Full Length Research Paper

ABSTRACT
Diets and nutrition have critical effect on immune status of human immunodeficiency virus infection and acquired immune deficiency syndrome (HIV/AIDS) patients and on recovery of immune competence after antiretroviral therapy (ART). A pilot study was conducted to explore associations between the dietary pattern of HIV/AIDS patients and their immune (CD4+ cell recovery) response following ART. A recall interview survey of dietary patterns (staple diets and consumption of dairy, other animal proteins, vegetables and fruits) and ART and CD4+ cell count record analysis was conducted on 92 participants visiting the Karamara hospital HIV/ART clinic between February and March, 2015. The staple diet of participants during ART comprised different cereal products and pulse stews. Dairy products, other animal proteins and vegetable/fruit diets were consumed by 88, 46.7 and 40.2% of the participants, respectively. CD4+ count increased more rapidly (p = 0.003) during the first 6 months of ART (144 ± 13.7 cells / mm3) compared to subsequent intervals (74±15.7 to 76.9±20.3 cells / mm3). ART CD4+ counts were consistently higher (p < 0.01) in participants having baseline values > 200 cells / mm3. CD4+ cell recoveries tend to be lower in participants aged > 40 years and in those interrupting ART (p < 0.05). Consumption of camel milk and fermented dairy was associated with relatively higher CD4+ cell recovery after 1 year on ART (p > 0.050). In particular, participants who take soured camel milk demonstrate CD4+ cell counts close to > 500 cell / mm3 after 1 year on ART. Long term CD4+ cell recovery was similarly improved (p = 0.051) in participants consuming fruit/vegetable diets. In contrast, consumption of other animal products had minimal impact on ART CD4+ cell count changes. Fermented or sour camel milk intake could enhance long-term ART immunological response. Deeper, systematic investigation is recommended to verify and establish potential ART-complimenting therapeutic benefits of camel dairy intake in HIV/AIDS patients.
Key words: Antiretroviral therapy (ART), camel, CD4+cell count, diets, HIV/AIDS, pastoralists.
INTRODUCTION
Despite persisting absence of a curative treatment, introduction of effective antiretroviral therapy (ART) has enabled substantial reduction in morbidity and mortality associated with human immunodeficiency virus (HIV) infection worldwide (Palella et al., 1998; WHO, 2006). There are currently over 30 different ARV drugs used in various combinations (Misgena, 2011). CD4 cell count and HIV viral RNA load estimation are key measures for gauging ART response, with former offering a more practical approach in resource poor settings (Hirigo et al., 2015; WHO, 2006). The success of ART in enhancing clinical wellbeing and longevity is predicated on a wide range of factors including; patient characteristics (age, sex, education, income, etc), ART program (accessibility, ARV type, regimen, timing, shifting, etc), CD4+ cell count at initiation of ART, viral load, clinical stage of AIDS, body mass index (BMI), strict adherence and monitoring of ART etc. (Hirigo et al., 2015; Misgena, 2011; Nash et al., 2008; Sieleunou et al., 2008).
Malnutrition constitutes a major contributor to the persistent burden of immune status of human immuno-deficiency virus infection and acquired immune deficiency syndrome (HIV/AIDS) in resource poor settings. AIDS patients who enroll in ART without adequate nutritional support have lower survival rates (Paton et al., 2006). Meanwhile, different diets and nutrients have a direct interaction with ARVs which can alter ART response (Raiten et al., 2005).
Micronutrients play important roles in maintaining immune function and neutralizing the reactive oxygen intermediates produced by activated macrophages and neutrophils in their response to microorganisms. Serum and plasma measurements of vitamins and trace elements, which are imperfect indicators of body stores, have shown that deficiencies are common among HIV infected persons, especially those who are under-privileged, such as women in developing countries, and injection-drug users. Furthermore, micronutrient supple-mentation strategies have shown promising potential in enhancing response to ART (Marston and De Cock, 2004). Adequate protein, energy and micronutrient intake and absorption are essential for achieving the full benefits of antiretroviral therapy (ART) in boosting immune recovery. Moreover, different diets have a direct interaction with antiretroviral drugs (ARVs) which can alter ART response. Enhanced understanding of potential interactions between nutrition and ART is critical for promulgating contextual evidence-based practice guidelines (Raiten et al., 2005).
Camel milk represents an important dietary resource for dry-land pastoralist societies. Moreover, pastoralist communities in Ethiopia traditionally prescribe the product as remedy to a range of human ailments including; gastritis, asthma, abdominal discomfort, HIV/AIDS, liver disease, tuberculosis, fever, urinary problems, common cold, diarrhea, nausea and diabetics (Asresie and Yusuf, 2014). In fact, emerging scientific evidences supports broad antimicrobial and immune modulating activities (Wernery et al., 2012) which could be relevant to traditional indication of camel milk against HIV/AIDS. However, the nutritional and therapeutic values of camel dairy diets for HIV/AIDS patients have not been properly explored. Moreover, research on interactions between nutritional and HIV/AIDS challenges in Ethiopia’s pastoralist areas is still limited.
Therefore, this study attempted to explore potential associations between the dietary trends and immuno-logical response of HIV/AIDS positives undergoing ART at Karamara hospital in eastern Ethiopia. Accordingly, CD4+ cell count variability was tested according to the consumption pattern of different local diets (including camel dairy products) among ART patients.
METHODOLOGY
A pilot study was conducted at the Karamara hospital HIV clinic - in eastern Ethiopia between February and March, 2015. The study adopted a retrospective-exploratory design involving recall interview survey of ART patients and analysis of corresponding clinical records. Recovery of CD4+ cell count (speed and magnitude) and immunological response quality after ART represented dependent study variables. Basic demographic characteristics, ART history and dietary intake patterns of ART patients comprised the major independent study variables.
Study participants were selected from a sampling frame comprising HIV positives having a regular check-up and ART refill schedule at Karamara HIV/ART clinic during the study period. Patients older than 15 years and those with ART duration of 6 months or less were excluded from the sampling frame. A total of 100 potential participants were identified by a random lottery sampling method using the unique clinical ID of ART patients. Subsequently, 8 selected ART patients expressed unwillingness to take part in the study leaving a total of 92 participants.
A simple, structured format was prepared and tested for gathering relevant data pertaining to individual participants. An experienced counseling nurse well-known to the participants was trained on purpose and procedures of the study. On their next visit to the HIV/ART clinic, participants were interviewed by the counseling nurse to give recall account of their dietary intake patterns as summary of average trends for covering their entire ART period. Major parameters addressed included regular staple diets and consumption pattern of other diets including; dairy products (animal source, frequency and type of dairy), other animal proteins, vegetables and fruits. Demographic data, ART history (duration, interruption, etc) and serial CD4+ cell counts (baseline, 6 moth, 1 year and most recent ART intervals) of participant was also registered from clinical records. A total of 7 CD4+cell count records were missing including 2 (1st year) and 5 (recent) ART interval records.
Baseline CD4+ counts were categorized in to three ranges that is, < 100 cells/mm3 (too low), 100 to 200 cells/mm3 (low) and > 200 cells/mm3 (optimum) for comparative analysis against recommended standards. Meanwhile, difference of CD4+ count between successive ART intervals was calculated to analyze speed and magnitude of immunological recovery. According to WHO (2006), ART immunologic failure was determined when CD4+ count falls to below the pre-therapy baseline, or below 50% of the on-peak value, or is persistently < 100 cells/mm.
Statistical analysis
Statistical analysis was conducted using statistical package for social sciences (SPSS-20). Chi-square test was used to evaluate degree of associations between; demographic characteristics, dietary trends, ART history, baseline CD4+ count groups and ART immunological response quality. Independent effect of latter categorical variables on CD4+ count was performed by comparison of means using students‘t’ test and one way ANOVA. Statistical significance was determined at p < 0.05.
RESULTS
The proportion of female participants (60.9%) was higher than (p = 0.037) that of males (39.1%). Meanwhile, fewer (p = 0.000) participants under 20 years (8.7%) were involved as compared to those aged 20 to 40 years (51.1%) or > 40 years (40.2%). The duration of ART was > 3 years, 1 to 3 years and < year for 72.8%, 21.7% and 5.4% participants, respectively (p = 0.000). History of treatment interruption was documented in 6 (6.5%) participants (4 females and 2 male aged > 20 years).
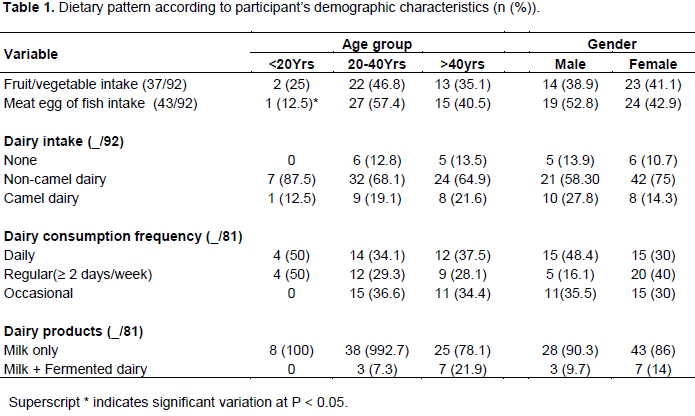
The staple diets comprised of cereal (Teff, Wheat, Rice, Sorghum and/or Maize) products and pulses (Beans and Peas). Majority (p = 0.000) of participants consumed dairy diets > 2 times/ week (59.8%) or at less frequent intervals (28.3%). Dairy products from other animals (68.5%) was consumed more commonly (p = 0.000) than camel dairy (19.6%). All dairy consumers took pasteurized/boiled milk but few (10.9%) also took fermented dairy products including soured camel milk (4.4%). Other animal product (meat, egg or fish) and fruit/vegetable intake was reported by 46.1% and 40.2% participants, respectively. Dairy consumption trend did not vary across age and gender groups. However, intake of meat, egg or fish was higher (p = 0.039) in participants aged > 20 years (Table 1).
A total of 350 CD4+ count records were documented and 7 records were missing for 1st year (2) and recent (5) ART intervals. CD4+ count of participants ranged from 5 to 1592 cells / mm3. Mean CD4+ count (cells / mm3) increased from baseline (192.7 12.9) to the 6 month (336.8 18.3), 1 year (396.5 21.8) and recent (462.4 23.7) ART intervals.
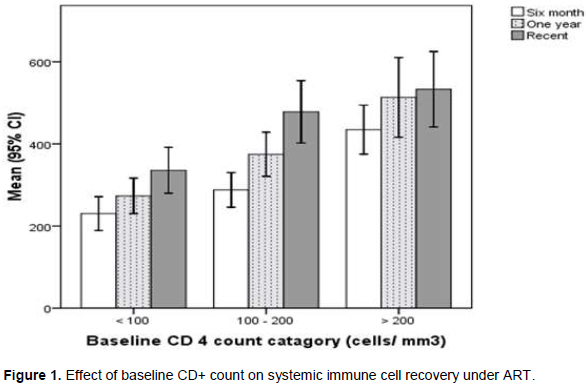
Baseline CD4+ count was too low (< 100 cells / mm3), low (100 to 200 cells / mm3) and optimum (> 200 cells / mm3) in 26.1, 31.5 and 42.4% participants, respectively (p = 0.149). Overall, CD4+ count recovery in 1st 6 months of ART (144 ± 13.7 cells / mm3) was higher (p = 0.003) than changes in the 6 to 12 month (74 ± 15.7 cells / mm3) or 12 month to recent (76.9±20.3 cells / mm3) ART intervals. Optimum baseline CD4+ count was associated with improved immune cell recovery on treatment (Figure 1).
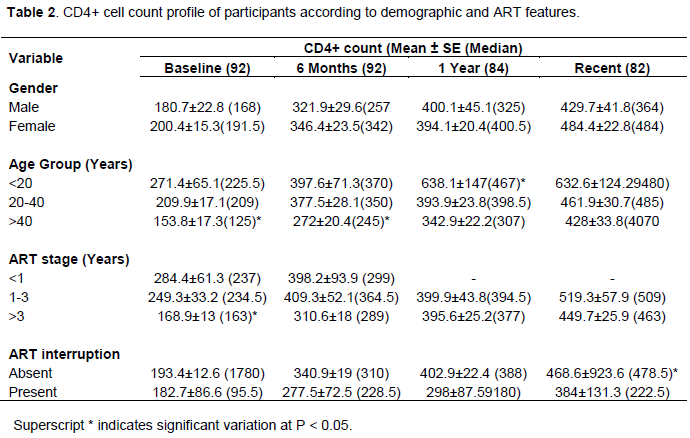
CD4+ counts did not vary significantly between male and female participants. Participants > 40 years had lower baseline (p = 0.012), 6 month ART (p = 0.008) and 1 year ART (p = 0.025) mean CD4+ cell counts. Mean baseline CD4+ count was lower (p = 0.015) in advanced (> 3 years) than recent ART stages. Treatment inter-ruption reduced (p = 0.050) mean CD4+ count on recent (> 1 year) ART interval (Table 2).
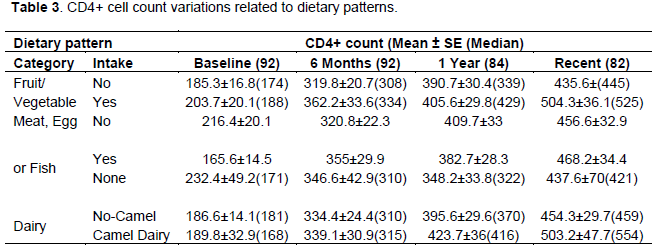
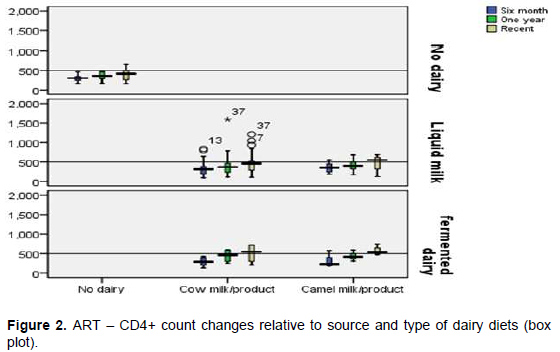
Consumption of non-dairy animal products was associated with lower baseline and higher ART mean CD4+ count, but these variations lacked statistical significance. Intake of fruit/vegetable diets was associated with somewhat higher (p = 0.051) mean CD4+ count on the > 1 year ART interval. Camel dairy consumers demonstrated relatively higher mean CD4+ counts under ART (p > 0.050). Likewise, long term (> 1 year ART interval) immune cell recovery was relatively higher (p > 0.050) among fermented dairy consumers (Table 3). In particular, participants who consumed soured camel milk demonstrate recent (> 1 year) ART interval CD4+ counts close to normal (> 500 cell / mm3) levels (Figure 2).
According to standard world health organization (WHO) definitions, 5 (6.1%) participants had encountered long term (> 1 year) ART immunological failure. Long term ART immunological failure was associated with limited CD4+ count recovery during 1st 6 months of ART and dropping CD4+ counts thereafter. Higher (p = 0.024) treatment failure risk was also noted in participants that interrupted treatment (33.3%) compared to strictly adherent patients (6.6%). None of the participants that reportedly consumed fermented dairy products encountered ART immunological failure (p > 0.050).
DISCUSSION
Higher female ART enrollment was previously noted at same clinic by Damtew et al. (2014). Improving maternal – child health care services could facilitate better HIV detection and treatment in females. Low ART coverage among children (< 15 years) as well as ART non-adherence and follow-up loss are recognized challenges in Ethiopia (HAPCO, 2014). Current observation of higher recent (< 3 years) baseline CD4+ count agrees with global trends (Nash et al., 2008). This could reflect impact of the revised integrated HIV/AIDS treatment guideline encouraging ART enrolment at higher CD4+ count cut points (WHO, 2006) which was adopted by Ethiopia in December 2013 (HAPCO,2014).
An important ART target is the recovery of immune competence (CD4+ cell count). This results from enhanced redistribution of reserve cells, recruitment of naïve T cells, and/or suppression of immune activation mediated apoptotic loss (Kaufmann et al., 2005). ART CD4+ recovery generally occurs in two phases, including a rapid increase of cells during the first two months of therapy followed by slower but sustained increment thereafter (Autran et al., 1997). In agreement, this study found significantly higher CD4+ recovery during the first 6 months of ART compared to subsequent intervals. Higher CD4+ recovery during first 6 months of ART was also reported in Ethiopia (Damtew et al., 2014; Alemu and Sebastián, 2010) and sub Saharan Africa (Lawn et al., 2006).
In this study, patients with low (< 100 cells/mm3) baseline CD4+ count were unable to regain a normal cell count (> 500 cells/mm3) after ART. In agreement, Nash et al. (2008) indicated that only patients initiating ART at baseline CD4+ count of > 200 cells / mm3 could be expected to achieve normal immune cell levels (near or above 500 cells/ mm3) and reduced risk of AIDS related morbidity and mortality. The study noted lower baseline, 6 months and one year CD4+ counts in ART patients over 40 years of age. A similar trend was reported in over 50 years ART recipients in southern Ethiopia (Hirigo et al., 2015). Other had implicated such variations to aging related impairment of thymic function (Douek et al., 1998) and changes in CD4+ reconstitution (Stuart et al., 2002). Another current observation involved significantly lowered recent (> 1 year) ART CD4+ count among patients with history of treatment interruption. ART non-adherence was associated to poor control of viral load (Misgena, 2011; Rougemont et al., 2009) which could foster destruction of immune cells.
In this study, intake of fruit/vegetable and non-dairy animal diets was noted in less than half of the participants. Whereas majority of participants did indicate dairy consumption, intake of camel dairy and fermented dairy products was limited. Consumption of camel dairy and fruit/vegetable diets was associated with relatively higher ART CD4+ recovery. Meanwhile, long term (> 1 year) ART CD4+ count was substantially better (>500 cells/ mm3) among participants consuming fermented camel dairy diets. Chronic malnutrition and nutrient deficiencies represent major contributors to elevated early mortality under ART in resource poor settings. Micronutrients (especially Vitamins A, B6 and B12, Iron and Zinc) play crucial roles in maintaining immune function and neutralizing reactive oxygen intermediates produced by activated macrophages and neutrophils in their response to microorganisms (Marston and De Cock, 2004).
Therefore, the high vitamin (C, B1, B12 and A) and mineral (Na, Cl, Ca, Fe, Mg, etc) contents of camel milk (Al-Humaid et al., 2010) could enhance immunity and tissue protection in HIV/AIDS patients. Moreover, antibacterial and virocidal components (including; lysozyme, highly neutralizing immunoglobulins, lactoferin, lactoperoxidase, peptidoglycan recognition protein (PPR), and N-acetyl glucosmainidase (NA Gase)) which abound in camel milk could facilitate control of infections and immune hyper-activation (Yagil, 2004). Generally, the scientific world (Perdigon et al., 1995) and pastoralist communities (Asresie and Yusuf, 2014; Gizachew et al., 2014) have recognized fermented dairy products to be more nutritious and health promoting than fresh milk.
CONCLUSIONS
This study evidenced that consumption of camel milk, fermented dairy and vegetable/fruit diets tend to enhance long term ART immune response. In particular, soured camel milk consumption appears to enhance recovery of normal systemic CD4+ cell levels (>500 cells/ mm3) after > 1 year of ART. Further study is recommended to validate current observations giving better account to all potential confounders as well as in collaborating immunological findings with strong virological and clinical evidences.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The project was conducted through modest funding by Directorate of Research Publication and Technology Transfer – Jigjiga University. The authors are very much indebted to Mr Seid Mohammed Ali (Academic and Research Vice President) for facilitating funding, Karamara hospital directorate and the HIV/ART clinic for their cooperation and supplying necessary information.
REFERENCES
|
Alemu AW, San Sebasti M (2010). Determinants of survival in adult HIV patients on antiretroviral therapy in Oromiyaa, Ethiopia. Glob. Health Action. 28:3. |
|
|
Al-Humaid A, Mousa HM, El-Mergawi RA, Abdel-Salam AM (2010). Chemical composition and antioxidant activity of dates and dates-camel-milk mixtures as a protective meal against lipid peroxidation in rats. Am. J. Food Technol. 5(1):22-30. |
|
|
Asresie A, Yusuf M (2014). Traditional Consumption, Therapeutic Value and Its Derived Dairy Products of Dromedary Camel (Camelus Dromedaries) Milk in Somali Regional State, Eastern Ethiopia: A Review. Glob. J. Anim. Sci. Res. 3(1):240-246. |
|
|
Autran B, Carcelain G, Li TS, Blanc C, Mathez D, Tubiana R (1997). Positive effects of combine antiretroviral therapyon CD4+ T cell homeostasis and function in advanced HIV disease. Science 277:112-116. |
|
|
Damtew B, Mengistie B, Alemayehu T (2014). Survival and determinants of mortality in adult HIV/Aids patients initiating antiretroviral therapy in Somali Region, Eastern Ethiopia. Pan Afr. Med. J. 22(1). |
|
|
Douek DC, McFarland RD, Keiser PH, Gage EA, Massey JM, Haynes BF, Polis MA, Haase AT, Feinberg MB, Sullivan&num JL, Jamieson BD (1998). Changes in thymic function with age and during the treatment of HIV infection. Nature 396(6712):690-695. |
|
|
Gizachew A, Teha J, Birhanu T, Nekemte E (2014). Review on medicinal and nutritional values of camel milk. Nat. Sci. 12:35-40. |
|
|
Hirigo AT, Fenta DA, Bala TB, Bule SG, Gemechu MR (2015). Trends of Immuno-virological Response Among HIVInfected Patients Receiving Highly Active Anti-retroviral Therapy at Hawassa, Southern Ethiopia. Clin. Med. Res. 4(4):104-110. |
|
|
HIV/AIDS Prevention and Control Office (HAPCO) (2014). Country Progress Report on the HIV Response, Federal Democratic Republic of Ethiopia (FDRE), March 2014 Addis Ababa. |
|
|
Kaufmann GR, Furrer H, Ledergerber B, Perrin L, Opravil M, Vernazza P, Cavassini M, Bernasconi E, Rickenbach M, Hirschel B, Battegay M (2005). Characteristics, Determinants, and Clinical Relevance of CD4 T Cell Recovery to< 500 Cells/µL in HIV Type 1, Infected Individuals Receiving Potent Antiretroviral Therapy. Clin. Infect. Dis. 41(3):361-372. |
|
|
Lawn SD, Myer L, Bekker LG, Wood R (2006). CD4 cell count recovery among HIV-infected patients with very advanced immunodeficiency commencing antiretroviral treatment in sub-Saharan Africa. BMC Infect Dis. 6:59. |
|
|
Marston B, De Cock KM (2004). Multivitamins, nutrition, and antiretroviral therapy for HIV disease in Africa. N. Engl. J. Med. 351(1):78-80. |
|
|
Misgena DK (2011). The pattern of immunologic and virologic responses to Highly Active Antiretroviral Treatment (HAART): Does success bring further challenges?. Ethiop. J. Health Dev. 25(1):61-70. |
|
|
Nash D, Katyal M, Brinkhof MW, Keiser O, May M, Hughes R, Dabis F, Wood R, Sprinz E, Schechter M, Egger M (2008). Long-term immunologic response to antiretroviral therapy in low-income countries: Collaborative analysis of prospective studies: The Antiretroviral Therapy in Lower Income Countries (ART-LINC) Collaboration of the International epidemiological Databases to Evaluate AIDS. AIDS 22(17):2291. |
|
|
Palella FJ Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, Aschman DJ, Holmberg SD (1998). Declining Morbidity and Mortality among Patients with Advanced Human Immunodeficiency Virus Infection; HIV Outpatient Study Investigators. New Engl. J. Med. 338(13):853-860. |
|
|
Paton N, Sangeetha S, Earnest A, Bellamy R (2006). The Impact of Malnutrition on Survival and the CD4 Count Response in HIV-Infected Patients Starting Antiretroviral Therapy. HIV Medicine 7:323-30. |
|
|
Perdigon G, Alvarez S, Rachid M, Agüero G, Gobbato N (1995). Immune system stimulation by probiotics. J. Dairy Sci. 78(7):1597-606. |
|
|
Raiten DJ, Grinspoon S, Arpadi S (2005). Nutritional considerations in the use of ART in resource-limited settings. Geneva: World Health Organization Department of Nutrition for Health and Development. 2005. |
|
|
Rougemont M, Stoll BE, Elia N, Ngang P (2009). Antiretroviral treatment adherence and its determinants in Sub-Saharan Africa: a prospective study at Yaounde Central Hospital, Cameroon. AIDS Res. Ther. 6(1):1. |
|
|
Sieleunou I, Souleymanou M, Schornenberger AM, Menten J, Boelaert M (2008). Determinants of Survival in AIDS Patients on Anti-Retroviral Therapy in a Rural Center in the Far-North Province, Cameroon, Tropical Medicine and International Health 14 (1): 36–43. |
|
|
Stuart JC, Hamann D, Borleffs J, Roos M, Miedema F, Boucher C, de Boer R (2002). Reconstitution of naive T cells during antiretroviral treatment of HIV-infected adults is dependent on age. Aids 16(17):2263-2266. |
|
|
Wernery R, Yagil R (2012). Medicinal Properties in Camel Milk for Treatment of 'Epidemic' Diseases Proceedings of the 3rd Conference of the International Society of Camelid Research and Development ISOCARD, Muscat, Sultanate of Oman. |
|
|
World Health Organization (WHO) (2006). Antiretroviral Therapy for HIV infection in Adults and Adolescents: Recommendations for a public health approach 2006 revision. HIV/AIDS Programme: Strengthening health services to fight HIV/AIDS. Geneva: World Health Organization. |
|
|
Yagil R (2004). Camel milk for health. Available at: http://www.camelmilkforhealth.com. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


