Full Length Research Paper

ABSTRACT
Acetazolamide is a carbonic anhydrase inhibitor which is on World Health Organization’s list of essential medicines, a list of most important medications needed in a basic health system. The ocular effects of acetazolamide was studied in 30 normotensive volunteers. Each volunteer received a loading dose of 500 mg at 0700 h followed by a maintenance dose of 250 mg at 1300 and 1800 h, respectively on day one. From day two to day five, the volunteers received 250 mg acetazolamide thrice daily at the established time intervals. Each volunteer served as his or her own control. Ocular effects of the drug were assessed on the following visual functions; pupil diameter, near point of convergence, visual acuity, amplitude of accommodation, accommodation/convergence accommodation ratio and the phoria status. Results showed that the pupil diameter and near point of convergence increased while the amplitude of accommodation and the accommodation/convergence accommodation ratio decreased. The phoria tended towards exophoria. The aggregate effect on the volunteers was convergence insufficiency with the accompanying asthenopic symptoms, transient myopia and photophobia.
Key words: Acetazolamide, asthenopic, symptoms, convergence, insufficiency.
INTRODUCTION
The use of high potent drugs by the public and clinically in the treatment or management of ocular or systemic ailment could affect the visual functions. Among such drug is acetazolamide, a carbonic anhydrase inhibitor (Dutta and Goodsell, 2004), unsubstituted sulphonamide derivative (Rossi, 2013; Tripathi, 2013), and a bicarbonate diuretic (Reiss and Oles, 1996). The drug is used for medical treatment of glaucoma (Ives, 2013), epileptic seizures (Reiss and Oles 1996; Porter and Meldrum, 2013); idiopathic intracranial hypertension (Brayfield, 2014), altitude sickness (Leaf and Goldfarb, 2007), cystinuria (Wikipedia, the free encyclopedia), periodic peristalsis, central sleep apnoea (Aurora et al., 2012), dural ectasia (Brayfield, 2014; SRS, 2006). It has also been used to prevent methotrexate induced kidney damage by alkalinizing the urine, hence facilitating the excretion of methotrexate by increasing its solubility in urine (Shamash et al., 1991; Brayfield, 2014). Acetazolamide is not an immediate cure for acute mountain sickness rather, it facilitates the acclimatization process which in turn helps to relieve symptoms (Muzza et al., 2004; Leaf and Goldfarb the study: 2007; Low et al., 2012).
Acetazolamide has been extremely effective in inhibiting the production of aqueous humor by the ciliary body (Dutta and Goodsell, 2004) and most valuable as preoperative adjunct in the treatment of acute glaucoma as well as secondary glaucoma (PID, 2005; Rossi, 2013). It is on the WHO list of essential medicines that is, a list of the most important medications needed in a basic health system (WHO, 2013). The drug produces its primary pharmacologic effects through reversible, non-competitive binding with the enzyme carbonic anhydrase in the red blood cells. The enzyme catalyses the cellular production of carbonic acid (H2C03) and the formation of hydrogen and bicarbonate ions (H+ and HC03, respectively). Hence the inhibition of carbonic anhydrase activity in the ciliary body is the mechanism responsible for the decreased aqueous formation produced by acetazolamide (Ives, 2013). In the management of raised intraocular pressure, glaucoma or any condition requiring the reduction of intraocular pressure or as a diuretic or in the treatment of epilepsy, etc (Brayfield, 2004) where acetazolamide is used as a sole drug or in combination with other drugs, no attempt has been made to evaluate the effect of this drug on visual functions such as, pupil size (diameter), near point of convergence, amplitude of accommodation, distant and near visual acuity, accommodative-convergence/accommodation ratio, near and distant phoria, etc. The purpose of this study is to bridge the gap and provide the needed information to clinicians and practitioners since the literature is devoid of such information. It will further serve as an advocate in creating such therapeutic awareness.
MATERIALS AND METHODS
Volunteers who are mainly undergraduate students of Abia State University, Uturu, of both sexes, whose ages ranged from 21 to 30 years (mean 23.6 ± 1.6 years) and body weight 58 to 62 kg were used for the study. Informed verbal consent was obtained from these volunteers. They were further subjected to ocular examination by the optometrist and subjects who from history or examination with any of the following conditions were excluded from the study those with ocular diseases requiring treatment, amblyopic subjects
or those with refractive errors of any type, subjects on any types of systemic medication, which might obscure the results, pregnant or lactating women, etc. After the pre-study examination (screening) thirty normal volunteers of either sexes, male: female ratio (50:50) were selected. Each volunteer had an average intraocular pressure, measured with schiotz tonometer of 20.5 ± 0.1 mmHg, and the following visual functions were measured to establish their initial values: pupil diameter, near point of convergence, amplitude of accommodation, visual acuity, etc. Furthermore, each volunteer acted as his or her own control. This study was approved by the University Ethical Committee on such studies.
Measurements
a. The pupil size (pupil diameter, PD) was measured in millimeters using the pupil distance rulers or pupilliometer. Readings were taken at three different positions and the mean calculated.
b. The near point of convergence (NPC) was measured with the subject fixating at the tip of a pencil positioned initially at 10 cm, then adjusted towards the subject until the subject reports diplopia. The distance between the position of doubling and the central plane of the subject was measured with a meter rule in centimeter to give the NPC.
c. The visual acuity (VA) was measured for near and far, respectively using the standard illuminated Snellen optotypes at appropriate measuring distance (0.4 m for near and 6m for far, respectively).
d. The phoria was measured using the phoropter, and for the distant phoria, the subject was asked to fixate at the far Snellen chart placed at 6 m, then a 15 prism diopters base-in was introduced on the right eye while 6 prism diopters base-out was introduced on the left eye. The chart will appear double. The 15 prism diopters base-in was gradually reduced until there was vertical alignment of the chart. The amount of prism diopters obtained was recorded as the phoria value. For near phoria, the procedure was repeated at a distance of 0.4 m.
e. The amplitude of accommodation (AA) was accomplished using the minus lens to the blur method. The amount of lens added to the blur point plus + 2.50 to compensate for the reduced target gave the AA in diopter.
Drug administration
Day 1, 500 mg acetazolamide tablets as loading dose, at 0700 h, thereafter maintenance dose of 250 mg at 1300 h and 1800 h, respectively. From day 2 to day 5, 250 mg acetazolamide was administered to the volunteers thrice daily at established time intervals. There was no restriction to fluid intake. Each volunteer agreed to comply with the research protocol. The general illumination was maximum, which was about 100 foot candles bearing in mind the volunteers comfort. The volunteers were allowed sufficient time for their eyes to adapt to this level of illumination before the following visual functions were measured: Pupil size (diameter) PD, near point of convergence, (NPC), visual acuity, (VA), amplitude of accommodation, (AA), accommodative convergence accommodation ratio, (AC/A) ratio and habitual phoria.
Materials
Acetazolamide tablets (DiamoxR) 250 mg, Lederle Laboratories Division, Cyanamide (Pakistan) Ltd, Karachi. Potable water, Pupillometer for the measurement of the pupil size (diameter) standard illuminated Snellen Optotypes, distant chart and reduced Snellen chart for the measurement of visual acuity, phoropter and its accessories for the measurement of other visual parameters involved in the study, Schiotz tonometer and 0.4% xylocaine.
Statistical analysis
Data were presented in tabular form. Each subject served as his or her own control. Differences between the initial value of each visual function prior to drug administration and the value obtained after administering acetazolamide was regarded as the change in that particular visual function and expressed as mean ± SEM for six readings, or as percentage.
RESULTS
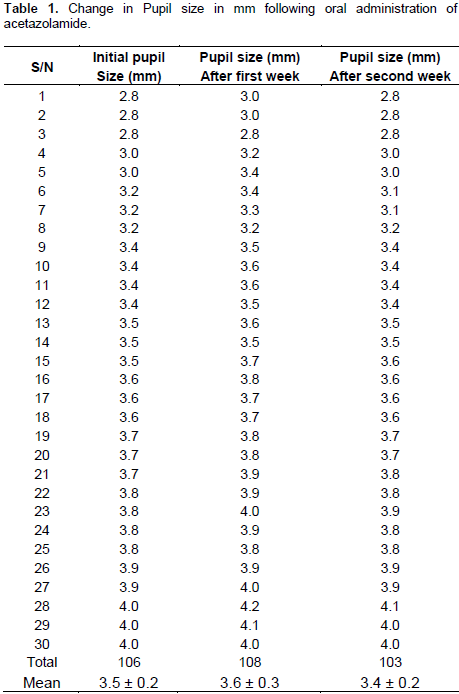
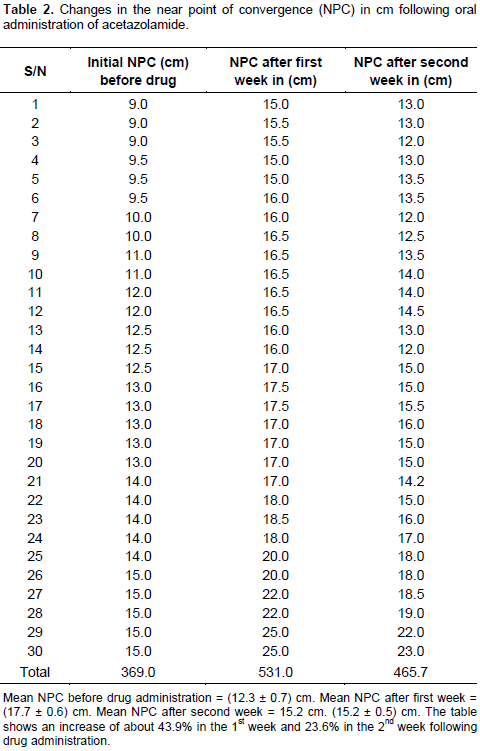
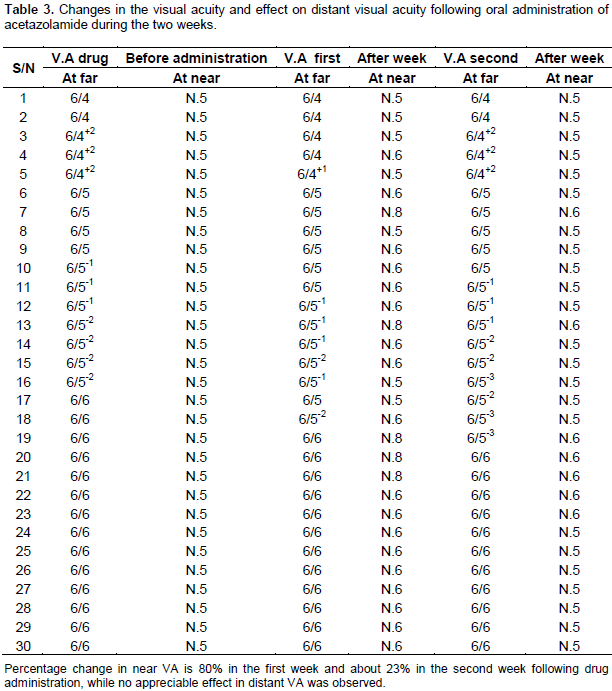
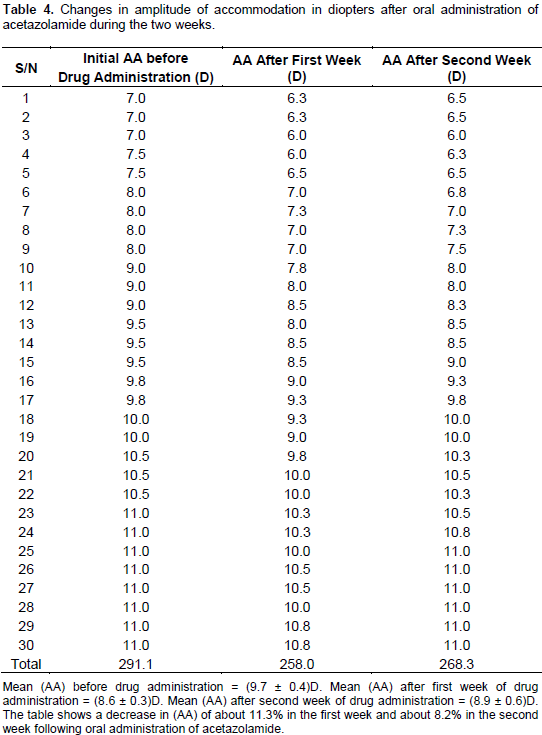
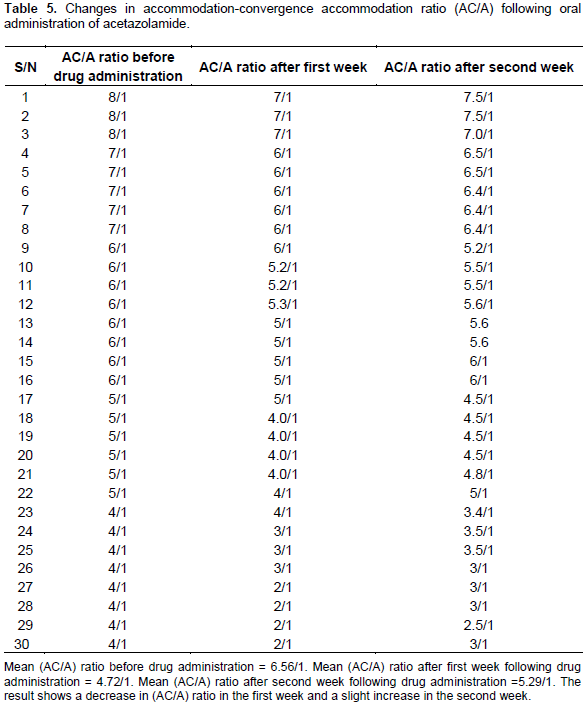
The results of this study are presented in Tables 1 to 6. Table 1 shows the changes in pupil diameter following oral administration of acetazolamide and is indicative of transient mydriasis during the first week and reversal by the second week. Table 2 shows the changes observed in the values of NPC, an increase in the first week (43.9%), a fall in the second week (23.6%) which was still above normal value while Table 3 represents changes in the VA. At near, there was 80% increase in the first week and 23% in the second week and there was no significant change in the distant VA throughout the study. Table 4 shows changes observed in the AA which declined by 11.3% in the first week and 8.2% in the second week while Table 5 shows a similar trend in the AC/A ratio in which the value decreased during the first week and increased slightly by the second week. Table 6 shows that before acetazolamide administration, 73.3, 16.7 and 10% of the study group were esophoric, exophoric and orthophoric, respectively. During the first and second week, the esophoric subjects demonstrated a decline, 50 and 36.7%, respectively while the exophoric and orthophoric subjects increased in the number of subjects (40 and 40%) and (10 and 23.3%), respectively. However, the near phoria was not affected by the acetazolamide administration hence all the subjects remained exophoric at near throughout the study.

DISCUSSION
Acetazolamide a diuretic, is a carbonic anhydrase inhibitor causing the accumulation of carbonic acid, catalyzing the reaction that ultimately leads to reduction in aqueous humour (PID, 2005) and fall in intraocular pressure. There is paucity of information on ocular manifestation of the drug on other visual functions when used thera-peutically. However, during the period of this study which lasted three weeks, some of the subjects complained of mild dizziness (a central effect), and slight discomfort in vision. The PD increased by 3.1% during the first week of drug administration and decreased to 1.1% during the second week, still showing mydriatic effect with a tendency to returning to normal by the end of the study. The transient mydriasis observed in the subjects led to double vision (Table 1). The state of the pupil at any moment is determined by a variety of synergistic and antagonistic nervous influences over the ocular muscles. Generally, external factors such as light and proximity of the fixation point tend to cause constriction while internal factors of sensation and psychic activity cause dilatation (Grosvenor, 1989), and in the present study oral acetazolamide aids the second process of dilatation, hence the transient mydriasis.
The NPC increased following oral administration of acetazolamide during the first and second week of the study, the normal NPC is between 8 and 10 cm as measured from the spectacle plane. If the NPC exceeds 10 cm, there will be problem of convergence insufficiency and in the study the NPC exceeded the range during the first and second week that is, (17.7 ± 0.6) cm and (15.2 ± 0.5) cm, respectively and the subjects would be predisposed to asthenopic symptoms during near work. Asthenopia is the weakness of the eye due to fatigue of the ciliary muscle or the extraocular muscle which is manifested in painful vision. This asthenopia is further aggravated by the mydriatic effect of the drug. During the course of the study, more than 60% of the population complained of tearing, dizziness, ocular discomfort and mild headache which are symptoms of asthenopia. Tearing which was experienced by all the subjects was indicative of diuretic action of acetazolamide.
It is known that when the NPC recedes beyond 10 cm, the individual will have convergence insufficiency. Since there was pupillary dilatation (mydriasis), the depth of focus has been compromised, the image tends to blur faster than normal hence the asthenopia. However, by the second week of the study, the NPC had started to improve, because the pupil had started to constrict.
The changes in near VA occasioned by the mydriatic effect of acetazolamide and the receding NPC shifted the refractive error to transient myopia, the myopia subsided upon discontinuing the acetazolamide therapy (Leaf and Goldfarb, 2007). Furthermore, it is noted that the myopia worsens with low NPC and convergence insufficiency as near work is attempted with the accompanying asthenopic symptoms.
The amplitude of accommodation (AA) represents the maximum amount of accommodation which the eye can exert and it is expressed in diopters. The ability of the eye to effect this is influenced by various factors such as age, previous refractive status of the patient, ciliary muscle balance, drug therapy etc and in the present study and in the first week, the AA dropped by 11.3% following oral acetazolamide administration in concert with the mydriatic effect. This further explains the transient myopia, receded NPC and poor near vision during the first week of the study and tended towards reversal by the second week (8.2%). The study also showed that a change towards exophoria existed from 16.7 to 40% during the first and second week of the study. In a similar manner, the esophoric volunteers declined from 73.3 to 50% and 36.7% in the first and second week, res-pectively. The number of volunteers in the orthoposition increased from 10 to 23.3% in the second week of the study. However, all these subjects demonstrated exophoria at near which exacerbated the asthenopic symptoms if the fusional reserves are not enough (Grosvenor, 1989).
The accommodative-convergence accommodation (AC/A) ratio represents the change in convergence that accompanies a change in accommodation when fusion is interrupted per unit change in accommodation (Bruce et al., 1995; Mutti et al., 2000). It is used for clinical analysis of visual problems and it was found in this study that following oral administration of acetazolamide the AC/A ratio decreased (Table 5) thereby causing convergence insufficiency (Igwe et al., 2015) and the associated visual problems. Table 5 shows that the changes in AC/A ratio were transient as the AC/A ratio increased following cessation of therapy.
It is noteworthy that drug-induced (acetazolamide) myopia and convergence insufficiency contributed to the visual problems of the volunteers, visual discomfort, asthenopic sysmptoms, etc and the unique benefit of this study is that it would enable clinicians gain more knowledge of the ocular pharmacology of such routine essential drug.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Aurora RN, Chowdhuri S, Ramar K, Bista SR, Casey KR, Lamm CJ, Kristo DA, Mallea JM, Rowley JA, Zak RS, Tracy SL (2012). The treatment of central sleep apnea syndromes in adults: practice parameters with an evidence-based literature review and meta-analyses. Sleep 35(1):17-40. |
|
|
Brayfield A (Ed.). (2014). Martindale: The Complete Drug Reference. Preparations, Manufacturers, Pharmaceutical Terms in Various Languages, General Index, Cyrillic Index. |
|
|
Bruce AS, Atchison DA, Bhoda H (1995). Accommodation convergence relationships and age. Invest. Ophthalmol. Vis. Sci. 36:400-403. |
|
|
Dutta S, Goodsell D (2004). Carbonic Anhydrase. |
|
|
Grosvenor TD (1989). Primary Care Optometry. Butterworth Heinemann. A division of Reed Publishing (USA) Inc. 2nd edn pp. 148-168. |
|
|
Igwe SA, Nwbodo N, Ibeawuchi I (2015). The effects of miotics on accommodative-convergence/accommodation ratio of Nigerian youths. World J. Pharmaceut. Sci. 3(4):702-705. |
|
|
Ives HE (2013). Diuretic Agents, In: Basic and Clinical Pharmacology. Katzung BG, Masters SB, Trevor AJ (Eds.). 11th edn McGraw Hill, Lange. International edition. P 456. |
|
|
Leaf DE, Goldfrab DS (2007). Mechanisms of action of acetazolamide in the prophylaxis and treatment of acute mountain sickness. J. Appl. Physiol. 102(4):1312-1322. |
|
|
Low EV, Avery AJ, Gupta V, Schedlbauer A, Grocott MP (2012). Identifying the lowest effective dose of acetazolamide for the prophylaxis of acute mountain sickness: Systemic review and meta-analysis. Br. Med. J. 345:26779. |
|
|
Mutti DO, Jones LA, Moeschberger ML, Zadnik K (2000). AC/A ratio, age and refractive error in children. Invest. Ophthalmol. Vis. Sci. 41:2469-2478. |
|
|
Muzza SR, Fulco CS, Cymerman A (2004). Altitude Acclimatization Guide. Army Research Institute of Experimental Medicine, Thermal and Mountain Medicine Division. Technical Report (USARIEM-TN-04-05). |
|
|
PID (2005). Product Information Diamox ACE. ACETAZOLAMIDE TABLETS. Aspen Pharma Pty Ltd. |
|
|
Porter RJ, Meldrum BS (2013). Antiseizure Drugs. In: Basic and Clinical Pharmacology. Katzung BG, Masters SB, Trevor AJ (Eds.) 11th ed, McGraw Hill, Lange. Int. Edition 416 p. |
|
|
Reiss WG, Oles KS (1996). Acetazolamide in the treatment of seizures. Ann. Pharmacother. 30(5):514-519. |
|
|
Rossi S (2013). Australian Medicines Handbook (2013 ed) Adelaide: The Australian Medicines Handbook Unit Trust. |
|
|
Shamash J, Earl H, Souhami R (1991). Acetazolamide for alkalinisation of urine in patients receiving high dose methotrexate. Cancer Chemother. Pharmacol. 28(2):150-151. |
|
|
SRS (2006). Dural Ectasia in the Marfan Spine: Symptoms and treatment. Scoliosis Research Society. Spine Universe. |
|
|
Tripathi KD (2013). Essentials of Medical Pharmacology, 7th ed. Jay Pee Brothers Medical Publishers, India P 586. |
|
|
World Health Organization (WHO) (2013). The Selection and Use of Essential Medicines: Report of the WHO Expert Committee, 2013 (including the 18th WHO Model List of Essential Medicines and the 4th WHO Model List of Essential Medicines for Children). World Health Organization; 2014 Jul 15. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


