ABSTRACT
Blastocystis hominis is an unusual enteric protozoan of human and animals. Natural products are not only the basis for traditional or ethnic medicine, but also provides highly successful new regimen for human welfare. Meronidazole constitutes a mainstay and is also traditionally considered first line therapy for treatment of Blastocystosis. However, the therapy is complicated due to different dosages and regimens adopted and the unresponsiveness to all treatment. A lot of interest has been generated on the role of probiotic, coconut oil and its fatty acid (Lauric acid) on eradication of the parasite. This study, appraised the effect of monolaurine, lactoferine and metronidazole using different dose regimens on experimental Blastocystosis. Assessment of evaluation was performed by determining the number of oocysts/gm stool, number of vegetative forms and histopathological changes in the intestine, in addition to in vitro susceptibility and ultrastructural changes of B. hominis following incubation with the previous agents. Each hamster was infected orally by 10.000 oocysts. Three weeks later, animals were divided into 6 groups, a control group and five other groups according to the drug they received. Drugs were taken for 5 consecutive days. Two weeks later, scarification of animals was performed and occyst/gm stool and trophozoites in the intestine were counted. In vitro incubation of the parasite with Lactoferine (1000 and 2000 µg/ml), metronidazole (120 and 200 µg/ml) was counted at different time periods (1/2, 1 and 2 h). Parasite viability was assessed using eosin-brilliant cresyle blue exclusion test. Ultrastructural changes of B. hominis following incubation of drugs were studied using transmission electron microscope. This study adds to the fact that natural products can offer an alternative therapy to be used in place of or concurrently with conventional antimicrobials.
Key words: Blastocystis hominis, lactoferine, monolaurin, metronidazole transmission electron microscope, in vitro cultivation, histopathology.
Blastocystis hominis is a unicellular, genetically diverse protest, phylogenetically placed within the stramenopiles (Scanlan, 2012). It is the only member of this group associated with human pathological changes (Tan, 2008;
Tan et al., 2010). It has a worldwide distribution, and is considered the most commonly isolated organism (0.8 to 61.8%) in parasitological surveys (Jenkins et al., 2005). B. hominis is a species complex comprising 17 subtypes (STs) at least 9 of which are found in humans (Poirier et al., 2012; Alfellani et al., 2013). The prevalence of this parasite is usually higher in developing countries, ranging from 30 to 50%, in developing countries and 1.5 to 15% in developed countries (Tan, 2008; Kulik et al., 2008). However, some selected populations in developed countries may have much higher prevalence (Parkar et al., 2007). It is frequently reported in human fecal samples from symptomatic patients as well as healthy individuals. The parasite induces enteritis, manifested in mucous and watery diarrhea, bloating, abdominal pain and/or vomiting (Tan et al., 2010). Clinical studies also associate Blastocystis with other intestinal and dermatological inflammatory disorders, such as irritable bowel syndrome and urticaria, respectively. Patients immune compromised due to the human immunodeficiency virus (HIV) or cancer are particularly susceptible to infections, suggesting that Blastocystis is also an opportunistic pathogen (Kumiawan et al., 2009; Tasova et al., 2000).
Medicinal plants have been used commonly in developing countries due to their availability, inexpensiveness and traditional use for centuries. Due to the controversy surrounding the potential pathogenicity of Blastocystis and the self-limiting nature of symptoms, the treatment of this disease is equivocal. Metronidazole is the most frequently prescribed antibiotic for infections (Mirza and Tan, 2012). Nitazoxanide, a broad-spectrum 5-nitrothiazole antiparasitic agent has also been reported to be effective in treatment (Diaz et al., 2003; Rossignol et al., 2005). A case study in Australia of 18 patients showed that clearance of Blastocystis and symptoms did not occur after treatment with either metronidazole, iodoquinol or triple combination therapy consisting of nitazoxanide, furazolidone and secnidazole showing the lack of efficacy of several commonly used antimicrobials for the treatment of Blastocystis (Sekar and Shanthe, 2013).
Treatment should be considered if there are chronic symptoms of diarrhea and abdominal pain in the absence of other pathogens identified from the stool sample. Metronidazole should not necessarily be considered first line treatment due to the large number of cases of treatment failure. There may be a correlation between subtypes and sensitivity to drugs which is yet to be addressed in studies (Kelesidis and Pothoulakis, 2012). Several clinical trials and experimental studies strongly suggest a place for probiotics as a biotherapeutic agent for the prevention and treatment of several gastrointestinal diseases. Probiotics mediates responses resembling the protective effects of the normal healthy gut flora. The multiple mechanisms of action of probiotics and its properties may explain its efficacy and beneficial effects in acute and chronic gastrointestinal diseases that have been confirmed by clinical trials (Kelesidis and Pothoulakis, 2012).
Lactobacillus seems to have a beneficial effect in amebiasis, giardiasis and infection with Blastocystis hominis. A lot of interest has also been generated on the role of probiotics particularly Saccharomyces boularrdii and other natural food compounds on eradication of the parasite (Choi et al., 2011). Much of the recent research done on coconut oil and lauric acid, the most predominant fatty acid chain found in coconut oil, has centered around the antimicrobial and anti-viral properties of this unique fatty acid. When lauric acid is consumed in the diet, lauric acid forms a monoglyceride called monolaurin, which has been shown to destroy several bacteria and viruses, including listeria monocytogenes and Helicobacter pylori, and protozoa such as Giardia lamblia.
This study highlights the need to reevaluate established treatment for Blastocystis infection and offers clear view treatment options for Metronidazole failures.
This study was carried out in the Parasitology, Pathology and Electron Microscopic Departments in Theodor Bilharz Research Institute (TBRI). All experimental animal studies were managed in accordance with the international guidelines.
Experimental animals
In-vivo studies were carried out in both parasitology and pathology departments. Thirty laboratory bred Syrian hamsters (Mesocricetus ausates) weighing 100 to 110 gms, were provided by the schistosome Biological Supply Program in TBRI.
Experimental design
Out of these 30 hamsters, 5 served as infected non-treated control. Five hamsters received metronidazole (200 µg/ml). Five hamsters received lausic acid (2000 µg/ml). Five hamsters received monolaurine (2000 µg/ml). Five hamsters received 1/3 dose of metronidazole + 2/3 dose of monolaurine, and finally the last group received 1/3 dose metronidazole 2/3 dose of lactobacillus. All groups except the first group received the above mentioned drugs for 5 consecutive days.
Parasites
Fresh stool samples were obtained from patients attending parasitology lab. in outpatient clinic of TBRI. Stool samples were examined by wet smear (Melvin, 1974), MIFC technique (Melvin and Brooke, 1974) and Giemsa stain, (Blagg et al., 1955).
Infection
Stool samples were repeatedly sieved and washed using normal saline. Each animal was infected by 10,000 Blastocystis oocyst orally. Three weeks following infection, treatment was given.
Drugs
(i) etronidazole: A standard drug supplied by Rhone Poulenc Rorer given in a dose of 200 µg/ml.
(ii) Monolaurine: A food supplement manulactured by Ecological formulas (Med. Chemical lab. Denmark, suspended in 10% DMSO. (Dose, 2000 µg/ml).
(iii) Lactobacillus acidophillus: Obtained from Egyptian Ministry of Health and Population License no. 23922 RAMEDA Axcan Pharma (Dose 2000 µg/ml). Two weeks following treatment, sacrification of animals was performed and oocysts/gram stools and trophozoites in the intestine were counted.
In-vitro study was carried out in the Parasitology and Electron Microscopic Departments in TBRI.
Parasites
Fresh stool samples were obtained from patients attending parasitology laboratory in outpatient clinic of TBRI. Stool samples were examined by wet smear (Zierdt, 1991), merthiolate Iodine formaldehyde concentration (MIFC) technique (Zierdt et al., 1988) and giemsa stain (Tan, 2008).
Drugs
Concentration of parasite cells/ml of culture was determined after incubation with different concentrations of drugs at different time intervals”. (1/2, 1 and 2 h).
(i) Metronidazole: Supplied by Rhone Poulenc Rorer (concentration: 120 and 200 µg/ml).
(ii) Monolaurine: Manufactured by: Ecological formulas Med. Chemical lab. Denmark (concentration: 1000, 1500 and 2000 µg/ml).
(iii) Lactobacillus acidophillus: Obtained from Egyptian Ministry of Health and population License no. 23922 RAMEDA Axcan Pharma, (concentration: 1000 and 2000 µg/ml).
(iv) 1% Dimethyle Sulphoxide (DMSO), as a Vehicle Solvent.
(v) In-vitro cultivation of stool samples positive for B. hominis: Approx 50 mg of each fecal sample was inoculated into 2 ml of locke medium (Fenoglia et al., 2008), supplemented with 20% horse serum in a screw cap tube. Tubes were incubated at 37°C for 48 h and a drop of cultured sol. was examined under the light microscope at x10 and x40 magnifications. B. hominis vacuolar forms were found in culture specimens were of variable sizes. Culture was regarded as negative, when it was failed to detect B. hominis after 72 h (Grimaud et al., 1980).
(vi) Stool culture was undertaken to exclude bacterial pathogens.
(vii) All tubes of different groups were incubated in a humidified C°2 at 37°C for ascending time intervals (30 min, 1 and 2 h).
(viii) Parasites were counted using a Neuboaer haemocytometer (Weber England) and trophozoite viability was assessed uring Eosin Brilliant cresyl blue stain.
Histopathological examination
Small intestine of all mice groups were fixed in 10% buffered formalin and processed to paraffin blocks. Tissue section were cut 250 µm apart from the proceeding sections. Paraffin section was prepared from each animal and stained with Hx and Eosin for histopathological examination (Zierdt, 1988).
Transmission electron microscopic examination (TEM)
For culture sediment after incubated with different drugs was done as a trial to discuss the mode of action of these drugs. Samples from different groups were fixed in 4% glutaraldehyde in 0.1 sodium cacodylate buffer to be studied by TEM according to Grimaud et al. (1980). TEM examination was performed in electron microscopy laboratory at TBRI, (Rayan et al., 2007).
There was a significant difference between all treated groups and the control group. The vegetative forms/field were as follows: control 48.33, metronidazole (200 mg/ml) 37.33, monolaurine (2000 m/ml): 17.33, lactoferine (2000 g/ml): 16.66, metronidazole 1/3 dose + lactoferine 2/3 dose: 7.33. As for the number of oocyst/gm stool, it was found to be: 216, 150, 100, 25, 37.33, 7.66, respectively. Histopathological examination revealed normal villi with no atrophy or inflammation as well as absence of Blastocystis in the groups receiving metronidazole, monolaurine and their combination, while in the groups receiving lactorferine alone or combined with metronidazole, few B. oocysts still persisted with some foci of inflammation. No viable oocysts were found after 1 h when lactoferine (2000 µg/ml) and monolaurin (2000 µg/ml) were used compared to 15% viability when metronidazole was added (Tables 1 and 2).


Concentration of parasite cell/ml of culture was determined after incubation with different concentration of drugs at different time intervals. The highest concentration of lactoferine (200µg/ml) caused rapid death of the parasite after 1 h. While the highest concentration of monolaurin that caused rapid death was 2000 µg/ml after ½ h. TEM studies of B. hominis cells displayed key morphological features of programmed cell death with shrinkage of cytoplasm with metronidazole (200 µg/ml) and shrinking of cell wall after exposure to 2000 µg/ml lactoferine. Histopathological figures are shown in Figures 1 to 7, electron microscopic figures are shown in Figures 8 to 11
Recent studies have identified potential parasite virulence factors in and host responses to this parasite. Although Metronidazole is the treatment of choice, physicians are often skeptical about prescribing antibiotics for Blastocystis infections due to frequent reports of non-responsiveness to chemotherapy. Strain-to-strain variation within Blastocystis in susceptibility to metronidazole and other antiparasitic agents among Blastocystis strains is commonly reported, and has been proposed to be the reason for frequent treatment failures in parasite infections (Tan, 2008; Mirza and Tan, 2012).
However, from an evolutionary standpoint, mutations associated with drug resistance may impair essential biological functions or impose energy demands on the organism, leading to decreased microbial fitness. Its role in human diseases was widely debated in the literature during the last two decades. Numerous recent in-vivo and in-vitro studies, strongly suggest that Blastocystis is a pathogen (John et al., 1997; Boorom et al., 2008). Considering the frequent reports of treatment failure in humans with symptomatic Blastocystis infections, it will be interesting to evaluate the effect of natural products on the pathogenicity and response to treatment alone or combined with metronidazole on experimental blastocystosis (Boorom et al., 2008).
In traditional medicine, leaves, bodies, fruits and seeds of many plant species have long been used as anti-diarrheic agents. As medical agents are relatively expensive and may cause significant side effects in patients, herbal compounds are used commonly by local people. Some of these herbal compounds may have significant potential therapeutic effects against different parasites, and may turn out to be registered drugs for these infections in the future (Travers et al., 2011).
The use of probiotics (live viable microbial organisms) in the treatment of specific diseases has evolved into an extremely valuable option, yet to be optimally used in clinical medicine. Probiotics have been shown to have immunomodulating properties and enhance the mucosal barrier. They can have a significant influence on the treatment and prevention of disease. Over 400 different species of micro-organisms reside in the human gastrointestinal tract (GI).
Lactobacilli are perhaps the most well known of these favorable micro-organisms (Termmathurapoj et al., 2004; Stenzel and Boreham, 1996).
Culture is recommended to be a routine diagnostic procedure in diagnosis of Blastocystis, as it is easy to prepare and increases the size and number of the organism (Amer et al., 2007). Transmission electron microscopy (TEM) assist in confirming the diagnosis if atypical morphological forms of Blastocystis species are noted. However, it is not generally required for routine diagnosis of the organism (Aly et al., 2013).
The present study, showed a high significant difference between control and all treated groups. Best results were observed when metronidazole was combined with either monolaurine or lactobacillus. Vegetative forms in the intestine and oocysts/gm stool were markedly reduced compared to the group receiving metronidazole alone. Promising results were obtained when monolaurine or lactobacillus were given alone, compared to metronidazole. The study results are in accordance with Choi et al. (2011), who found that Saccharomyces boulardii probiotics or metronidazole has potential beneficial effects on B. hominis infection (symptoms and presence of parasites). The percentage of reduction in the number of Blastocystis cysts and trophozoites after treatment with lauric acid may be explained by its immunostimulatory effect through its ability to provoke lymphocyte proliferation and stimulation of T-cells proliferation via regulation of IL-2 production, a lymphokine necessary for T-cells proliferation (Helmy, 2010).
In the present study, the combined administration of metronidazole and lauric acid reported very good evidences of cure when compared to the results obtained following administration of the two drugs separately. This can be explained by a potential synergistic effect as each of the two drugs has a different mechanism of action. Similar results were obtained when lauric acid given alone or combined with metronidazole on experimental giardiasis. Rayan et al. (2007), reported that the antigiardial activity of lauric acid was comparable to that of metronidazole.
In our study, the effect of lactobacillus was evaluated on both vegetative forms and oocyst/gm stool. The effect was more promising when combination with metronidazole was used. These results are in accordance with Amer et al. (2007), who found that the combined therapy resulted in a reduction rate of 99.32 and 98.69% in both cysts and vegetative form of Giardia spp. Histopathological examination of the infected control group revealed profound effect on the structure of the intestinal mucosa. This effect was in the form of villous shortening and atrophy, with infiltration of lamina propria with inflammatory cells. Additionally, B. hominis vegetative forms were detected in the intestinal lumen and in-between the villi.
In the current study, histopathological examination of intestinal sections from the infected groups treated with metronidazole, lauric acid (monolaurine) and lactobacillus, revealed an improvement in the form of normal villi, with mild to no inflammation and absence of Blastocystis at the intestinal surface. These results agree with those of Amer et al.
(2007) and Aly et al. (2013) on their work on experimental giardiasis, who found that treatment with Metronidazole, lauric acid and Lactobacillus revealed an improvement in the form of partial healing of intestinal mucosa mild shortening and thickening of the villi, with few Giardia trophozoites were detected in the lumen. Lauric acid appeared to have a better ameliorating effect on the histopathology of the intestinal wall than Metronidazole.
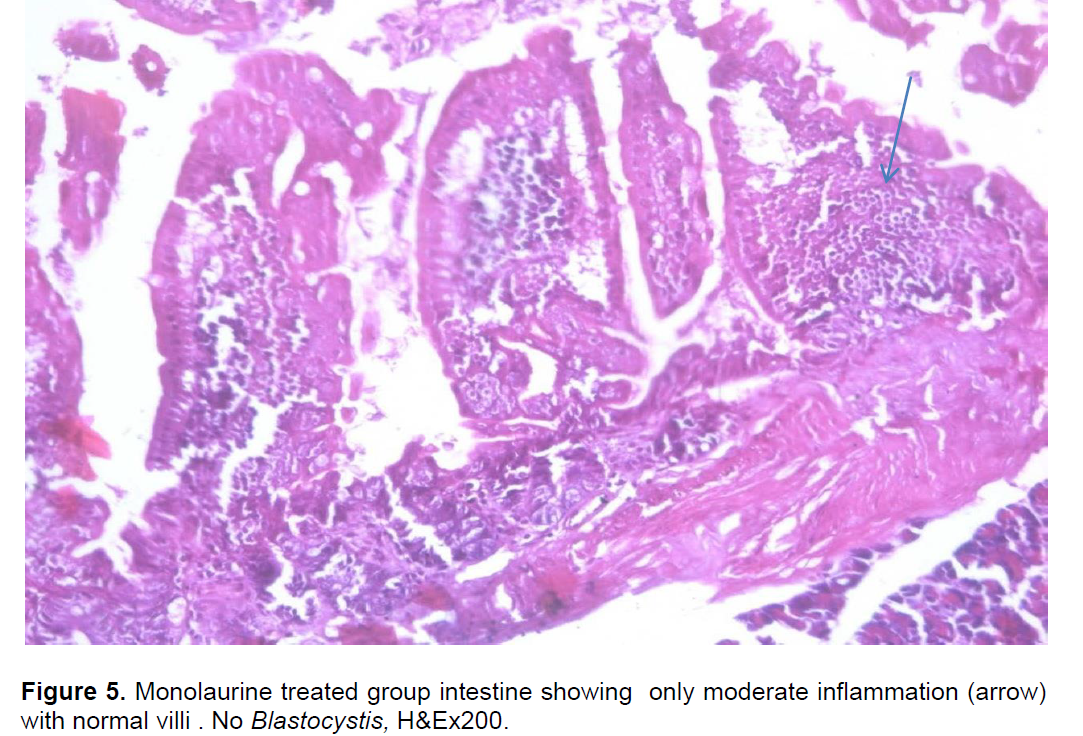
In our study, metronidazole showed normal villi with no inflammation and no Blastocystis. Monolaurine showed only moderate inflammation with normal villi and no blastocystis were detected. On the other hand, lactobacillus alone showed few deformed Blastocystis combined therapy of Metronidazole with either of the twodrugs showed normal intestinal villi, with no Blastocystis. El-Gayar and Soliman (2011), found that Quillaja soponaria showed remarkable improvement of histopathological findings; the mucosa was infiltrated with few inflammatory cells and submucosa was free from inflammation in addition to absence of Blastocystis cells. Lactoferin treated group showed some deformed Blastocystis veg. forms. In agreement with the present results regarding the histopathological changes following Metronidazole treatment, Amer et al. (2007) reported partial healing of intestinal villi after Metronidazole treatment.
In the present study, the effect, lactobacillus and monolaurine was evaluated by the in-vitro growth of B. hominis. Different concentrations of lactobacillus (1000 and 2000 µg/ml) were incubated with B. hominis isolates in culture media at 37°C at different time intervals (1/2, 1 and 2 h). The treatment period at least 1 h was employed as previous standardized studies had shown that this time period is necessary to trigger the cytotoxic response in these parasites (Stenze and Bonham, 1996). At a concentration of 1000 µg/ml and after ½ an hour incubation, lactobacillus showed a reduction in the cells/ml (29.4) compared to 46.5 and 19.5 when metronidazole was called ½ an hour after incubation in this study, lactobacillus at 2000 µg/ml showed highly significant reduction, in the number of concentration of Blastocystis after 1 h incubation after 2 h incubation rapid death of the parasite was detected. The effect of monolaurine on Blastocystis isolates in culture in a concentration of 2000 µg/ml showed 100% reduction in Blastocystis with no viable cells in culture even after incubation for ½ an hour metronidazole is the most frequently prescribed antibiotic (Tan, 2008).
In the present study, the reduction when metronidazole was added to Blastocystis culture in a dose of 120 mg/ml, was 54.9%, while when a dose of 200 mg/ml of the same drug was added to Blastocystis culture after incubation for 2 h, no viable cells were detected. These results are in accordance with Coyle et al. (2012) who, although considering metronidazole being the first line treatment for Blastocystis, stated that the success of eradicating the parasite with this drug has been reported to be anywhere between 0 and 100%. This variation in treatment response suggests the existence of resistant subtypes of the parasite (Mirza and Tan, 2012). The unresponsive patients are perhaps infected with resistant subtypes (Mirza et al., 2011).
Transmission electron microscopic studies are Blastocystis cells displayed key morphological features of shrinkage of the cytoplasm and filamentous layers on the surface with apoptopic changes when Blastocystis cells were treated with metronidazole (Figure 2a) (200 µg/ml), in addition to programmed cell death with apoptopic features (Figure 2b). The result are in accordance with those obtained by Hassan et al. (2010) who observed similar findings. After exposure of B. hominis to lactobacillus 2000 µg/ml, TEM showed shrinkage of cytoplasm and distortion of cell at one pole (Figure 4).
Previous work by Hassan et al. (2010) proved that the in-vitro effects of lauric acid on Blastocystis cells include dose dependent apoptotic changes followed by cell lysis compared to the standard drug, metronidazole.
In summary, a variety of drug treatment option are available for Blastocystis infections. Metronidazole appears to be the most effective and drug for Blastocystis chemotherapy despite some evidence for treatment failure. The development of new therapeutic options to counter antimicrobial resistance requires the use of high through put screening tools. This study shows that natural products (example, monlaurine and lactobacillus), can offer an alternative therapy to be used in place, on concurrently with conventional antimicrobials. Monolaurine and lactobacillus proved to be useful as herbal consolidate for B. hominis therapy. Further studies are recommended on larger number of isolates with relation to clinical manifestations. Molecular typing should be performed to further explain the difference in drug efficacy on different isolates.
The authors have not declared any conflict of interests.
REFERENCES
Alfellani MA, Taner-Mulla D, Jacob AS, Imeede CA, Yoshikawa H, Stensvold CR, Clark CG (2013). Genetic diversity of Blastocystis in livestock and zoo animals. Protist, 164(4):497-509.
Crossref |
|
|
|
Aly MM, Shalaby MA, Artia SS, E-Sayed SH, Mahmoud SS (2013). Therapeutic effect of lauric acid, a medium chain saturated fatty acid. On Giardia lamblia in experimentally infected hamsters. PUJ 6(1):89-98. |
|
|
|
Amer NM, Mahmoud SS, Helmy A, Hammam O (2007). The role of probiotics in controlling Giardia intestinalis in experimental animals. New Egypt J. Med. 37:13-23. |
|
|
|
Blagg W, Schlogel E, Mansour NS, Khaled GJ (1955). A new concentration technique for the demonstration of protozoa and helminth's eggs in faeces. Am. J. Tropical Med. Hygiene 1: 23-28. |
|
|
Boorom KF, Smith H, Nimri L, Viscogliosi E, Spanakos G, Parkar U, Jones MS (2008). Oh my aching gut: Irritable bowel syndrome, Blastocystis, and asymptomatic infection. Parasitol. Vectors 1(1):40.
Crossref |
|
|
Choi CH, Jo SY, Park HJ, Chang SK, Byeon JS, Myung SJ (2011). A randomized, double-blind, placebo-controlled multicenter trial of Saccharomyces boulardii in irritable bowel syndrome: Effect on quality of life. J. Clin. Gastroenterolin Press.
Crossref |
|
|
Coyle CM, Varscehese J, Weiss L, Tanowitz HB (2012). Blastocystis to treat or not to treat. Clin. Infectious Diseases 54(1):105-110.
Crossref |
|
|
|
Diaz E, Mondragon J, Ramirez E, Bernal R (2003). Epidemiology and control of intestinal parasites with nitazoxanide in children in Mexico. Am. J. Tropical Med. Hygiene 68(4):384-385. |
|
|
|
El-Gayar E, Soliman RH (2011). In vitro and in vivo effects of quillaha saponasia on Blastocystis hominis isolates. Parasitol. United J. 4(1):101. |
|
|
|
Fenoglia-Preiser CM, Noftsinger AE, stemmermann GN (2008). Gastrointestinal pathology. An Atlas and Text. 3rd ed. USA: Walters Kluwer, Lippincott Williams and Wilkins P 834. |
|
|
Grimaud JA, Druget M, Peyrol S, Chevalier D (1980). Light and electron microscope study. J. Histochem. Cytol. 28:1145-1151.
Crossref |
|
|
Hassan SI, Moussa HME, Fahmy ZH Mohamed AH (2010). In vitro effect of medium-chain saturated fatty acid (Dodecanoic acid) on Blastocystis Spp. Int. J. Infect Disease 14:584.
Crossref |
|
|
Jenkins B, Holsten S, Bengmark S, Martindale R (2005). Probiotics: A practical review of their role in specific clinical scenarios. Nutr. Clin. Pract. 20(2):262-270.
Crossref |
|
|
|
John A, Catanzaro ND, Green L (1997). Microbial ecology and probictics in human medicine. Altern. Med. Rev. 2(4):296-305. |
|
|
Kelesidis T, Pothoulakis C (2012). Efficacy and safety of the probiotic Saccharmyces boulardii for the prevention and therapy of gastrointestinal disorders. Ther. Adv. Gastroenterol. 5:111-125.
Crossref |
|
|
Kulik RA, Falavigna DL, Nishi L, Araujo SM (2008). Blastocystis sp. and other intestinal parasites in hemodialysis patients. Braz. J. Infect Disease 12:338-341.
Crossref |
|
|
Kumiawan A, Karyadi T, Dwintasari SW, Sari IP, Yunihastuti E, Djauzi S, Smith HV (2009). Intestinal parasitic infections in HIV/AIDS patients presenting with diarrhea in Jakarta, Indonesia. Transactions Royal Society Tropical Med. Hygiene 103: 892-898.
Crossref |
|
|
|
Mirza H, Tan KS (2012). Clinical Aspects of Blastocystis Infections: Advancements amidst controversies. In: Mehlhorn H, Tan KS, Yoshikawa H, editors. Blastocystis: Pathogen or Passenger? Verlag Springer Berlin Heidelberg pp. 65-84. |
|
|
Mirza H, Teo JD, Upcroft J, Tan KS (2011). A rapid, high throughput viability assay for Blastocystis spp. reveals metrenidazole resistance and extensive subtype dependent variations in drug susceptibilities. Antimicrob. Agents Chemother. 55(2):637-648.
Crossref |
|
|
Parkar U, Traub RJ, Kumar S, Mungthin M, Vitali S, Leelayoova S, Thompson RCA (2007). Direct characterization of Blastocystis from faeces by PCR and evidence of zoonotic potential. Parasitology 134(03):359-367.
Crossref |
|
|
Poirier P, Wawrzyniak I, Vivares CP, Delbac F, El Alaoui H (2012). New insights into Blastocystis spp.: A potential link with irritable bowel syndrome. Plos Pathog. 8(3):e1002545.
Crossref |
|
|
|
Rayan H, Ismail OE, Gayar E (2007). Prevalence and clinical features of D. fragilis infection in patients suspected to have intestinal parasitic infection. J. Egypt Soo Parasitol. 37:599-608. |
|
|
Rossignol JF, Kabil SM, Said M, Samir H, Younis AM (2005). Effect of nitazoxanide in persistent diarrhea and enteritis associated with Blastocystis hominis. Clin. Gastroenterol. Hepatol. 3:987-991.
Crossref |
|
|
Scanlan PD (2012). Blastocystis: past pitfalls and future perspectives. Trends Parasitol. 28:327-334.
Crossref |
|
|
Sekar U, Shanthi (2013). Blastocystis: Consensus of treatment and controversies. Tropical Parasitol. 3(1):35-39.
Crossref |
|
|
|
Stenzel DJ, Boreham PF (1996). Blastocystis hominis revisited. Clin. Microbiol. Rev. 9:563-584. |
|
|
Tan KS (2008). New insights on classification, identification, and clinical relevance of Blastocystis spp. Clin. Microbiol. Rev. 21:639-665.
Crossref |
|
|
Tan KS, Mirza H, Teo JD, Wu B, Macary PA (2010). Current views on the clinical relevance of Blastocystis spp. Current infectious disease reports 12:28-35.
Crossref |
|
|
|
Tasova Y, Sahin B, Koltas S, Paydas S (2000). Clinical significance and frequency of Blastocystis hominis in Turkish patients with hematological malignancy. Acta Med. Okayama 54:133-136. |
|
|
Termmathurapoj S, Leelayoova S, Aimpun P, Thathaisong U, Nimmanon T, Taamasri P, Mungthin M (2004). The usefulness of short-term in vitro cultivation for the detection and molecular study of Blastocystis hominis in stool specimens. Parasitol. Res. 93(6):445-447.
Crossref |
|
|
Travers AM, Florent I, Kohl L, Grellier P (2011). Probiotics for the control of parasites: An overview. J. Parasitol. Res. 2011 Article ID 610769.
Crossref |
|
|
Zierdt CH (1988). Blastocystis hominis, a long misunderstood intestinal parasite. Parasitol. Today 4:15-17.
Crossref |
|
|
|
Zierdt CH (1991). Blastocystis hominis-past and future. Clin. Microbiol. Rev. 4(1):61-79. |
|
|
|
Zierdt CH, Donnolley CT, Muller J, Constantapoulos G (1988). Biochemical and ultra structural study of B. hominis. J. Clin. Microbiol. 26(5):965-970. |