ABSTRACT
The aim of this study is to investigate the burden of basic diseases, the epidemiology of pathogenic microbes in patients with bloodstream infections and their clinical biomarkers. Data on bloodstream infections from 2012 to 2018 were obtained from a 3A General Hospital in Lanzhou of China. 1990 patients with bloodstream infections participated in the study; their basic diseases, pathogenic microorganisms and corresponding clinical laboratory biomarkers such as procalcitonin (PCT), C-reactive protein (CRP), interleukin-6 (IL-6), neutrophil% (NEU%), blood lactate (LAC) and D-Dimer were recorded. 722 cases with non-bloodstream infections were selected randomly as control group. 8.9% of the patients had positive blood culture. The contamination rate was 0.24%. 1043 strains were isolated belonging to 75 species; they contained Gram negative bacilli, Gram-positive cocci, anaerobic and fungi accounting for 62.00, 31.64, 2.40 and 2.01%, respectively. Statistical analysis showed that hematopathy was the most frequent disease caused by bloodstream infections (number of episodes per years: 56 overall) and it accounted for 16.88%; this is followed by hepatobiliary diseases, central nervous system diseases, urinary disease, respiratory diseases and digestive tract disease which accounted for 12.31, 11.61, 10.75, 6.35 and 9.95%, respectively. Receivers operators characteristics (ROC) curve was used to evaluate the biomarker for diagnostic value of bloodstream infections, and the AUC values of NEU%, PCT, IL-6, CRP, D-Dimer and LAC were 0.974, 1.000, 1.000, 0.438, 0.932 and 0.784, respectively. This study documents a very timely picture of the strains of the bloodstream infections epidemiology in a 3A General Hospital over a 6-year period, the basic diseases with bloodstream infections in patients, and the biomarker diagnostic value for BSIs. PCT and IL-6 can be used as rapid and accurate biomarkers for bloodstream infections caused by bacteria.
Key words: Bloodstream infections, pathogenic microorganisms, basic diseases, biomarkers, receivers operators characteristics (ROC) curves.
Bloodstream infection (BSI) is a serious systemic infectious disease in which pathogenic microorganisms are transient, intermittent or persistent in the blood circulation, that can cause serious damage to the body, can lead to shock, multiple organ failure (MODS), disseminated intravascular coagulation (DIC) or even death (Murrary, 2003). Bloodstream infections cause mortality worldwide (Pien et al., 2010) such as bacteremia, sepsis and central venous catheters (CVCS) BSI. They can be clinically diagnosed by blood cultures, leading to approximately 157,000 deaths per year in Northern Europe and more than 79,000 deaths per year in North America (Goto and Al-Hasan, 2013).The directory for BSIs diagnosis and treatment released by the Surviving Sepsis Campaign (SSC) (Dellinger et al., 2004, 2008) shows that early identification and effective intervention will significantly improve prognosis and reduce death rate (Otero et al., 2006). Current clinical biomarkers with wide application in the rapid and accurate diagnosis of bacterial infections (Müller et al., 2000; Charchaflieh et al., 2015; Su et al., 2013) include NEU%, C-reactive protein (CRP), procalcitonin (PCT), IL-6, blood D-Dimers and blood Lac. If etiological evidence is not identified timely, about 30% of the relevant diagnoses would not be well grounded pathologically (Gibot and Cravoisy, 2004); so we collected the most accurate clinical biomarkers for clinical diagnose of bloodstream infections.
Recently, PCT has been put to a wide clinical use because it is a biomarker that indicates infection caused by bacteria (Bhatia and Basu, 2007), and predicts cases of infectious diseases (Bloos et al., 2011; Giamarellos et al., 2011). There are also some non-infection factors such as trauma and acute respiratory syndrome that can lead to increased PCT (Bhatia and Basu, 2007). Another biomarker is CRP that is involved in more than one inflammatory cascade amplifications; it is now widely applied in sepsis diagnosis. Some scholars have shown that CRP is not an ideal biomarker in this field (P´ovoa, 2002). Interleukin-6 (IL-6) is a pleiotropic immune molecule that serves both as a pro-inflammatory cytokine to stimulate the immune response during infection, and even occurs in the absence of infection, such as in hay fever or atherosclerosis(Napolioni and MacMurray, 2016). The blood lactic acid can also be used to evaluate disease severity and prognosis with sepsis. It is a sensitive indicator for severe infection, systemic oxygen metabolism and tissue (Yan et al., 2016; Lee et al., 2008; Singer et al., 2016). The D-dimer (DD) as well as other biomarkers related to coagulation is significantly increased during sepsis and especially when developing disseminated intravascular coagulation (DIC). The high levels of DD are associated with 28-day mortality in patients with infection or sepsis identified in the emergency department (Rodelo et al., 2012). The present study makes a comparison of five biomarkers including PCT, CRP, NEU%, IL-6 and blood lactic acid (B-Lac) to explore which of them is more valuable in BSIs diagnosis, as well as in the prediction of its development and prognosis. Hopefully, our findings could prove to be of some help to clinicians in general.
Blood culture and pathogenic microbes
All the subjects were recorded episodes from inpatients who were hospitalized between January 2012 and January 2018 in a 3A General Hospital, LanZhou of China. The results of positive blood culture caused by bacteria and the corresponding infection biomarkers within 24 h, including CRP, PCT, NEU%, IL-6, D-dimer, Lac, and their basic disease were also recorded. We selected 722 cases with non-bloodstream infections as a negative control group; we recorded all the results of negative blood culture and the corresponding infection biomarkers within 24 h. The definition of culture contaminated bacteria is that in several blood cultures, the single bottle of blood culture is positive for the following bacteria: coagulase negative staphylococcus, Corynebacterium, Micrococcus, Propionibacterium and so on.
Blood cultures were obtained using BacT/ALERT (bio-Mérieux, Inc, Durham, NC), aerobic FA and anaerobic SN blood culture bottles. They were incubated in the BacT/ALERT 3D (bioMérieux, Inc) automatic monitoring system for a week in the clinical microbiology laboratory of the hospital. Bottles flagged as positive were Gram stained and subcultured. VITEK 2 system (bioMérieux, Inc, Durham, NC) was used for species-level ID and AST of most antimicrobial agents. During the study period, microbiology laboratory personnel at the study hospital notified the primary team prescriber via phone regarding the Gram-stain ID of any positive blood culture within 15 min of a positive result (Jesús et al., 2010). They reviewed a printed list of positive blood cultures supplied by the microbiology laboratory once daily in the morning and intervened on patients with BSIs. Infectious diseases were diagnosed at the discretion of the primary team.
An episode of BSIs was defined by the growth of one or more microbes from blood culture combined with clinical evidence of systemic infection (Levy et al., 2003; Mehl et al., 2017). BSIs strains included both first-time and repeat episodes in a week (Riedl and Carroll, 2010). One positive blood culture for organisms regarded as etiological agents was the requirement for inclusion. For coagulase-negative staphylococci, alphahemolytic streptococci, or other possible skin contaminants, at least two identical isolates from separate venipunctures were required.
Etiology of bloodstream infection
The hospital receives updated information on Lis status of the patients from register, and thus information on etiology of BSI was complete even if the patient was discharged from hospital. An etiology focus was assigned when the microbe was isolated from blood culture along with clinical signs/symptoms or risk factors for infection; and no other source of infection were identified. Therefore, we identified 21 basic diseases in patients with blood infections through clinical diagnosis.
Serum inflammatory biomarker detection
Serum samples for PCT, CRP IL-6 and D-dimer were collected in a dry tube with gel separator and centrifuged within the first 2 h. PCT and IL-6 were detected by E-170 automatic analyzer (Roche), and the cut-off value is 0.046 and 70.046 ng/ml. C-reactive protein was measured quantitatively by an immunoturbidimetric assay using an ARCHITECT c-System (Abbott Laboratories, IL, USA). The detection limit was 0.5 mg/dL, and the imprecision of the assay was 5% or less of the total coefficient of variation, as reported by the manufacturer. D-dimer was measured by aturbidimetric immunoassay in an CS-2100i/2000i(SYSMEX, Japan), and the cut-off value is 0.55 mg/L. Blood lactic acid was measured by blood gas analysis instrument (nova, American).
ROC cure analysis of biomarkers in diagnosis of bloodstream infections
The area under curve (AUC) of receiver operating characteristic (ROC) was constructed to evaluate the diagnostic value of serum biomarkers for predicting BSIs, and the ideal cut-off criteria for the laboratory results were chosen by determining the point lying geometrically closest to an ideal test with 100% specificity and sensitivity. The biomarkers as a clinical screening index for clinical bloodstream infection must have high sensitivity. For statistical analysis, SPSS 17.0 statistical software was used, and a two-tailed p<0.05 was considered significant.
Pathogenic microorganisms of bloodstream infections
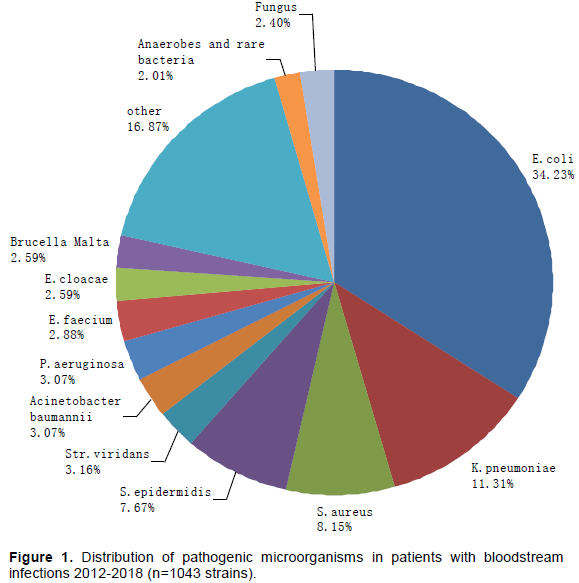
From 2012 to 2018, a total of 4025 positive blood cultures were identified from 45151 individual; 8.9% had positive blood culture, and the contamination rate was 0.24%. 1043 strains belong to 75 species, and contain Gram negative bacilli, Gram-positive cocci, anaerobic and rare species such as fungi accounting for 62, 31.64, 2.40 and 2.01%, respectively (Figure 1). Escherichia coli was the most frequent agent (34.2% overall), followed by Klebsiella pneumoniae (11.3%), Staphylococcus aureus (8.15%). Staphylococcus epidermidis (7.76%), Streptococcus viridans (3.16%), Acinetobacter baumannii (3.07%), Pseudomonas aeruginosa (3.07%), Enterococcus faecium (2.88), Enterobacter cloacae (2.59%) and Brucella Malta (2.59%).
Burden of basic diseases on bloodstream infections
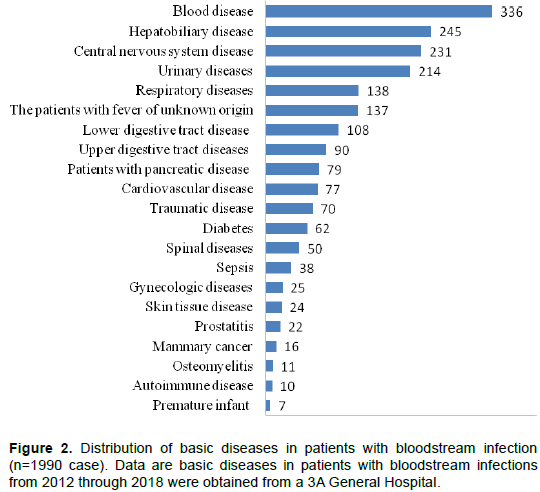
During 2012 to 2018 study period, a total of 1990 persons had bloodstream infections and we defined 21 types of basic diseases in patients with bloodstream infections by clinical diagnosis (Figure 2). Hematopathy was the predominant disease caused by bloodstream infections (number of episodes per years: 56 overall) accounting for 16.88%, followed by hepatobiliary disease, central nervous system disease, urinary disease respiratory disease and digestive tract disease, accounting for 12.31, 11.61, 10.75, 6.35 and 9.95%, respectively. Patients with fever of unknown origin make up a large number of the overall group (6.88%).
Disease types included in the patients' underlying disease were defined. Hepatobiliary disease includes cholecystitis, liver cancer, etc.; central nervous system disease includes disturbance of consciousness, cerebrovascular disease, intracranial infection and subarachnoid hemorrhage, etc.; urinary diseases include renal calculi, ureteral calculi, urinary tract infection, uremia and renal insufficiency etc.; respiratory diseases include pneumonia, lung infection, upper respiratory tract infection, lung cancer etc.; lower digestive tract disease includes abdominal infection, colitis, colorectal cancer etc.; upper digestive tract diseases include gastric cancer, cancer, esophageal cancer, cardiac, gastrointestinal bleeding, etc.; cardiovascular disease includes arterial dissection, heart muscle ischemia and infective endocarditis; gynecologic diseases include hysterectomy, myoma of uterus, cancer of the cervix, etc.; skin tissue disease includes skin and soft tissue infections, global disease, cellulitis skin disease, and traumatic disease includes traumatic craniocerebral injury, trauma, fracture, burn, etc.
Data on basic diseases in patients with bloodstream infections from 2012 to 2018 were obtained from a 3A General Hospital.
Application of cut-off value of inflammatory biomarkers in diagnosis of bloodstream infections
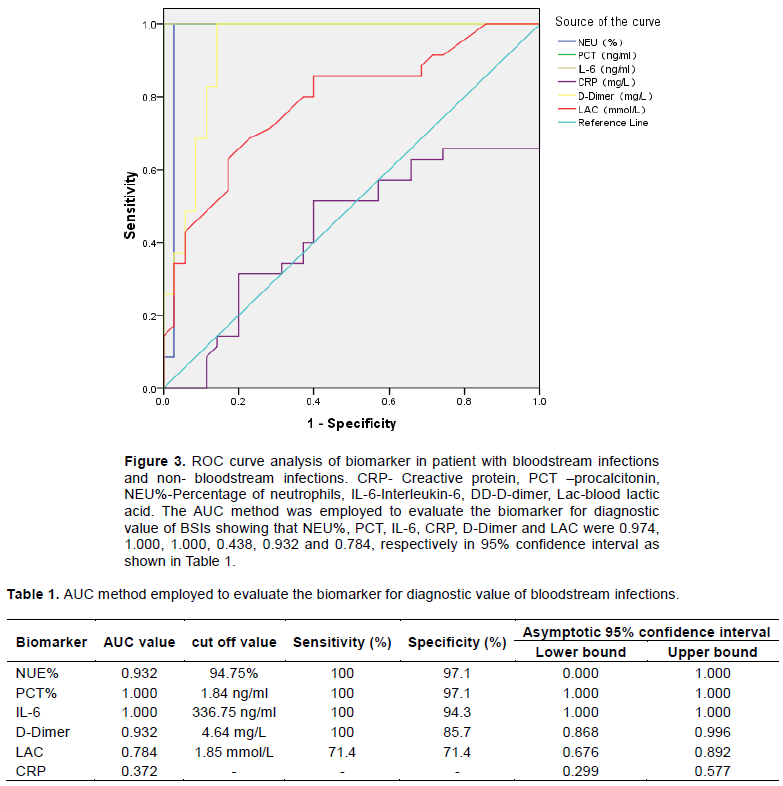
The discriminatory ability for bloodstream infections, as determined by the AUC-ROC for each biomarker is presented. For overall bloodstream infections, the AUC-ROC value for NUE was 0.932%; when the cut off value of NEU% is 94.75%, the sensitivity and specificity are 100 and 97.1% respectively; the AUC-ROC value for PCT was 1.000; when the cut off value of PCT is 1.84 ng/ml, the sensitivity and specificity are 100 and 97.1%, respectively; the AUC-ROC value for IL-6 was 1.000; when the cut off value of IL-6 is 336.75 ng/ml, the sensitivity and specificity are 100 and 94.3% respectively; the AUC-ROC value for D-Dimer was 0.932; when the cut off value of D-Dimer is 4.64 mg/L, the sensitivity and specificity are 100 and 85.7%, respectively; the AUC-ROC value for LAC was 0.784; when the cut-off value of LAC is 1.85 mmol/L, the sensitivity and specificity are 71.4 and 71.4%, respectively (Figure 3).
CRP-Creactive protein; PCT-procalcitonin; NEU%-Percentage of neutrophils; IL-6-Interleukin-6,DD-D-dimer, Lac-blood lactic acid. The AUC method was employed to evaluate the biomarker for diagnostic values of BSIs. NEU%, PCT, IL-6, CRP, D-Dimer and LAC were 0.974, 1.000, 1.000, 0.438, 0.932 and 0.784, respectively in 95% confidence interval (Table 1).
Bloodstream infection is a serious systemic infectious disease in which pathogenic microorganisms are transient, intermittent or persistent in the blood circulation; they can cause damage to the body, lead to serious shock, MODS, DIC, or even death (Murrary, 2003). It can be clinically diagnosed by blood cultures, and its microbial identification and drug sensitivity results are the bases needed for the accurate treatment of clinical infected patients (Baron et al., 2013; Laupland, 2013). From 2012 to 2018 episodes, 8.9% had positive blood culture, lower than the domestic reports of 15.1% (Laupland, 2013). Of these, 1043 strains belong to 75 species having Gram negative bacilli, Gram-positive cocci, anaerobic and rare species, fungi; they account for 62, 31.64, 2.40 and 2.01%, respectively. That means the strains were very complex in patients with bloodstream infections. So it is very important to do blood culture and find etiology evidence for the treatment of patients. E. coli was the most frequent agent (Wilson et al., 2011; Skogberg et al., 2012); it is usually considered as a pathogen acquired in the community, it causes HA-BSI and is the most detected across all hospital areas. It is followed by K. pneumoniae (11.3%). This report is different from other reports (Wilson et al., 2011; Skogberg et al., 2012; Buetti et al., 2015). As the main pathogen of bloodstream infection, E. coli is mainly seen in the intestine, which may be caused by the damage of the intestinal mucosa or the rupture of the intestine. S. aureus (8.15%) is the third frequent pathogen identified and Methicillin resistant S. aureus (MRSA) is 2.97%. It may relate to more methicillin-susceptible antibiotics widely used for MRSA bacteremias prevalent in hospital infection concurrently (David et al., 2014). In our data, Brucella Malta (no. of strain per years: 4.5) was the eighth frequent pathogen identified; it is a source of human infection that always resides in domestic or wild animal in our region (Godfroid et al., 2005).
The increased incidence of bloodstream infections is usually caused by the widespread use of immunosuppressive agents, broad-spectrum antibiotics, extensive and medical operations; and the hospital bloodstream infections still pose a serious threat to the life of patients. The document showed (Laupland et al., 2018; Ballard et al., 2016) that the risk factors of bloodstream infections include: damage to the integrity of the function of an organism such as damage to the skin and mucous membrane, indwelling central venous catheter, indwelling catheter, tracheal intubation or tracheotomy, decreased immunity of the body, use of catheters, malignant tumors of the blood system and diabetic patients. Our finding shows that hematopathy was the predominant site of infection (number of episodes per years: 56 overall) accounting for 16.88%, followed by hepatobiliary disease, central nervous system disease, urinary disease, respiratory disease and digestive tract diseases. For the Hematology/Oncology Units patients, upper or lower gastrointestinal tract mucositis or skin breakdown is common, and also variability in adjudicating central line-associated bloodstream infections needs to be addressed (Gaur et al., 2013). Urinary tract infections are usually common in elderly patients (Esposito et al., 1980), and the mortality rate is approximately 10 to 20% despite appropriate treatments in patients with bacteremia (Sugiyama and Atomi, 1997). The increased risk for bloodstream infections conferred by urinary disease is consistently related to reduced bacterial clearance. This is due to decrease in urinary flow or other changes such as reduced urinary antimicrobial concentrations, or altered local immune function (Bursle et al., 2015). It is found that higher Charlson comorbidity index or catheters inserted for accurate urine output monitoring likely reflect a predisposition to chronic and acute illness, respectively. The central nervous system disease caused by bloodstream infections include disturbance of consciousness disease, cerebrovascular disease, intracranial infection and subarachnoid hemorrhage. The overgrowth of potentially pathogenic microorganisms (PPMs) in the patients’ oropharynx is the major risk factor for lower respiratory tract infections and of subsequent invasion from the lungs into the bloodstream (Garrouste et al., 1997). Upper or lower gastrointestinal tract is caused by bloodstream infections due to mucositis or skin breakdown, when variability in adjudicating central line-associated bloodstream infections is concerned and needs to be addressed. So it is caused by bacterial bloodstream infections in critically ill patients. Patients with fever of unknown origin and sepsis patients have a surface phenomenon; it is necessary for them to actively seek and clear the infections. There are other reasons for bloodstream infections such as venous catheters, indwelling catheters, tracheal cannula or tracheotomy wildly used. It is necessary to treat critically ill patients. Therefore, patients with bloodstream infections should follow hospital infection control, antibiotic management and self- rehabilitation to reduce the incidence of the infections.
About 15% of the patients had bacteremia, but the blood culture was negative. Therefore, the establishment of more valuable biomarkers in BSIs diagnosis has become a research hotspot (Gibot and Cravoisy, 2004; Bhatia and Basu, 2007). The AUC values used to evaluate the biomarker for the diagnosis of bloodstream infections showed that NEU%, PCT, IL-6, CRP, D-Dimer and LAC were 0.974, 1.000, 1.000, 0.438, 0.932 and 0.784, respectively. Dates indicated that the accuracy of prediction for bloodstream infection was PCT=IL-6>NEU%>D-Dimer>LAC. Serum PCT and IL-6 levels significantly increased when the bacterial toxin was stimulated. They were reliable early prognostic marker in patients with BSIs, respectively. This is similar to Clec'h et al. (2006) and Napolioni and MacMurray (2016) who recommend most specific biomarkers by MEDS score (mortality in emergence Department sepsis score). The other biomarker was NEU%, its sensitivity and specificity for bloodstream infections were 100 and 97.1%, respectively. As the shock progressed, the total number of leukocytes and neutrophils increased significantly (neutrophils more than 80%), and there was a leukemic reaction. D-dimer is a significant prognostic factor in patients with suspected infection and sepsis. Rodelo et al. (2012) demonstrated the discriminatory ability showed area under the ROC for DD, 0.68, with an odds ratio of 2.07 (95% confidence interval, 0.93-4.62) for values more than 1180 and less than 2.409 mg/mL and an odds ratio of 3.03 (95% confidence interval, 1.38-6.62) for values more than 2.409 mg/mL. But, our study shows that the AUC-ROC value was D-Dimer 0.932; when the cut off value of D-Dimer is 4.64 mg/L, the sensitivity and specificity are 100 and 85.7%, respectively. For sepsis (Lee et al., 2008) it is demonstrated that blood lactic acid more than 4.0mmol/L is significant for diagnosing lactic acidosis, and it is a sensitive biomarker for detecting and evaluating severe infection, septic shock, systemic oxygen metabolism and tissue attention. Lactic acid can respond to the severity of sepsis in tissue metabolism, but it is not very specific for the diagnosis of sepsis. Our data indicated the AUC-ROC value was LAC 0.784. There was a good correlation between CRP levels and the severity of sepsis and other inflammatory diseases (Povoa et al., 1998); but our study indicated that CRP has significant difference (T test p=0.372, <0.05). Therefore, PCT and IL-6 can be used as convenient auxiliary diagnostic biomarkers for patients with bloodstream infection caused by bacteria.
In conclusion, this study documents a very timely picture of the bloodstream infections epidemiology in a 3A General Hospital over a 6-year period, the burden of basic diseases with bloodstream infections in patients, and the biomarker diagnostic value for bloodstream infections. PCT and IL-6 can be used as rapid and accurate biomarkers measurement and etiological diagnosis for bloodstream infections by caused by bacteria.
In this context, we analyzed the burden of basic diseases caused by BSIs in patients by clinical diagnosis, but we did not investigate the first site which the pathogenic bacteria invade into the blood stream. We need to be more accurate to understand the BSIs occurrence. Furthermore, we did not distinguish the pathogen that is community acquired (CA) and hospital acquired (HA) in BSIs. It may be useful to control hospital infection and treat severe disease to prevent the occurrence of BSIs. Finally, we did not provide data on resistance of microorganisms, which are essential for decision-making about empirical antimicrobial therapies.
The authors have not declared any conflict of interests.
The authors thank their competent technician for diligent and accurate work in the data collection process. They thank the staff at the Microbiology Laboratory, Lanzhou General Hospital of Lanzhou Military Area, for consecutively including cases and sending registration forms to physicians treating the patients at the wards.
REFERENCES
|
Ballard MS, Schønheyder HC, Knudsen JD (2016). The changing epidemiology of group B streptococcus bloodstream infection: A multi-national population-based assessment. Infectious Diseases (Lond) 48(5):386-391.
Crossref
|
|
|
|
Baron EJ, Miller JM, Weinstein MP (2013). A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infections Disease: 2013 Recommendations by the Infections Disease Society of America (IDSA) and the American Society for Microbiology (ASM). Clinical Infectious Diseases 33(24):3020-3021.
|
|
|
|
|
Bhatia BD, Basu S (2007). Newer diagnostic tests for bacterial disease. Indian Journal of Pediatrics 74(7):673- 677.
Crossref
|
|
|
|
|
Bloos F, Marshall JC, Dellinger RP (2011). Multinational, observational study of procalcitonin in ICU patients with pneumonia requiring mechanical ventilation: A multicenter observational study. Critical Care 15(2):88.
Crossref
|
|
|
|
|
Buetti N, Marschall J, Atkinson A (2015). National Bloodstream Infection Surveillance in Switzerland 2008-2014: Different Patterns and Trends for University and Community Hospitals. Arquivos Brasileiros De Oftalmologia 37(9):1060-1067.
Crossref
|
|
|
|
|
Bursle EC, Dyer J, Looke DF (2015). Risk factors for urinary catheter associated bloodstream infection. Journal of Infection 70(6):585-591.
Crossref
|
|
|
|
|
Charchaflieh J, Rushbrook J, Worah S (2015). Activated Complement Factors as Disease Markers for Sepsis. Disease Markers 2015:382-463.
Crossref
|
|
|
|
|
Clec'h C, Fosse JP, Karoubi P (2006). Differential diagnostic value of procalcitonin in surgical and medical patients with septic shock. Critical Care Medicine 34:102-107.
Crossref
|
|
|
|
|
David MZ, Daum RS, Bayer AS (2014). Staphylococcus aureus bacteremia at 5 US academic medical centers, 2008-2011: significant geographic variation in community-onset infections. Clinical Infectious Diseases 59:798-807.
Crossref
|
|
|
|
|
Dellinger RP, Carlet JM, Masur H (2004). Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock Critical. Intensive Care Medicine 32(3):858-873.
Crossref
|
|
|
|
|
Dellinger RP, Levy MM, Carlet JM (2008). Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Medicine 34(1):17-60.
Crossref
|
|
|
|
|
Esposito AL, Gleckman RA, Cram S, Crowley M, McCabe F (1980). Community‑acquired bacteremia in the elderly: Analysis of one hundred consecutive episodes. Journal of the American Geriatrics Society 28:315‑319.
Crossref
|
|
|
|
|
Garrouste OM, Chevret S, Arlet G (1997). Oropharyngeal or gastric colonization and nosocomial pneumonia in adult intensive care unit patients: A prospective study based on genomic DNA analysis. American Journal of Respiratory and Critical Care 156:1647-1655.
Crossref
|
|
|
|
|
Gaur AH, Miller MR, Gao C (2013). Evaluating application of the National Healthcare Safety Network central line-associated bloodstream infection surveillance definition: A survey of pediatric intensive care and hematology/oncology units. Infection Control and Hospital Epidemiology 34(7):663-670.
Crossref
|
|
|
|
|
Giamarellos EJ, Tsangaris I, Kanni T (2011). Procalcitonin as an early indicator of outcome in sepsis: A prospective observational study. Journal of Hospital Infection 77(1):58-63.
Crossref
|
|
|
|
|
Gibot S, Cravoisy A (2004). Soluble form of the triggering receptor expressed on myeloid cells-1 as a marker of microbial infection. Clinical Medicine and Research 2(3):181-187.
Crossref
|
|
|
|
|
Godfroid J, Cloeckaert A, Liautard JP (2005). From the discovery of the Malta fever's agent to the discovery of a marine mammal reservoir, brucellosis has continuously been a re-emerging zoonosis. Veterinary Research 36(3):313-326.
Crossref
|
|
|
|
|
Goto M, Al-Hasan MN (2013). Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clinical Microbiology and Infection 19:501-509.
Crossref
|
|
|
|
|
Jesús RB, Marina C, Retamar P (2010). Current management of bloodstream infections. Expert Review of Anti-Infective Therapy 8(7):815-829.
Crossref
|
|
|
|
|
Laupland KB (2013). Incidence of bloodstream infection: A review of population-based studies. Clinical Microbiology and Infection 19:492-500.
Crossref
|
|
|
|
|
Laupland KB, Niven DJ, Pasquill K (2018). Culturing rate and the surveillance of bloodstream infections: A population-based assessment. Clinical Microbiology and Infection 24(8).
Crossref
|
|
|
|
|
Lee SW, Hong Ys, Park DW (2008). Lactic acidisis not hyperlactatemia as a predicyor of in-hospital mortality in sepsis emergency patients. Emergency Medicine Journal 25(10):659-665.
Crossref
|
|
|
|
|
Levy MM, Fink MP, Marshall JC (2003). 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Medicine 29(4):530-538.
Crossref
|
|
|
|
|
Mehl A, Åsvold BO, Lydersen S (2017). Burden of bloodstream infection in an area of Mid-Norway 2002-2013: A prospective population-based observational study. BMC Infectious Diseases 17(1):205.
Crossref
|
|
|
|
|
Müller B, Becker KL, Schächinger H (2000). Calcitonin precursors are reliable markers of sepsis in a medical intensive care unit. Critical Care Medicine 28(4):977-983.
Crossref
|
|
|
|
|
Murrary PR (2003). Manual of clinical microbiology. 8th ed. Washington: ASM 234-246.
|
|
|
|
|
Napolioni V, MacMurray J (2016). Infectious diseases, IL6 -174G>C polymorphism, and human development. Brain Behavior and Immunity 51:196-203.
Crossref
|
|
|
|
|
Otero RM, Nguyen HB, Huang DT (2006). Early goal-directed therapy in severe sepsis and septic shock revisited: Concepts, controversies, and contemporary findings. Chest 130(5):1579-1595.
Crossref
|
|
|
|
|
P'ovoa P (2002). C-reactive protein: A valuable marker of sepsis. Intensive Care Medicine 28(3):235-243.
Crossref
|
|
|
|
|
Pien BC, Sundaram P, Raoof N (2010). The clinical and prognostic importance of positive blood cultures in adults. The American Journal of Medicine 123:819-828.
Crossref
|
|
|
|
|
Povoa P, Almeida E, Moreira P (1998). C-reactive protein as an indicator of sepsis. Intensive Care Medicine 24:1052-1056.
Crossref
|
|
|
|
|
Riedl S, Carroll KC (2010). Blood culture: key elements for best practices and future directions. Journal of Infection and Chemotherapy 16(5):301-316.
Crossref
|
|
|
|
|
Rodelo JR, Rosa GDL, Valencia ML (2012). D-dimer is a significant prognostic factor in patients with suspected infection and sepsis. American Journal of Emergency Medicine 30(9):1991-1999.
Crossref
|
|
|
|
|
Singer M, Reutschman CS, Seymour CW (2016). The Third International Consensus Definitions for Septic Shoch (Sepsis-3.0). Journal of the American Medical Association 315(8):801-810.
|
|
|
|
|
Skogberg K, Lyytikainen O, Ollgren J (2012). Population-based burden of bloodstream infections in Finland. Clinical Microbiology and Infection 18:170-176.
Crossref
|
|
|
|
|
Su LX, Feng L, Song Q (2013). Diagnostic value of dynamics serum sCD163, sTREM-1, PCT, and CRP in differentiating sepsis, severity assessment, and prognostic prediction. Mediators of Inflammation 2013:969-875.
Crossref
|
|
|
|
|
Sugiyama M, Atomi Y (1997). Treatment of acute cholangitis due to choledocholithiasisin elderly and younger patient. Archives of Surgery 132(10):1129.
Crossref
|
|
|
|
|
Wilson J, Elgohari S, Livermore DM (2011). Trends among pathogens reported as causing bacteraemia in England 2004-2008. Clinical Microbiology and Infection 17:451-458.
Crossref
|
|
|
|
|
Yan HP, Lu XL, Qiu J (2016). Value of blood lactic acid in evaluating disease severity and prognosis in children with sepsis. Zhongguo Dang Dai Er Ke Za Zhi 18(6):506-510.
|
|