our study), resulting in their misclassification as MDR strains if testing for MDR strains is based exclusively on resistance to RMP. It would therefore be useful, if possible, to test strains identified as resistant to RMP for resistance to INH.
The authors have not declared any conflict of interests.
The authors thank all the staff of the National Antituberculosis Program in Senegal, including, in particular, the staff of the NATP laboratory and the staff of the hospitals at which the samples were collected.
REFERENCES
|
Brossier F (2011). Mechanisms of action and resistance to INH, a first-line antituberculous drug. J. Anti. infect. 10 (003).
view
|
|
|
|
Chevalier B, Margery J, Sane M, Camara P, Lefebvre N, Gueye M, Thiam M, Perrier-Gros-Claude JD, Simon F, Fabre M, Soler C, Herve V, Mbaye PS, Debonne JM (2010). Epidemiology of the resistance of Mycobacterium tuberculosis to antituberculosis drugs at the main hospital in Dakar, Senegal. A 4-year retrospective study (2000-2003). Rev. Pneumol. Clin. 66(4):266-271.
crossref
|
|
|
|
Diop SA, Fortes Déguénonvo L, Manga NM, Dia NM, Ka D, Hounsou AS, Ndour CT, Soumaré M, Seydi M (2014). Epidemiological, clinical and evolutionary aspects of tuberculosis retreatment patients. RMIM. 3:9-13.
view
|
|
|
|
FIND (2015). Line probe assay (1st line drugs).
|
|
|
|
Kouassi B, Horo K, N'douba KA, Koffi N, Ngom A, Aka-Danguy E, Dosso M (2004). Epidemiological, clinical and biological profile of pulmonary tuberculosis in situation of failure or relapse in Abidjan. Bull.Soc. Pathol. Exot. 97(5):336-337.
|
|
|
|
Kurbatova EV, Cavanaugh JS, Shah NS, Wright A, Kim H, Metchock B, Van Deun A, Barrera L, Boulahbal F, Richter E, Martin-Casabona N (2012). Rifampicin-resistant Mycobacterium tuberculosis: susceptibility to isoniazid and other anti-tuberculosis drugs. Int. J. Tuberc. Lung Dis. 16 (3):355-357.
crossref
|
|
|
|
Mbatchou NBH, Diatta A, Touré NO, Dia Kane Y, Ba Diop S, Ndiaye EH, Niang A, Sah Belinga A, Agodokpessi G, Ngakoutou R, Thiam K, Hane AA (2008). Clinical, biological and radiological spectrum of newly diagnosed pulmonary tuberculosis. Rev. Mal. Respir. 25:22-26.
|
|
|
|
Minime-Lingoupou F, Pierre-Audigier C, Kassa-Kélémbho E, Barilone N, Zandanga G, Rauzier J, Cadet-Daniel V, Le Faou A, Gicquel B (2010). Rapid identification of multidrug-resistant tuberculosis isolates in treatment failure or relapse patients in Bangui, Central African Republic. Int.J.Tuberc. Lung. Dis.14(6):782-785.
|
|
|
|
Prasad R, Gupta N, Singh M (2014). Multidrug-resistant tuberculosis: trends and control. Indian. J. Chest. Dis. Allied. Sci. 56:237-246.
|
|
|
|
National Antituberculosis Program (PNT), Senegal. Annual Report, 2013.
view
|
|
|
|
Rapid implementation of Xpert MTB/RIF (2011). WHO Report, Geneva. WHO/HTM/TB/ 2011.2.
view
|
|
|
|
Sangaré L, Diandé S, Badoum G, Dingtoumda B, Traoré AS (2010). Anti-tuberculosis drug resistance in new and previously treated pulmonary tuberculosis cases in Burkina Faso. Int. J. Tuberc. Lung. Dis. 14(11):1424-1429.
|
|
|
|
WHO (2015). WHO policy statement: molecular line probe assays for rapid screening of patients at risk of multidrug-resistant tuberculosis.
|