Full Length Research Paper

ABSTRACT
Patients with hypertension and diabetes co-morbidity may have medication knowledge and therapy challenges that could impact on patients’ outcomes. The study examines knowledge of medication and therapy among hypertension and Type-2- diabetes mellitus co-morbid patients at a Municipal hospital in Ghana. This study was conducted at the medical outpatient department (OPD) of the Municipal Hospital in Tema (a Harbour City), in the Greater Accra Region of Ghana. This was a prospective study involving 389 patients, who had co-morbid hypertension and Type-2-diabetes mellitus visiting an OPD of the hospital, of which 338 patients consented to be part of the study. The patients were interviewed with a semi-structured questionnaire, on the name, purpose, number of medications taken, dose, duration of therapy, mode of administration, and side effects of the medication therapy. Bloom’s cut off was used to assess the overall patients’ knowledge, and chi-square analysis used to test the association between knowledge and other variables. From the study, 29% of the study subjects (n=98) had five medicines prescribed (the highest) and three patients (0.9%) were prescribed nine medicines (the least). Patients had knowledge of the names of medication (n=158, 46.8%), duration of therapy (n=322, 95.3%), route of administration (n=324, 95.9%), purpose of anti-hypertensive (n=254, 75.1%), anti-diabetic therapy (n=251, 74.9%) and common side effects (n=50, 14.8%). Overall, more than half had inadequate knowledge of their medication and therapy (n=187, 55.3%). The hypertensive and diabetic patients did not have adequate knowledge about their medications and therapy. This provides justification for the integration of effective pharmaceutical care interventions to improve patients’ outcomes.
Keywords: Hypertension, Knowledge, Medication, Therapy, Type-2-diabetes mellitus
INTRODUCTION
Chronic non-communicable diseases (NCDs) are among the major causes of morbidity, disability and deaths globally. It has been estimated that deaths due to NCDs may increase globally by 17% in the next 10 years (WHO, 2018). In Africa, though infectious diseases are still predominant, there are reports of high rates of deaths from NCDs as well (that is Double disease burden). In Sub-Saharan Africa, deaths from non-communicable diseases increased from 1.7 million (25%) to 2.7 million (34%) from the year 1990 to 2015 (Juma et al., 2019). There has also been an estimation that there could be 27% increase in deaths by the year 2030, if pragmatic health care measures are not put in place in the Africa region for the management and control of non-communicable diseases (WHO, 2018). Ghana, like many other developing countries, is also experiencing the double burden of infectious diseases and NCDs (Agyei-Mensah and Aikins, 2010). According to Ghana Health Service (GHS) report 2016, increase in the disease burden of NCDs has been documented. Hypertension and diabetes have been increasing progressively in Ghana. The prevalence of hypertension is reported to be in the range of 19 to 48%, whilst that of diabetes is 9% in Ghana (Ghana Health Service, 2017). In a cross-sectional study using data retrieved from a 2014 Ghana demographic and health survey, the overall prevalence of hypertension was 13% (Sanuade et al., 2018). Again, in a systematic review of 624 articles, the overall prevalence of diabetes mellitus among adult Ghanaians was 6.46% (Asamoah-Boaheng et al., 2019). These NCDs are managed mainly with multiple drug therapy dependent on patient characteristics and risk factors such as age, gender, past medical history and social history among others (Alomar, 2014). In co-morbid conditions, it is expected that the level of multiple drug therapy use will be higher. This has a consequential effect of increased adverse effects, food drug interactions, disease drug interactions, drug-drug interaction, and nutraceutical drug interaction. One essential requirement for patients to use their medications in the optimum way is when they have adequate knowledge of their medicine. According to the World Health Organization, patient knowledge of their medicines and therapy are essential for patient care (WHO, 2016). Inadequate knowledge about medication and therapy on the other hand can lead to under dose or over dose of medication, treatment failures, non-adherence, increased hospitalization, increased health care cost and poor health outcomes (Saqib et al., 2019). There are some essential parameters which are used for the evaluation of patient’s knowledge, which includes the name, the dose, the dosing frequency, the duration of therapy and one common side effect of the medicine (Saqib et al., 2019). In Ghana, though there have been studies on patients knowledge on NCDs (Agyei-Baffour et al., 2018; Boima et al., 2015; Marfo and Owusu-Daaku, 2017; Okai et al., 2020) there appears to be paucity of data on co-morbid hypertension and diabetes patients regarding their knowledge about medication and therapy in hospital settings. This study therefore seeks to assess the knowledge of patients with hypertension and type-2-diabetes mellitus at a municipal hospital in Ghana about their medications and therapy.
MATERIALS AND METHODS
Study setting
The study subjects were recruited from the medical outpatient clinic, located at the main outpatient department (OPD) of the Tema Municipal Hospital (TMH). TMH is the largest government funded public health institution in the Tema Metropolitan Area, which is a Harbour City. The catchment area of the hospital includes the Tema Metropolis, satellite towns, and villages around it and beyond. The geographical location, the port and harbour and the commercial nature of the metropolis makes the hospital one of the busiest in the Greater Accra Region of Ghana. TMH which has a bed capacity of about 399 is the major referral point for other clinics and hospital in the metropolis, and the towns and villages around it. It has a medical OPD which runs a clinic for hypertension and diabetic patients.
Study design
This study was a prospective hospital-based study among clients with co-morbid hypertension and Type-2- diabetes mellitus. Three hundred and thirty-eight patients (338) were recruited voluntarily on clinic days from August, 2018 to October, 2018.
Inclusion and exclusion criteria
Patients who had been diagnosed with hypertension and Type -2- diabetes mellitus were enlisted into this study based on the inclusion criteria (that is, ≥18 years, ≥6months hypertension and diabetes and consent to regularly to visit the hospital and be part of the study) and exclusion criteria (that is mental incapacitated clients, pregnancy and patients with other forms of diabetes).
Sampling procedure
A simple random technique was employed in the recruitment of participants (Tripepi et al., 2010). The sampling unit was clients attending the diabetic clinic. This clinic operates three days in a week (Wednesday, Thursday and Friday) and averagely attends to 85 patients on each day. The maximum cycle a patient visits the diabetic clinic is 2 months. This means that there will be eight clinic weeks which will result in 24 clinic days. In order to give each patient an equal chance of being sampled, the number of patients sampled per clinic day was 10. Computer generated random sequence was used to generate 10 coded numbers for each clinic day and the patients to be recruited for this study. The sampling frame was the number of patients that were booked for a clinic day. Every patient was given a unique number on each clinic day. Patients who had been previously sampled were excluded from subsequent sampling using dates for their previous clinic attendance. A total of 36 clinic days were used for the recruitment of clients. In all, 389 patients were recruited but 51 refused consent. This reduced the number of participants to 338.
Data collection methods and tools
A consent form was signed or thumb printed by all prospective participants. Participants who were unable to read, write or sign nominated an independent witness to attest to the consent process. A semi-structured questionnaire was used to collect data on the demographic characteristics (age, religion, sex, marital status, educational background, residence status, employment status and lifestyle characteristic), family history of hypertension and diabetes, the number of years diagnosed with hypertension and the number of years diagnosed with diabetes mellitus, number of medications taken per patient, class of medicines prescribed, non-prescription medicines used, complications of hypertension and diabetes and assessment of patient knowledge (name, dose, dosing frequency, duration of therapy, purpose of hypertension and diabetes medication). Experts on the subject matter reviewed the developed questionnaire to validate the content for comprehensiveness, clarity and readability.
Data analysis
Each completed questionnaire was given an identification number. Prior to data entry and analysis, they were coded and entered into Epi info 7 data base. Data processing was done using Microsoft Excel 2016. Statistical analysis and graphical presentation were performed using the GraphPad Prism 7. Normality of continuous data was assessed with Shapiro Wilk’s test and it was not normally distributed. All continuous data were non-parametric and were presented as median (interquartile ranges). Categorical data were presented as frequency (percentages). Blooms cut off point was used to assess the overall knowledge, patients with a score above 80% had adequate knowledge, whilst patient with scores below 80% had inadequate knowledge. Chi-squared test was used to test significance of associations between knowledge and other variables. A p value less than 0.05 was considered statistically significant.
RESULTS
Socio demographic characteristics
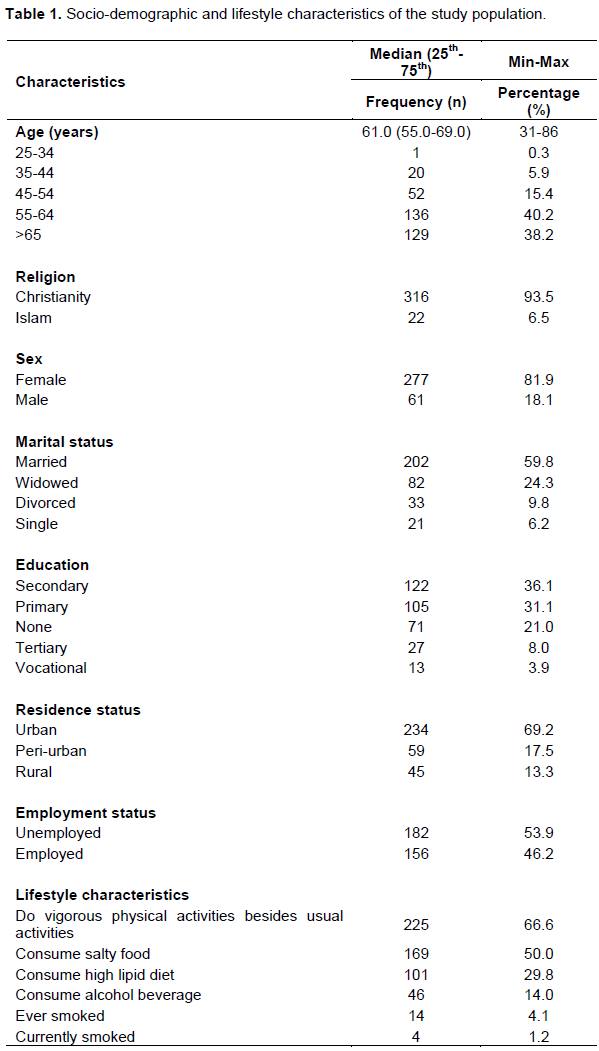
The median age of the patients involved in the study was 61.0 years. Most of the participants (40.2%, n=136) were aged between 55-64 years. A higher proportion of the participants were females (81.9%, n=277), had secondary education (36.1%, n=122), were married (59.8%, n=202), Christians (93.5%, n=316), urban dwellers (69.2%, n=234) and were unemployed (53.9%, n=182). A total of 4 (1.2%, n=4) patients currently smoke, while 14 (4.1%, n=14) had ever smoked. The proportion of the patients who consume alcoholic beverage, salty food and high lipid diet were (14.0%, n=46), (50.0%, n= 169) and (n=101, 29.8%) respectively. A total of 225 participants (66.6%) do vigorous exercise, that is, do 30 min brisk walking at least five times in a week. All but one of the study participants had health insurance (99.7%, n=337) (Table 1).
Clinical characteristics of the study population
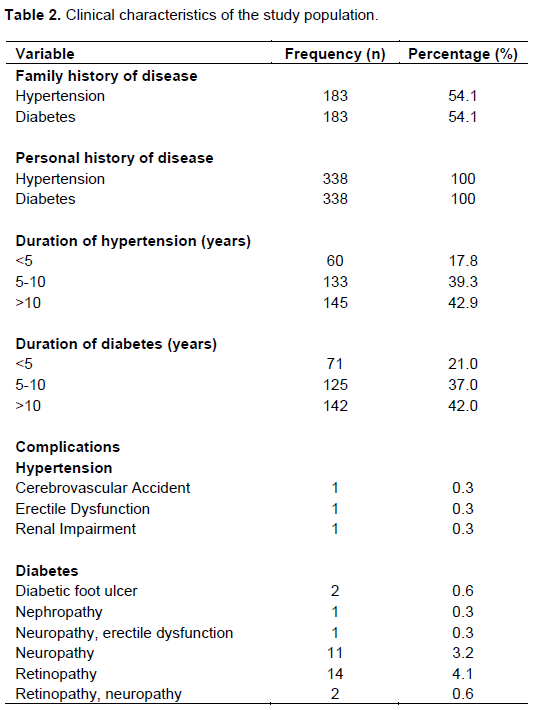
All the patients had hypertension with diabetes as a co-morbidity, with the duration of disease being less than 10 years for hypertension (n=193, 57.1%) and diabetes (n=196, 58.0%). Duration of diseases was more than 10 years for hypertension (n=145, 42.9%) and diabetes (n=142, 42.0%). The most common diabetic complication was diabetic retinopathy (n=14; 4.1%) (Table 2).
The number and class of prescribed medicines used by participants
Seven of the patients (n=7, 2.1%) were on dual therapy, while three hundred and thirty –one (n=331, 97.9%) were on multiple drug therapy. 29% of the study subjects (n=98) had five medicines prescribed (the highest), and three patients (0.9%) were prescribed nine medicines (the least). A total of sixteen classes of medicines were prescribed in 338 prescriptions. Seven (7) were from the anti-hypertensive class of medicines, five (5) were anti-diabetic class medicines and three (3) were other medicines to prevent cardiovascular risk and for the management of complications. The most prescribed class of anti-hypertensive was angiotensin-receptor blocker (n=234, 69%), the most prescribed class anti-diabetic was the biguanide (n=304, 90.74%) and the other classes of medicine prescribed were the anti-platelet, statins and anti-convulsant.
Non-prescription medicines used by participants
A total of four categories of non-prescription medicines were used by patients with diabetes and hypertension. This includes food supplements, herbal preparations, analgesics (non-steroidal anti-inflammatory drugs) and home remedies (bitter leaf of neem, cinnamon and aloe vera) (n=75, 22.2%). The most used non-prescriptive medicine was herbal preparation (n=35, 10.4%) and the least used was home remedies (n= 3, 0.9%).
Results of participant’s response to questions on knowledge on medication
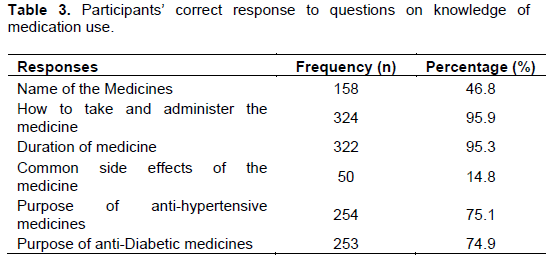
A total of 158 (46.8%) responded correctly to the name of medication, whereas 95.9, 95.3, 14.8%, 75.1 and 74.9% accurately responded to question about how to take and administer the medicine, duration of medicine therapy, side effects of the medicines, purpose of anti-hypertensive medicines and purpose of anti-diabetic medicines respectively (Table 3).
The prevalence of inadequate and adequate knowledge of medication was 55.3 and 44.7%, respectively. Among those classified as having inadequate knowledge; 29.3 and 26.0% had moderate and low level of knowledge based on Bloom’s cut-off points (Figure 1).

Knowledge of medication and demographic characteristics of study participants
There was a significant association between sex (p<0.001), religion (p<0.0001), and educational level (p<0.0001) with knowledge of medication. More males (63.9%) and Christians (47.5%) had high knowledge compared to females and Muslims, respectively. Most of the participants with secondary education (60.7%) had high knowledge of medication used.
Association between knowledge of medication and clinical characteristics
There was a significant association between knowledge of medication and family history of disease, duration of hypertension and diabetes. A higher proportion of the participants with family history of hypertension (n= 97; 53.0%), family history of diabetes (n=93,50.8%) and those with 5-10 years’ duration of hypertension had high knowledge of medication use. Additionally, longer duration of medication (>10 years’=76, 52.4%) was associated with high knowledge of medication use (Table 4).

DISCUSSION
In this study, almost half of the study subjects had knowledge of the names of medication but few (less than 15%) had knowledge of the side effect of their medications. In another study in Turkey, regarding in patients with only hypertension, 64% knew the name of their medicines whiles only 43% knew the side effects (Karaeren et al., 2009). In the area of diabetes mellitus, in a study conducted in Nigeria, 56.9% knew the names of their medicines whilst only 30.6% knew the side effects (Ayodeji et al., 2017). In another study in Lebanon in diabetics, 92.4% knew the name and 17.4% knew a common side effect (Karaoui et al., 2018). This implies majority of patients with non-communicable disease hypertension or diabetes have poor knowledge about the side effects of their medicines, but in co-morbid diabetes and hypertension the situation is worse. The same is observed of the knowledge of the names of their medicines in the isolated condition of hypertension or diabetes as compared to a comorbid condition. Knowing the side effects of medicines reduces anxiety, and also informs the patient and health care workers on when a medicine should be discontinued in case the effects are getting serious. If patients get to know the names of their medicine, it helps them to be part of their own health care and use their medicines in a rational manner and reduces medication errors on the part of the health worker. Pharmacists and other health care personal should effectively counsel patients on their medicines. The World Health Organization and FIP guidelines actively support an active role of pharmacist in assessing patient’s drug history, monitoring of patient, reviewing medications and disseminating information about medicine to patients (FIP and WHO, 2011).
Again, it was observed that almost all but one of the participants was on the National Health Insurance Scheme (NHIS) of Ghana. The Ghana NHIS policy covers the cost of most of the medications of the patient and consultation fee for diagnosis (National Health Insurance Scheme, 2019). This is encouraging. However, the NHIS can further improve the services of patients as part of the NHIS package, by giving remuneration to pharmacist, time for counselling, educating and medication review among others. This can create an enabling environment for the institutionalization of Medication Therapy Review (MTR) and ensuring the effective use of medicines.
Furthermore, most of the participants that had been to school had a higher knowledge of medication than those who had not been to school (p<0.0001). This result shows a positive relationship between formal education and knowledge of education. Thus, there is a need to adopt a comprehensive approach to educate and sensitize patients apart from the knowledge and literacy which comes with learning from formalised schooling. Options should be looked at for sensitizing patients through local languages, self-explainable signs and symbols and other easy to use educational materials.
Additionally, the most used non-prescriptive medicine was herbal preparation (n=35, 10.4%). In a study from Nigeria, 50% of diabetic patients were using herbal medicines (Ezuruike and Prieto, 2016). The use of herbal preparation is becoming widespread, hence there is the need to anticipate drug –herb interaction in other to avoid toxicities. Health care practitioners should probe patients further in order to identify patients on herbal preparations, and the type of herbs used in the preparation so as to make it easy to monitor them for any possible interactions.
Again, this research buttress findings that family history is an essential non-modifiable risk factor for diabetes (n=183, 54.1%) and hypertension (n=183, 54.1%). The genetic factors, shared environment and behaviour linked to these association is well established by many family studies which have demonstrated a linkage of diabetes and hypertension among parents, siblings and children (Barlassina et al., 2002; Geetha et al., 2017); hence, this becomes a useful tool for public health education. Last but not the least, a high proportion of the patients had both conditions for more than 10 years.
STRENGTH OF THE STUDY
To the best of the authors’ knowledge, though studies have been conducted in patient’s medication knowledge in chronic disease in Sub-Saharan Africa, there appears to be paucity of research information in patient knowledge in co-morbid diabetes and hypertension.
LIMITATION OF STUDY
In patient’s recruitment, selection bias was a risk because participation in the study was voluntary. Patients who chose to participate in the study may have been dissimilar in some vital way from those who did not participate; which makes generalization of the study difficult.
CONCLUSION
More than half of the patients assessed had inadequate knowledge about their medication and therapy. Furthermore, the knowledge deficiency was highest regarding the name of medicines being used for therapy and their common side effects. These findings support the justification for the integration of enhanced pharmaceutical care services with emphasis on patient education/counselling about their health, medications and therapy, particularly for patients with co-morbid hypertension and diabetes.
ACKNOWLEDGMENTS
The authors are grateful to the patients, management and staff of the Tema Municipal hospital.
ETHICS APPROVAL
The study proposal was approved by the Committee of Human Research Publications and Ethics (CHRPE) of the Kwame Nkrumah University of Science and Technology (Ethics approval number: CHRPE/AP/409/18).
CONFLICT OF INTERESTS
The authors have not declared any conflict of interest.
REFERENCES
|
Agyei-Baffour P, Tetteh G, Quansah DY, Boateng D (2018). Prevalence and knowledge of hypertension among people living in rural communities in Ghana: a mixed method study. African Health Sciences 18(4):931-941. |
|
|
Agyei-Mensah S, Aikins A (2010). Epidemiological transition and the double burden of disease in Accra, Ghana. Journal of Urban Health 87(5):879-897. |
|
|
Alomar MJ (2014). Factors affecting the development of adverse drug reactions (Review article) Saudi Pharmaceutical Journal 22(2):83-94. |
|
|
Asamoah-Boaheng M, Sarfo-Kantanka O, Boaheng Tuffour A, Eghan B, Mbanya JC (2019). Prevalence and risk factors for diabetes mellitus among adults in Ghana: a systematic review and meta-analysis. International Health 11(2):83-92.11:83-92. |
|
|
Ayodeji AA, Oluseyi Ademola A, Fidelis Olubiyi A (2017). Awareness of Iatrogenic Hypoglycemia Secondary to Anti-Diabetic Agents in Diabetic Nephropathy: A Case Report and Review of Literature. |
|
|
Barlassina C, Lanzani C, Manunta P, Bianchi G (2002). Genetics of Essential Hypertension: From Families to Genes. Journal of the American Society of Nephrology 13(3):S155-S164. |
|
|
Boima V, Ademola A, Odusola A, Agyekum F, Nwafor E, Cole H, Salako B, Ogedegbe G, Tayo O (2015). Factors associated with medication nonadherence among hypertensives in Ghana and Nigeria. International Journal of hypertension 2015. |
|
|
Ezuruike U, Prieto JM (2016). Assessment of potential herb-drug interactions among Nigerian adults with type-2 diabetes. Frontiers in Pharmacology 7:248.. |
|
|
FIP WHO (2011). WHO guidelines on good pharmacy practice: standards for quality of pharmacy services from the WHO technical report series, No. 961. |
|
|
Geetha A, Gopalakrishnan S, Umadevi R (2017). Study on the impact of family history of diabetes among type 2 diabetes mellitus patients in an urban area of Kancheepuram district, Tamil Nadu. International Journal of Community Medicine and Public Health 4(11):4151-4156. |
|
|
Ghana Health Service (2017). Ghana Health Service 2016 annual report. June. |
|
|
Juma K, Juma PA, Mohamed SF, Owuor J, Wanyoike A, Mulabi D, Odinya G, Njeru M, Yonga G (2019). First Africa non-communicable disease research conference 2017: Sharing evidence and identifying research priorities. Journal of Global Health 8(2). |
|
|
Karaeren H, Yoku?o?lu M, Uzun S, Baysan O, Köz C, Kara B, K?r?lmaz A, Naharc? ?, P?nar M, Y?lmaz MB, Uzun M (2009). Original Investigation Özgün Ara?t›rma. In journalagent.com. |
|
|
Karaoui LR, Deeb ME, Nasser L, Hallit S (2018). Knowledge and practice of patients with diabetes mellitus in Lebanon: A cross-sectional study. BMC Public Health 18(1):1-9. |
|
|
Marfo AFA, Owusu-Daaku FT (2017). Exploring the extended role of the community pharmacist in improving blood pressure control among hypertensive patients in a developing setting. Journal of Pharmaceutical Policy and Practice 10(1):1-9. |
|
|
National Health Insurance Scheme, G (2019). NHIS Medicines list . NHIS Ghana. |
|
|
Okai DE, Manu A, Amoah EM, Laar A, Akamah J, Torpey K (2020). Patient-level factors influencing hypertension control in adults in Accra, Ghana. BMC Cardiovascular Disorders 20(1):123. |
|
|
Sanuade OA, Boatemaa S, Kushitor MK (2018). Hypertension prevalence, awareness, treatment and control in Ghanaian population: Evidence from the Ghana Demographic and Health Survey PloS One 13(11):e0205985. |
|
|
Saqib A, Atif M, Ikram R, Riaz F, Abubakar M, Scahill S (2019). Factors affecting patients' knowledge about dispensed medicines: A Qualitative study of healthcare professionals and patients in Pakistan. PloS ONE 13(6). |
|
|
Tripepi G, Jager KJ, Dekker FW, Zoccali C (2010). Selection Bias and Information Bias in Clinical Research. Nephron Clinical Practice 115(2):c94-c99. |
|
|
World Health Organization (WHO) (2016). Medication Errors Technical Series on Safer Primary Care Medication Errors: Technical Series on Safer Primary Care. |
|
|
World Health Organization (WHO) (2018). Noncommunicable diseases country profiles 2018. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


