Full Length Research Paper

ABSTRACT
Asymptomatic bacteriuria, a form of urinary tract infections that involves isolation of a specified quantitative count of bacteria in an appropriately collected urine specimen obtained from a person without symptoms or signs referable to urinary infection is common, but the prevalence in population varies widely with age, sex and the presence of genitourinary abnormalities. This study therefore aimed at investigating the prevalence of asymptomatic bacteriuria among selected students of Faculty of Pharmacy, Obafemi Awolowo University, Ile-Ife Nigeria as well as the antibiotic resistance patterns of the bacterial isolates associated with the condition. Urine samples were collected from one hundred apparently healthy students and processed within two hours of collection. The isolates were identified by conventional biochemical tests while antibiotic susceptibility of the isolates were carried out according to the Clinical and Laboratory Standard Institute (CLSI) guidelines. Results revealed 77% prevalence (49 females, 27 males) among the sample studied with the presence of Staphylococcal spp., Klebsiella spp., Citrobacter spp. and Bacillus spp. Staphylococcus aureus is the predominant species accounting for 54.5% of the isolates. Antibiotic susceptibility study revealed all the isolates to be multidrug resistant. However, resistance to ofloxacin by Gram-negative bacterial isolates was least while resistance to streptomycin by the Gram-positive isolates was least in this study. The study concluded that multidrug resistant bacteria can be associated with asymptomatic bacteriuria while the patients may not develop any sign or symptom referable to urinary tract infection.
Key words: Asymptomatic bacteriuria, urinary tract infections, genitourinary abnormalities, prevalence, multidrug resistance.
INTRODUCTION
Urinary tract infections (UTIs) have been defined as the condition in which actively-multiplying bacteria persist in the urine at any point from kidney to the urethral meatus (Perrin, 1974). Hilbert (2011), however, defined urinary tract infection as the presence of a significant level of bacteria in urine typically 104 to 106 colony forming units (CFU/mL). Urinary tract infections (UTIs) are among the most frequent bacterial infections in human beings, affecting millions of people each year (Roos et al., 2006). They are the second most common type of infections in the body. (Stamm et al., 2001). UTI usually starts as a bladder infection but often evolves to encompass the kidneys and ultimately can result in renal failure or dissemination to the blood. Studies suggest that up to 95% of all UTIs develop by an ascending route of infection (Bacheller and Bernstein, 1997), meaning that infection begins by colonizing the periurethral area, followed by an upward progression to infect the bladder and, in some cases, continued progression of the bacteria through the ureters to infect the kidneys if conditions of infection allow. Transmission occurs in four ways; namely through sexual intercourse, from mother to the foetus via placenta, through poor personal hygiene and via communal sponge and towel usage (Onifade et al., 2011). UTIs may be with symptoms, that is, symptomatic or without symptom, that is, asymptomatic. Symptomatic UTIs can be classified as uncomplicated or complicated depending on patient comorbidities and the presence of anatomic or physiologic abnormalities that predispose to UTI (Mittal et al., 2009; Nicolle, 2008). It can also be classified into disease categories by the site of infection: Cystitis (the bladder), pyelonephritis (the kidney) and bacteriuria (the urine) (Foxman, 2002). Paradoxically, the most frequent form of UTI is asymptomatic bacteriuria (Roos et al., 2006). Asymptomatic bacteriuria (ABU) has been defined as colonization of urine by microorganisms in the absence of clinical symptoms (Roos et al., 2006). ABU patients may carry large number of bacteria, more than 105 CFU/ml, for months or years without developing symptoms. This condition is benign and does not cause renal injury (Oyelami et al., 2005). Most patients with ABU do not need treatment and in many cases the colonizing organism actually helps to prevent infection by other more virulent bacteria (Hull et al., 2000; Darouiche et al., 2001). ABU occurs in up to 6% of healthy individuals and 20% of elderly individuals (Roos et al., 2006).
However, although not in all cases, there is propensity for asymptomatic bacteriuria to become symptomatic if left untreated. Escherichia coli has been reported as the most prominent bacteria associated with asymptomatic bacteriuria but an increased percent of Proteus, Klebsiella, Enterococcus, and Pseudomonas has also been identified (Katsarolis et al., 2010). This study therefore aimed at investigating the occurrence of asymptomatic bacteriuria among some students of Faculty of Pharmacy, Obafemi Awolowo University, Ile-Ife as well as the antibiotic susceptibility profiles of isolated organisms to commonly used antibiotics.
MATERIALS AND METHODS
After ethical approval for the study was obtained from the OAUTHC Research and Ethical Committee, urine samples were collected from one hundred (45 males and 55 females) apparently healthy students of Faculty of Pharmacy, Obafemi Awolowo University, Ile-Ife, Nigeria. Prior to sample collection, consent forms were given to the students. The first part contained the Biodata of the students e.g. name, sex, age, past medical history as well as history of UTI.
The participating students were instructed to wash their external genital with mild toilet soap and rinse thoroughly with clean water. Thereafter, midstream urine was to be collected into the sterile specimen bottles, provided. The samples were labelled against the name of student in accordance with the supplied biodata. However, within two hours of collection, the samples were transported into the Pharmaceutical Microbiology Laboratory of the Department of Pharmaceutics for culturing. Students who were currently on antibiotics or have been on antibiotics treatments in the last three months were excluded from the study.
A loopful of the urine samples was streaked onto the surface of oven-dried Cysteine-Lactose Electrolyte Deficient (CLED) (Lab M, Bury, UK) agar and incubated at 37°C for 24 h. The colonies were counted and colony forming unit per millilitre (cfu/mL) calculated with a view to ascertaining if the growth was significant as to qualify for classification as asymptomatic bacteriuria or not.
The isolated colonies were identified by conventional biochemical tests (Barrow and Feltham, 2003).
Antibiotic susceptibility test
Susceptibility of both the Gram-negative and Gram-positive isolates to eight antimicrobial agents each was tested by the disc diffusion technique according to the guidelines of the Clinical and Laboratory Standards Institute (CLSI, 2012). The Gram-negative antibiotic disc contained augmentin (30 μg); ofloxacin (5 μg); gentamycin (10 μg); nalidixic acid (30 μg); nitrofurantoin (200 μg); cotrimoxazole (25 μg); amoxycillin (25 μg) and tetracycline (25 μg) while the Gram-positive antibiotic disc contained cotrimoxazole (25 μg); cloxacillin (5 μg); erythromycin (5 μg); gentamicin (10 μg); augmentin (30 μg); streptomycin (10 μg); tetracycline (10 μg) and chloramphenicol (10 μg).
Four or five colonies of each test organism taken from a nutrient agar culture plate were inoculated into 10 ml of sterile distilled water using a sterile loop. The suspension was thoroughly mixed with a spin mixer. The resulting suspension was adjusted to a turbidity of 0.5 McFarland standard (A625nm = 0.09). This was then applied to the surface of over-dried Mueller Hinton agar and spread evenly with a sterile swab stick. The inoculated plates were incubated at 37°C for 20 min for acclimatization and growth of the inocula. Antibiotic discs (Abtek, Liverpool, UK) were then lightly but firmly pressed onto the surface of the plates using a pair of sterile forceps. The plates were then refrigerated at 4°C for thirty minutes to ensure adequate diffusion of antibiotics. E. coli ATCC 25922 was used as control strain. All plates were incubated at 37°C for 18 h. The diameters of inhibition zones were measured in millimetres and interpreted according to CLSI manual.
RESULTS
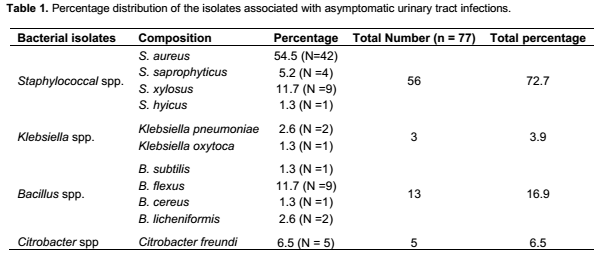
Hundred samples were collected out of which 77 had significant growth after inoculating and incubating on the C.L.E.D agar. Of these 77 isolates, 49 (63.6%) were from the female subjects while 28 (36.4%) were from the male subjects.
In this study, four genera of bacteria were isolated. These include Staphylococcal spp., Klebsiella spp., Citrobacter spp. and Bacillus spp. The percent distribution of each spp. is as shown in Table 1.
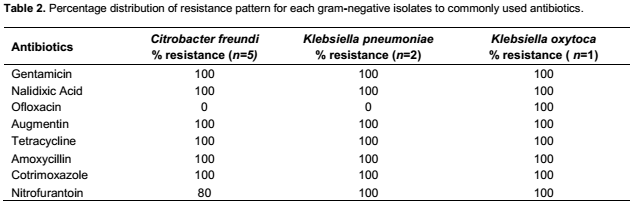
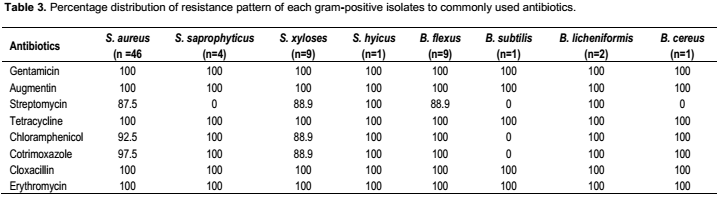
The percentage distribution of resistance patterns of Gram-negative bacterial isolates is shown in Table 2. The resistance to ofloxacin by all Gram-negative bacterial isolates is the least among the antibiotics used except the Klebsiella oxytoca that was resistant to all the antibiotics tested in the study while resistance to streptomycin is the least by Gram-positive bacterial isolates with the exception of Staphylococcus hyicus and Bacillus licheniformis that have 100% resistance to streptomycin as shown in Table 3.
DISCUSSION
Stamm and Hooton (1993) referred to UTI as a clinical (symptomatic) or subclinical (asymptomatic) disease that may involve just the lower tract or both the lower and upper tracts. “Asymptomatic bacteriuria,” or asymptomatic urinary infection, has been defined as isolation of a speciï¬ed quantitative count of bacteria in an appropriately collected urine specimen obtained from a person without symptoms or signs referable to urinary infection (Rubin et al., 1992).
Asymptomatic bacteriuria is common, but the prevalence in populations varies widely with age, sex, and the presence of genitourinary abnormalities (Nicolle et al., 2005). In this study, the prevalence of asymptomatic bacteriuria in the population of students studied was 77%. This was significantly higher than those earlier reported (Onifade et al., 2011; Ngwai and Bakare, 2012; Adekunle et al., 2013; Ayoade et al., 2013). This may be attributed to unhygienic living conditions students were subjected to on campus and /or poor personal hygiene on the part of the students. In this study, more females than males (63.6% vs 36.4%) had asymptomatic bacteriuria. This, while in agreement with those earlier reported (Onifade et al., 2011; Adekunle et al., 2013) however contradicts the findings of Ngwai and Bakare (2012). This may be attributed to anatomical differences between male and female urinary tracts. For instance, the urethra of female is shorter than in male thus allowing bacteria a more ready access to the bladder. Also, the urethral opening in women is closer to sources of bacteria from the anus and the vagina (Lipsky, 1989). One other reason for lower incidence in male than female is the antibacterial property of prostatic fluid (Onifade et al., 2011). However, the prevalence of bacteriuria among young women is strongly associated with sexual activity. It was 4.6% among premenopausal married women but only 0.7% among nuns of similar age (Kunin and McCormack, 1968).
Escherichia coli remains the single most common organism isolated from bacteriuric women (Kunin and McCormack, 1968; Evans et al., 1978; Bengtsson et al., 1998), although this happens proportionally less frequently than for women with acute uncomplicated urinary tract infection. Other Enterobacteriaceae (such as Klebsiella pneumoniae) and other organisms (including coagulase-negative staphylococci, Enterococcus species, group B streptococci, and Gardnerella vaginalis) are common as well. For men, coagulase-negative staphylococci are also common, in addition to gram-negative bacilli and Enterococcus species (Lipsky et al., 1984; Mims et al., 1990). In this study, four genera of bacteria were isolated. They include Staphylococcal spp., Klebsiella spp., Bacillus spp. and Citrobacter spp. Of these, Staphylococcal spp. was the predominant genera accounting for 72.7%. Staphylococcus aureus, among others as S. saprophyticus S. hyicus and S. xylosus, has the highest occurrence of 54.5%. This agrees with the report of Frank-Peterside and Wokoma (2009). The findings however contradicts the reports of Adekunle et al. (2013) and Onifade et al. (2011) where E. coli was reported the predominant species of bacteria isolated.
S. aureus is a common pathogen in the community and in hospitals. S aureus causes significant mortality and morbidity but is an infrequent cause of urinary tract infection (Demuth et al., 1979). In patients with S. aureus bacteremia, a positive urine culture is typically attributed to ascending infection or to hematogenous spread. Coagulase positive Staphylococci may have invaded the UTI through hematogenous routes while the coagulase negative Staphylococci may invade the urinary tract through sexual activity especially in females (Frank-Peterside and Wokoma, 2009).
It is however possible that the S. aureus isolated in this study may have gotten into the urinary tract by the individuals inadvertently touching their genitalia with hands that have been used to touch infected surfaces since S. aureus infections are spread by contact.
All the isolates in this study are multidrug resistant with many resistant to four or more antibiotics tested. This may be attributed to the isolates possessing genes that code for multidrug resistance. Some of the ways by which bacteria can develop resistance to antibiotics include: (i) Antibiotic inactivation- direct inactivation of the active antibiotic molecule (Wright, 2005); (ii) Target modification- alteration of the sensitivity to the antibiotic by modification of the target (Lambert, 2005); (iii) Efflux pumps and outer membrane (OM) permeability changes- reduction of the concentration of drug without modification of the compound itself (Kumar and Schweizer, 2005); or (iv) Target bypass- some bacteria become refractory to specific antibiotics by bypassing the inactivation of a given enzyme. This mode of resistance is observed in many trimethoprim- and sulfonamide-resistant bacteria. This observation corroborates the postulation that healthy members of the community are the highest reservoir of antibiotic resistant bacteria (Lester et al., 1990; Lamikanra et al., 1996). Ofloxacin, a fluoroquinolone, and streptomycin, an aminoglycoside, are the drugs of choice with the least resistance by Gram-negative and Gram-positive isolates respectively in this study. Ofloxacin exerts its antibacterial effect by disrupting DNA synthesis through interference with type II topoisomerases DNA gyrase and topoisomerase IV during replication and by causing double strand breaks (Strohl, 1997). Resistance could be developed to ofloxacin by alterations in drug target enzymes and alterations that limit the permeability of the drug to the target (Hooper, 1999).
The bactericidal activity of streptomycin is attributed to the irreversible binding to the ribosomes. Resistance to streptomycin is through modification of the target sites by enzymes as aminoglycoside acetyltransferases (AAC), aminoglycoside adenyltransferases (also named aminoglycoside nucleotidyltransferases [ANT]), and aminoglycoside phosphotransferases (APH) (Shaw et al., 1993). The activity of these enzymes is not restricted to streptomycin alone but other members of the aminoglycosides group.
Aminoglycosides modified at amino groups by AAC enzymes or at hydroxyl groups by ANT or APH enzymes lose their ribosome-binding ability and thus no longer inhibit protein synthesis. Besides aminoglycoside-modifying enzymes, efflux systems and rRNA mutations have been described (Quintiliani and Courvalin, 1995).
CONCLUSION
The high prevalence of asymptomatic bacteriuria among apparently healthy students as obtained in this study is of public health concern and need to be addressed. The high prevalence may be attributed to poor public and personal hygiene going by the nature of the isolates in this study hence the need for public enlightenment to promote good personal hygiene and hand washing among others. Also living and environmental conditions of the students should be improved through regular sanitation and regular provision of potable water.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interest.
ACKNOWLEDGEMENT
The authors are grateful for the role played by Mr Salau A. O., the Principal Technologist in Pharmaceutical Microbiology Unit of the Department of Pharmaceutics, Faculty of Pharmacy, Obafemi Awolowo University, Ile-Ife, Nigeria in the course of this work.
REFERENCES
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


