Full Length Research Paper

ABSTRACT
Prescribing errors are common. Available data on these errors, particularly in family community centers in Saudi Arabia, presents a problem that must be addressed. The aim of this study is to investigate the rate and types of prescribing errors at an ambulatory care setting in Riyadh, Saudi Arabia. Data were collected to cover a 12-month period. A prospective review of hand-written prescriptions was made by a trained pharmacist to identify any potential errors therein. The main outcome measure was quantifiable rate and types of prescribing errors. A total of 177,406 prescriptions were scanned wherein 481 (0.27%) prescriptions consisted of at least one error for a total of 510 (0.09%) prescribing errors during the 12-month period of the study. The most common errors were: (1) inappropriate dosage and (2) inappropriate treatment. The uncommon errors consisted of: (1) incorrect drug, (2) incorrect strength, and (3) incorrect duration. All errors were corrected before the prescription reached the corresponding patient. Most errors were made during early morning hours. Lastly, the frequency of errors was highest with prescriptions relating to antidiabetics. Although the rate of prescribing errors in the subject family community center was not frequent, continuous education and monitoring is needed to limit such errors.
Key words: Prescribing error, rate, family community, primary care, Riyadh
INTRODUCTION
According to Dean et al. (2000), “a clinically meaningful prescribing error occurs when, as a result of a prescribing decision or prescription writing process, there is an unintentional significant reduction in the probability of treatment being timely and effective or an increase in the risk of harm when compared with generally accepted practice” (Dean et al., 2000). Prescribing errors in a primary care setting pose significant challenges. Although a prescribing error is considered an avoidable and foreseeable source of harm, it continues to account for 3.7% of hospital admissions (Howard et al., 2007). Previous studies on prescribing errors indicated that these errors were identified in 7.5% of all prescribed items (Shah et al., 2001). Research focused on this issue is, thus, deemed important because of the high number of medications provided during visits to ambulatory centers. A recent systematic review on medication error incidents in the Gulf area included 17 articles on prescribing errors published between 2005 and 2016 (Alsaidan et al., 2018). These papers covered both outpatient and inpatient settings as well as primary care centers. The papers yielded varying results such that the old reports indicated less prescribing errors than the more recent ones. Al Khaja et al. (2005) reported the incidence rate of prescribing errors vis-à-vis the total number of prescriptions at 7%, while Khoja et al. (2011) reported the same ratio albeit at 18% (Al khaja et al., 2005; Khoja et al., 2011). This trend regarding the incidence rate of prescribing errors is not consistent due to the heterogeneity of methods and definitions used throughout the papers. Handwritten prescriptions from outpatient departments were assessed for prescribing errors in 2014, wherein it was showed that 36% of prescriptions contained errors related to omitted dose and omitted route of administration (Albarrak et al., 2014). Moreover, as reported among 46 international studies on medication errors in community care settings, inappropriate prescription was found to be the most common error (Assiri et al., 2018). Severely ill and elderly patients may increase the challenge of prescribing. Prescribing error rates as high as more than 90 and 74% were reported in incidents involving pediatric patients in Bahrain and USA, respectively (Al khaja et al., 2007; Kaushal et al., 2010). A prescribing error rate of 8.3% was also reported in relation to elderly home care patients (Barber et al., 2009). As such, understanding the most common prescribing errors and the factors associated therewith will help formulate an effective strategy to prevent or limit future errors. The main thrust of this study is to detect and analyze the rate and type of prescribing errors at a family community center in Riyadh, Saudi Arabia.
MATERIALS AND METHODS
This study was conducted at a family and community medicine center considered as a primary care facility. It consists of 15 different types of clinics (Table 1) that continuously provide a comprehensive range of professional medical services located in Riyadh, Saudi Arabia. The prescriptions used in this study are all paper-based. The prescriptions were received and processed by the outpatient pharmacy and examined by at least two pharmacists. During this process, if a pharmacist identifies a prescribing error, it is subsequently reported then double checked by a trained or clinical pharmacist. Data were collected from January to December 2018 (12-month period) following the approval from the Institutional Review Board. A prescribing error, in this study, is defined as any error identified in the process of dispensing medications through a prescription that might negatively interfere with the treatment of a patient. The 2001 National Coordinating Council for Medication Error Reporting and Prevention (NCCMERP) standards were utilized for error classification.

A prospective, record-based review of prescriptions for the detection of errors was made. A medication error reporting form was used to document the prescription errors. None of the patients’ identifiable information (names and addresses) on prescriptions was recorded. Medication error reports were initiated by a pharmacist and, subsequently, reviewed by the quality control department according to NCCMERP. The detailed information in the patients’ electronic medical profile relating to their characteristics, demographics, comorbidities, medications, allergies, and their need for monitoring were all reviewed. A communication form was used to specify the type of error. The said form was then attached to the prescription and returned to the prescriber for reevaluation and rectification of the error. The data were uploaded via the MicrosoftÒ ExcelÒ 2017 wherein categorical variables were described using frequencies and percentages, while continuous variables were expressed as means or medians.
Ethical approval
Ethical approval was obtained from the Research Ethics Committee at the Scientific Research Center in Prince Sultan Military Medical City and correspondingly granted the number HP-01-R079.
RESULTS
During the 12-month period of the study, 177,406 prescriptions consisting of 585,499 items were dispensed. Among those, 481 (0.27%) prescriptions were found to have at least one prescribing error for a total of 510 (0.09%) prescribing errors. Only 29 (6%) prescriptions have more than one error. There were 300 (62.4%) prescriptions with errors for females; whereas the rest were for males. The median age of patients presented with prescribing errors was 49 years old. The age range of the population of patients who were presented with prescribing errors was 1 to 86 years old. Approximately 10% of the prescriptions were for pediatric patients.
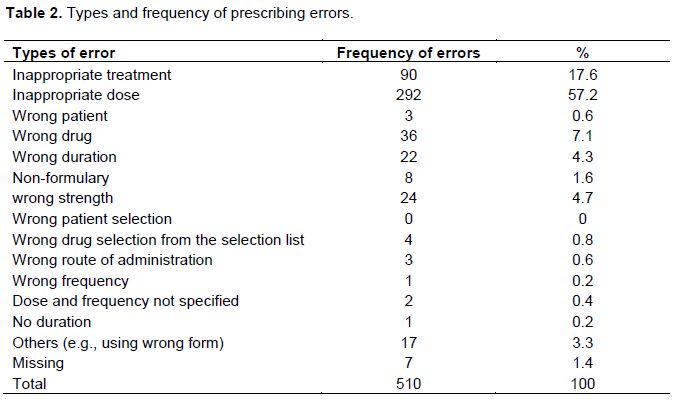
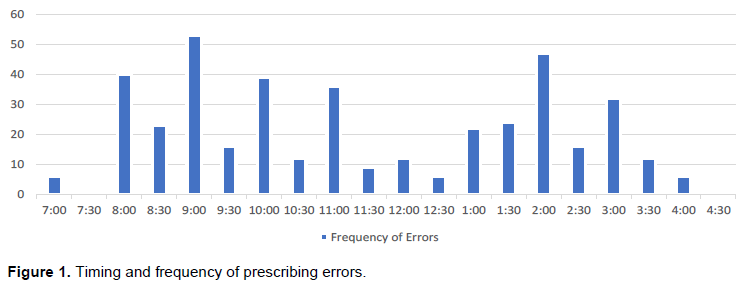
The types of errors and their frequency are summarized in Table 2. It was determined that inappropriate dose was the most frequent error representing 292 (57.2%) of all prescribing errors reported. Inappropriate treatment was reported in 90 (17.6%) cases. Wrong drug was reported in 36 (7.1%) cases, wrong strength was reported in 24 (4.7%) cases and wrong duration was reported in 22 (4.3%) cases. Lastly, the remaining types of errors accounted for less than 4% of overall prescribing errors. Prescribing errors occur most frequently during the early hours of morning and afternoon. The highest frequency of prescribing errors (53) occurred at 09:00 am followed by 47 errors at 14:00 pm (Figure 1). Prescribing errors occurred most frequently with antidiabetics (83) followed by vitamin D3 (69) then cardiovascular drugs (61) (Table 3). The average number of items per prescription was 5.3 from a range of 1 to 16 items.

DISCUSSION
This study identified the incidence of prescribing error in a community family care center. The findings of the study show a low percentage (0.09%) prescribing errors. Moreover, the said errors were of the less harmful type. As such, the findings indicate a well-designed medication prescribing process. Medication prescribing in the subject center is based on standard protocols and guidelines. Its primary strategy to conduct continuous review of all policies and protocols implemented might be the main reason behind the low percentage findings regarding the incidence of prescribing errors. The most common prescribing errors in this study are: (1) inappropriate dose and (2) inappropriate treatment. These findings are consistent with prior studies (Al Juhani et al., 2019; Ferracini et al., 2018; Agrawal, 2009; Lesar et al., 1997). None of the errors detected were presented to patients because these were all rectified by pharmacists immediately through referral to the prescriber.
Unfortunately, an investigation of the reasons behind the prescribing errors was not done in this study. However, it was determined that some of the junior physicians in the subject center were not aware of the protocols and policies in prescribing vitamin D, which might be one of the reasons behind the high frequency of prescribing errors concerning vitamin D prescriptions. The foregoing reason was previously reported by Ross et al. (2012). Most of the patients visiting the community center are diabetic or hypertensive or both, in addition to other cardiovascular diseases, which might explain the high frequency of prescribing errors on diabetic and cardiovascular medications (Laatikainen et al., 2020; Safholm et al., 2019). Other reported reasons pertain to prescribers not using current available treatment evidence or available patient information (allergy information, other medications, and other conditions). It was also found that prescribers fail to consider appropriate information in the patient chart and to communicate the prescription appropriately (Ross et al., 2012; Velo and Minuz, 2009). High frequency of prescribing errors during the early morning hours and in the afternoon may be caused by environmental factors such as time pressures, staff shortage, and fatigue. There is no robust evidence connecting long working hours with patient harm directly, however, medication errors have been linked to fatigue and stress (Peterson et al., 1999). Stress is multifactorial and can be caused by several reasons such as interpersonal relationships, prescription volume, walk-in patients, management responsibilities and individual characteristics (Jacobs et al., 2018). Inadequate breaks and lack of staff have also been identified as problematic within the UK community pharmacy sector as an example (Lea et al., 2012).
Age and high number of unique medications per prescription per patient were also reported as contributing factors to prescribing errors (Avery et al., 2013). In this study, more than 50% of the prescriptions consisted of more than 5 items which justifies the occurrence of more than one error in 6% of the prescriptions. It was also determined that handwriting plays an important role in increasing prescription error. Fortunately, the negative effect of this factor was not high in the subject center. Moreover, computerized prescription will be introduced soon in this center as part of the continuing improvements in pharmaceutical and medical services, which is projected to significantly reduce prescribing errors. According to Bizovi et al. (2002), computerized prescriptions are more than three times less likely to contain errors and five times less likely to require pharmacist clarification than handwritten prescriptions.
Identifying the most common errors and the factors associated with these errors will be useful in formulating effective strategies in preventing such errors in the future. An emphasis on good prescription-making skills and increased awareness of such problems in prescriptions is recommended to be included in every induction program for junior prescribers in order to minimize the recurrence of the problem.
This study, however, may be limited by a selection bias, since only one center is involved in the analysis which is not a representative of the majority of primary care centers in the country. Moreover, the prescriber information was not taken into consideration since most of them are family and community medicine specialists and access to the prescriber name was not readily available to the pharmacy section. It is well known that the total incidence of prescribing errors may be higher than that recorded in studies at pharmacies since many errors are either not disclosed or not detected resulting to non-dissemination to the patients (Kuo et al., 2008; Friedman et al., 2007; Gandhi et al., 2005; Shah et al., 2001). Therefore, identification of the causes of prescribing errors should be conducted so that changes can be made in practice.
CONCLUSION
The rate of prescribing errors in a family community care setting is limited, however, continuous monitoring and education is pivotal to limit the errors. The implementation of computerized prescription in the future will significantly lessen the occurrence of such errors.
FUNDING
This research project was supported by a grant from the Research Centre of the Female Scientific and Medical Colleges, Deanship of Scientific Research, King Saud University.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The authors appreciate the Deanship of Scientific Research and RSSU at King Saud University for their technical support.
REFERENCES
|
Agrawal A (2009). Medication errors: Prevention using information technology systems. The British Journal of Clinical Pharmacology 67:681-686. |
|
|
Albarrak A, Al Rashidi E, Fatani R (2014) Assessment of legibility and completeness of handwritten and electronic prescriptions. Saudi Pharmaceutical Journal 22:522-527. |
|
|
Al Juhani M, Alhumaid N, Abbas M, Assiri E, Aljuhani M (2019). Description of medication errors in primary healthcare centers in Riyadh, Saudi Arabia. The Pharmacy Innovation 8:276-284. |
|
|
Al Khaja K, Al-Ansari T, Sequeira R, (2005). An evaluation of prescribing errors in primary care in Bahrain. International Journal of Clinical Pharmacology and Therapeutics 43:294-301. |
|
|
Al Khaja KA, Al-Ansari T, Damanhori A, Sequeira R (2007). Evaluation of drug utilization and prescribing errors in infants: A primary care prescription- based study. Health Policy (New York) 81:350-357. |
|
|
Alsaidan J, Portlock J, Aljadhey HS, Sheble NA, Franklin BD (2018). Systematic review of the safety of medication use in inpatient, outpatient and primary care setting in the Gulf Cooperation Council countries. Saudi Pharmaceutical Journal 26:977-1011. |
|
|
Assiri GA, Shebl NA, Mahmoud MA, Aloudah N, Grant E, Aljadhey H, Sheikh A (2018). What is the epidemiology of medication errors, related adverse events and risk factors for errors in adults managed in community care contexts? A Systematic Review of the International Literature. BMJ 8:e019101. |
|
|
Avery AJ, Ghaled M, Barber N, Dean Franklin B, Armstrong SJ (2013). The prevalence and nature of prescribing and monitoring errors in English general practice: A retrospective case note review. The British Journal of General Practice 63:e543-553 |
|
|
Barber ND, Alldred DP, Raynor DK, Dickinson R, Garfield S (2009). Care homes' use of medicines study: Prevalence, causes and potential harm of medication errors in care homes for older people. Quality and Safety in Health Care 18:341-346. |
|
|
Bizovi KE, Beckley BE, McDade MC, Adams AL, Lowe RA (2002). The effect of computer-assisted prescription writing on emergency department prescription error. Academic Emergency Medicine 9:1168-1175. |
|
|
Dean B, Barber N, Schachter M (2000). What is a prescribing error? Quality and Safety in Health Care 9:232-237. |
|
|
Ferracini AC, Rodrigues AT, de Barros AA, Derchain SF, Mazzola PG (2018). Prescribing errors intercepted by pharmacist intervention in care of patients hospitalised with breast and gynaecological cancer at a Brazilian teaching hospital. European Journal of Cancer Care 27:e12767. |
|
|
Friedman SR, Geoghegan NM, Sowers S, Kullkarni RN, Formica JR (2007). Medication errors in the outpatient setting: Classification and root cause analysis. The Archives of Surgery 142:278-283. |
|
|
Gandhi TK, Weungart SN, Seger AC, Borus J, Burdick E (2005). Outpatient prescribing errors and the impact of computerized prescribing. The Journal of General Internal Medicine 20:837-841. |
|
|
Howard R, Avery A, Slavenburg S, Royal S, Pipe G, Lucassen P, Pirmohamed M (2007). Which drugs cause preventable admissions to hospital? A systematic review. The British Journal of Clinical Pharmacology 63:136-147. |
|
|
Jacobs S, Johnson S, Hassell K. (2018). Managing workplace stress in community pharmacy organisations: Lessons from a Review of the Wider Stress Management and Prevention Literature. International Journal of Pharmacy Practice 26(1):28-38. |
|
|
Kaushal R, Goldmann D, Keohane C, Abramson E, Woolf S (2010). Medication errors in paediatric outpatients. Quality and Safety in Health Care 19:e30. |
|
|
Khoja T, Neyaz Y, Qureshi N, Magzoub M (2011). Medication errors in primary care in Riyadh City. Saudi Arabia. The Eastern Mediterranean Health 17:156-159. |
|
|
Kuo GM, Philips RL, Graham D, Hickner JM (2008). Medication errors reported by US family physicians and their office staff. Quality and Safety in Health Care 17:286-290. |
|
|
Laatikainen O, Sneck S, Turpeinen M (2020). The risks and outcomes resulting from medication errors reported in the Finnish tertiary care units: A cross-sectional retrospective register study. Frontiers in Pharmacology 10:1571. |
|
|
Lea V, Corlett S, Rodgers R (2012). Workload and its impact on community pharmacists' job satisfaction and stress: A review of the literature. International Journal of Pharmacy Practice 20(4):259-271 |
|
|
Lesar TS, Briceland L, Stein DS (1997). Factors related to errors in medication prescribing. The Journal of the American Medical Association 277:312-317. |
|
|
Peterson G, Wu M, Bergin J (1999). Pharmacists' attitudes towards dispensing errors: Their causes and prevention. Journal of Clinical Pharmacy and Therapeutics 24(1):57-71. |
|
|
Ross S, Ryan C, Duncan EM, Francis JJ (2012). Perceived causes of prescribing errors by junior doctors in hospital inpatients: A study from the PROTECT programme. BMJ Quality and Safety 22:97-102. |
|
|
Safholm S, Bondesson A, Modig S (2019). Medication errors in primary health care records: A cross-sectional study in Southern Sweden. BMC Family Practice 20(1):110. |
|
|
Shah SNH, Aslam M, Avery AJ (2001). A survey of prescription errors in general practice. (2001). Pharmaceutical Journal 267:860-862. |
|
|
Velo GP, Minuz P (2009). Medication errors: Prescribing faults and prescription errors. The British Journal of Clinical Pharmacology 67:624-628. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


