Full Length Research Paper

ABSTRACT
Myocardial infarction causes an acute condition of necrosis of the myocardium resulting in increased production of free radicals and decreased levels of antioxidants. It was proposed that Febuxostat reduced myocardial oxidative stress and suppressed apoptosis. Cilostazol used to treat claudication has a growing evidence, suggesting that Cilostazol could be cardioprotective. This work aims to highlight the potential protective effect of pretreatment with Febuxostat vs. Cilostazol on Isoproterenol induced cardiac toxicity in rats. Thirty-six male albino rats were divided into 6 groups (6 rats each); control, Febuxostat, Cilostazol, Isoproterenol, Febuxostat+Isoproterenol and Cilostazol+Isoproterenol groups. Cardiotoxicity was induced by subcutaneous injection of Isoproterenol 100 mg ̸ kg on the 13th and14th day of the experiment. ECG parameters were assayed. Measurement of cardiac TNF-α level, serum troponin and histopathological changes were also performed. Pretreatment with Febuxostat led to significant increase in heart rate and a significant decrease in QT and QTC intervals compared to Cilostazol. Cilostazol led to significant reduction in TNF-α and insignificant reduction of cardiac troponin levels compared to Febuxostat. Isoproterenol led to arrhythmia in 33% of rats, Febuxostat led to arrhythmia in 50% of rats, while Cilostazol did not lead to any arrhythmias. Pretreatment with Febuxostat and Cilostazol led to significant improvement in the pathological changes caused by Isoproterenol; however, there was no statistically significant difference between them. Pretreatment with Cilostazol is more cardioprotective than Febuxostat as it led to more reduction in TNF-α without increasing arrhythmias or affecting QT and QTC intervals as compared to Febuxostat.
Key words: Cardioprotective, cilostazol, febuxostat, isopreterenol, cardiac dysfunction.
INTRODUCTION
Myocardial infarction is a state of acute myocardial necrosis that results in increased production of free radicals and decreased antioxidants levels. Oxidative stress leads to generation of toxic reactive oxygenspecies such as superoxide radical, hydrogen peroxide and hydroxyl radical that results in myocardial cells damage (Badore et al., 2017).
Many experimental models were proposed to study the possible protective effects of drugs on myocardial injury. The widely used drug to induce myocardial injury is the Isoproterenol model, since it causes damage similar to the one that occurs in acute myocardial infarction in humans. Several mechanisms were proposed to explain the Isoproterenol-induced myocardial damage. First, the oxygen supply/demand is imbalance due to increased chronotropic and inotropic actions as well as hypotension in the coronary circulation. Second, the elevation of Ca++ overcharges inside the cell which is related to the activation of the adenylate cyclase enzyme and adenosine triphosphate (ATP) depletion. Eventually, the oxidative stress augmentation that is generated because of several metabolic products originated from Isoproterenol (Filho et al., 2011).
Febuxostat is a non-purine selective inhibitor of xanthine oxidase. Xanthine oxidase is a major source of reactive oxygen species during myocardial ischemia. Evidence suggests that Febuxostat has an antioxidant effects by direct reactive oxygen species scavenging. Febuxostat has been shown to have beneficial effects in renal ischemia reperfusion injury, suggesting that it suppresses apoptosis and reduces oxidative stress (Wang et al., 2015).
Cilostazol is a selective type-III phosphodiesterase inhibitor that is widely used in treatment of claudication; there is a growing evidence that it could be cardioprotective as it inhibits not only type III phosphodiesterase enzyme, but also adenosine uptake, thus reducing the cAMP levels. Some studies suggested that it can also prevent fatal arrhythmias in Brugada syndrome. It can also prevent H2O2-induced cardiac mitochondrial dysfunction by attenuating mitochondrial swelling, preventing mitochondrial depolarization, and reducing reactive oxygen species production (Siriporn et al., 2014).
The aim of this study is to highlight the potential protective effect of pretreatment with Febuxostat vs. Cilostazol on Isoproterenol induced cardiac toxicity in rats.
MATERIALS AND METHODS
Experimental animals
Thirty-six adult male albino rats of Wistar strain weighting (200 ± 20) g were used. The animals were handled according to the guidelines of local ethical committee which complies with the international laws for use and care of laboratory animals. All rats were kept under observation for at least one week prior to study with free access to food, water, and in separate cages. They were fed with a standard laboratory diet composed of 20% proteins, 9% fats, 14% fibres, 44% carbohydrates, 22% minerals and 15% vitamins. They were allowed free access to water. Rats were exposed to daily light ̸ dark cycle. Rats were divided into 6 groups (6 rats each): Group 1 (Control group): Rats received 1 ml distilled water orally and SC for 14 days; Group 2 (Febuxostat group): Rats received Febuxostat 10 mg orally for 14 days (Wang et al., 2015) followed by 1 ml distilled water SC on the 13th and 14th days; Group 3 (Cilostazol group): Rats received Cilostazol 5.8 mg/kg orally for 14 days (Dhakad et al., 2017) followed by 1 ml distilled water SC on the13th and 14th day; GROUP 4 (Isoproterenol group): Rats received 1 ml distilled water orally for 14 days followed by Isoproterenol 100 mg/kg SC on the 13th and 14th days (Dhakad et al., 2017); Group 5 (Febuxostat+Isoproterenol group): Rats received Febuxostat 10 mg/kg orally for 14 days followed by Isoproterenol 100 mg/kg SC on the 13th and 14th day; Group 6 (Cilostazol+Isoproterenol group): Rats received Cilostazol 5.8 mg/kg orally for 14 days followed by Isoproterenol 100 mg/kg SC on the 13th and 14th day.
Evaluation of the cardioprotective effects
At the end of the 14th day, ECG was performed then rats were sacrificed by cervical dislocation and hearts were excised for estimation of tumor necrosis factor alpha (TNFα), Cardiac troponin I (cTnI) and for histopathological examination.
Electrocardiogram
This was recorded on rats under light ether anesthesia in the prone position by KENZ (ECG106) device (made by NAGOYA, JAPAN). Standard limb leads were constructed from electrodes placed at the right hand, left hand and the tail. ECG was traced to asses: heart rate, QT and corrected QT (QTc) interval (using Bazett’s formula: QTc (millisecond)=QT(millisecond)/ÖRR(second), and for detection of signs of ischemia (ST segment deviation or T-wave changes) and arrhythmias.
Biomarkers
Calculation of serum cardiac troponin-I (cTnI) and Tumor necrosis factor alpha (TNFα) in cardiac tissue were performed using Elisa kit (Competitive ELISA).
Histopathological examination of cardiac tissue
The hearts were excised, prepared and a serial section of 4 microns thickness was obtained and stained with Hematoxylin and Eosin to assess myocardial histopathological changes. Myocardial injury was assessed by the score that was developed by Filho et al. (2011).
Statistical analysis
Data were collected, coded, double entered and analysed using SPSS software (Version 16) on Windows 7. Mean and S.D. were calculated for quantitative variables in the form of simple descriptive analysis. Categorical data were analyzed by computing percentages, and differences were tested statistically by applying chi square tests for comparisons between groups; p-value of <0.05 was considered statistically significant. Comparison of quantitative normally distributed values between groups was done using ANOVA test; post hoc test (LSD) was performed after ANOVA test for intergroup comparisons. Comparison of scores was performed using Mann-Whitney test. Correlation of quantitative variables was performed using Pearson correlation and expressed using correlation coefficient(r) with its value ranging from -1 to 1 (Table 1).

RESULTS
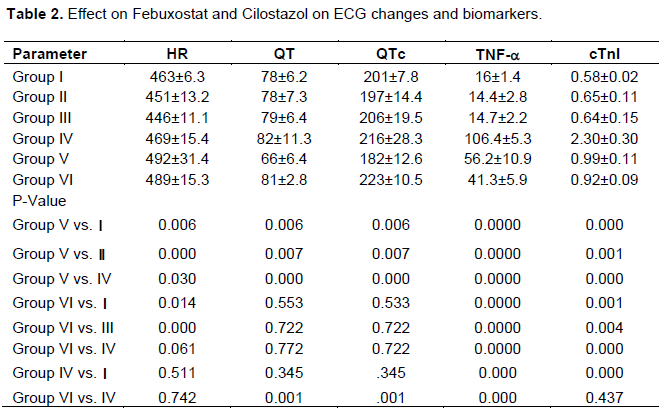
Isoproterenol led to cardiac toxicity that is evident by increase in the heart rate, QT, QTc intervals, and the incidence of arrhythmia compared to control group. It led to significant increase in the TNF-a (106 ± 5.3 vs. 16 ± 1.4 U ̸ mg protein, p value 0.00) and cardiac Troponin I (cTnI) (2.30 ± 0.30 vs. 0.58 ± 0.02 U ̸ mg, p value 0.0000) (Table 2). Regarding the histopathological changes (Table 3; Figures 1 and 2), Isoproterenol led to loss of the normal myocardial architecture, edematous changes (in the form of gapping, disorientation and vacuolations between the muscle fibers), disorganized muscle fibers with marked cellular injury and enlargement in the size of cardiomyocytes, blood vessels were dilated and congested, and inflammation (moderate in 83.3% and marked in 16.7% of rats, p value 0.001) compared to control group. Pre-treatment with Febuxostat showed cardioprotective effect on Isoproterenol induced toxicity. It led to significant decrease in QT and QT intervals compared to Isoproterenol group. However, it led to arrhythmia in 50% of rats compared to 33% of rats in Isoproterenol group. There was significant decrease in the TNF-a (56±10.9 vs. 106±5.3 U/mg, p value 0.000) and cTnI (0.99±0.11 vs. 2.30±0.30 U/mg, p value 0.0000) (Table 2). It also led to improvement of Isoproterenol-induced histopathological changes (Table 3 and Figures 1 to 3). Cardiomyocytes were arranged in interlacing bundles with normal histological pattern. However, few pathological changes were still evident in the form of areas of lost striations, intercellular and intracellular vacuolations, as well as few mononuclear inflammatory cells but congestion was still present. Moreover, there was mild inflammation in 66.7% of rats and moderate inflammation in 33.3% of rats compared to Isoproterenol group (p value 0.002).
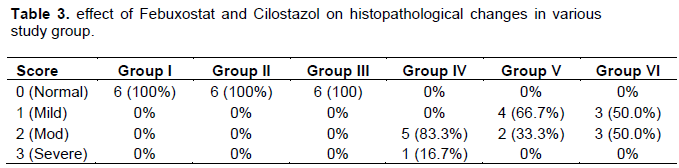



Pre-treatment with Cilostazol showed cardioprotective effect on Isoproterenol induced toxicity without any significant change in heart rate, QT and QTC intervals or arrhythmias when compared to Isoproterenol group. Cilostazol led to significant decrease in the TNF-a (41.3±5.92 vs. 106.4±5.34 U/mg, p value 0.0000) and cTnI (0.92±0.09 vs. 2.30±0.30 U/mg, p value 0.0000) (Table 2). Pre-treatment with Cilostazol led to improvement of Isoproterenol-induced histopathological changes (Table 3, and Figures 1, 2 and 4).
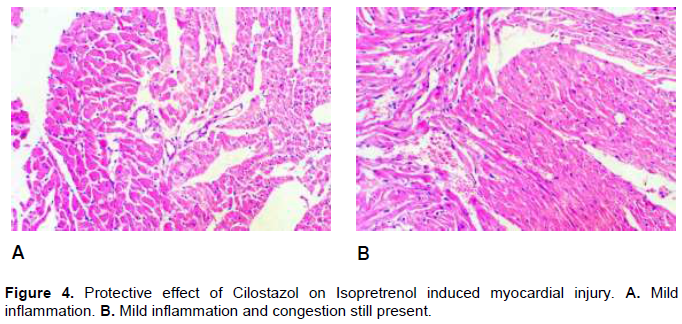
Cardiomyocytes were arranged in interlacing bundles with normal histological pattern. However, few pathological changes were still evident in the form of areas of lost striations, intercellular and intracellular vacuolations, as well as few mononuclear inflammatory cells but congestion was still present. Moreover, Cilostazol led to mild inflammation in 50% of rats and moderate inflammation in 50% of rats.
On comparison between the cardio-protective effect of Febuxostat vs. Cilostazol on Isoproterenol-induced cardiac toxicity, Cilostazol led to significant increase in QTC interval (223.00±10.526 vs. 182.17±12.671 millisecond, p value 0.001) without significant change in heart rate or arrhythmias compared to Febuxostat. Cilostazol led to significant reduction in TNF-a (41.3 ± 5.92 vs. 56.2±10.92 U/mg, p value 0.000) and insignificant reduction in cTnI (0.92±0.09 vs. 0.99±0.11 U/mg, p value 0.437) (Table 2). Both Febuxostat and Cilostazol led to significant improvement of histopathological changes on Isoproterenol treated rats; however, on comparing them to each other, these changes were not statistically significant (Table 3; Figures 2,3 and 4).
DISCUSSION
The present study demonstrated the cardioprotective effect of Febuxostat and Cilostazol on Isoproterenol induced cardiac toxicity in rats.
The mechanism of cardiotoxicity induced by Isoproterenol administration is associated with a decrease in endogenous antioxidants and increase in oxygen-free radicals, resulting in increased oxidative stress. It is reported that plasma levels of these markers are directly proportional to the degree of necrotic lesions present in the myocardium and thus are markers of myocardial damage (Dhakad et al., 2017).
In the present work Isoproterenol administration led to arrhythmia in 33.3% of rats. This was in accordance with Dhakad et al. (2017) who demonstrated that cardiac arrhythmia pattern is observed in Isoproterenol induced cardiac toxicity in Wistar rats. Several mechanisms proposed to explain the Isoproterenol-induced myocardial harm: First of all, an imbalance between oxygen supply to and demand from cardiomyocytes inwardly, which is related to myocardial hyperfunction due to increase in chronotropism and inotropism as well as hypotension in the coronary bed. Secondly, it is also claimed that there is an elevation of Ca++ overcharge inside the cell. In addition, that ion is related to the activation of the adenylate cyclase enzyme and the depletion of ATP levels on the course of the events. Eventually, there is an oxidative stress augmentation because of several metabolic products that originated from Isoproterenol (Filho et al., 2011).
Isoproterenol in the present study produced significant increase in TNF-a compared to control group which is in agreement with Eom et al. (2016) who showed that Isoproterenol enhances TNF-Related apoptosis-in human embryonic kidney cells through death of receptor 5 up- regulation. Deng et al. (2015) who investigated the cardioprotective effects of timosaponin B II from Anemarrhena asphodeloides Bge on Isoproterenol-induced myocardial infarction in rats showed that Isoproterenol administration resulted in significant elevations in the levels of cardiac injury biomarkers CK-MB, LDH, proinflammatory cytokines IL-6, and TNF-α.
Moreover, Isoproterenol produced significant increase in cardiac troponin I (cTnI) compared to control group. This coincides with the results of Parikh (2015) who investigated the cardioprotective effects of Crataegus oxycantha and Triticum aestivum Linn. He demonstrated that there was significant increase in cardiac troponin I (cTnl) and CK-MB in Isoproterenol treated rats. Furthermore, Isoproterenol caused pleomorphic pathological changes including congestion in cardiomyocytes, loss of the normal myocardial architecture and edematous changes. Cardiac muscle fibers were disorganized and marked by cellular injury, enlargement in the size of cardiomyocytes, and a large number of inflammatory cell infiltration. Blood vessels were dilated and congested which coincide with Deng et al. (2015) who revealed that Isoproterenol treated rats exhibited obvious myocardial cell swelling degeneration, transverse striations loss, and increased amount of infiltrating inflammatory cells. Filho et al. (2011) observed that the administration of Isoproterenol caused an increase in leukocyte counts and neutrophils in the Infarcted group, when compared to control group. High counts of leukocytes and neutrophils were observed in rats with Isoproterenol-induced myocardial infarction.
In the present work pretreatment with Febuxostat led to significant decrease in QT and QTc intervals compared to Isoproterenol. It also led to arrhythmia in 50% of rats while Isoproterenol led to arrhythmia in 33% only of rats. To our knowledge this is the first study that demonstrated a decrease in QT, QTc intervals and arrhythmias with Febuxostat.
Moreover, pretreatment with Febuxostat produced significant decrease in TNF‑α when compared to Isoproterenol treated rats. This coincides with the results of Hao et al. (2019) who investigated the effect of Febuxostat on serum cytokines IL‑1, IL‑4, IL‑6, IL‑8, TNF‑α and COX‑2. He showed that Febuxostat plays a positive role in reducing inflammatory responses in the body. The possible mechanism of action is that it inhibits the transformation of hypoxanthine into xanthine by means of oxidation.
Furthermore, pretreatment with Febuxostat also produced significant decrease in serum cTnI when compared to Isoproterenol treated rats. Jain et al. (2018) revealed that Febuxostat pretreated group of animals also showed decrease in level of malondialdehyde with increase in level of defensive antioxidant enzyme (CAT, SOD, GSH). Thus, Febuxostat exerts antioxidant activity against Isoproterenol induced myocardial fibrosis. This result is also in agreement with Tanno et al. (2018) who studied the protective effects of Topiroxostat on an ischemia-reperfusion model of rats’ Heart. He showed that Topiroxostat as well as Allopurinol and N-acetyl cysteine significantly reduced the release of CPK and LDH from perfused hearts with ischemia reperfusion (I/R) injury, suggesting that these agents prevent the cardiomyocyte death and exert protective effects against ischemia reperfusion I/R injury.
Also, Febuxostat produced improvement of Isoproterenol- induced histopathological changes. Cardiomyocytes were arranged in interlacing bundles with normal histological pattern. However, few pathological changes were still evident in the form of areas of lost striations, intercellular and intracellular vacuolations as well as few mononuclear inflammatory cells. This is in accordance with Jain et al. (2018) who revealed that administration of Febuxostat (10 mg/kg/day) significantly reduced the effects of Isoproterenol on myocardial structure when compared with control group.
William et al. (2018) sated in the CARES trial that treatment with Febuxostat resultedin overall rates of major cardiovascular events that were similar to those associated with Allopurinol treatment among patients with gout who had coexistingcardiovascular disease. However, cardiovascular death and deaths from any cause were more frequent in the Febuxostat group than in the Allopurinol group.
In the present work pretreatment with Cilostazol produced increase in QTc interval compared to Isoproterenol group but this increase was not significant and there was no evidence of arrhythmias. This was contrary to Gamssari et al. (2002) who studied rapid ventricular tachycardias associated with Cilostazol use. He revealed that Cilostazol (and possibly other PDE III inhibitors) poses a probable risk of ventricular tachyarrhythmia.
Moreover, pretreatment with Cilostazol produced significant decrease in TNF‑ α when compared to Isoproterenol treated rats. This is in line with Kangawa et al. (2016) who studied anti-inflammatory effects of Cilostazol, and antioxidants, enzymatically-modified Isoquercitrin and a-lipoic acid on reducing dextran sulphate sodium-induced colorectal mucosal injury in mice. They showed that all the treatment groups exhibited significantly decreased levels of IL-6 and TNF-a compared with the control.
Cilostazol also produced significant decrease in serum cTnI when compared to Isoproterenol treated rats and this is in agreement with Abbas and Kabil (2017) who investigated the effect of Pentoxifylline and Cilostazol on
rat heart injuries induced by Doxorubicin. They demonstrated that Cilostazol decreased troponin I and CK-MB while increased SOD activity with decrease in MDA, IL-6, TNF- α, and caspase-3; thus Cilostazol exert protective effects against Doxorobucin-induced cardiotoxicity.
Furthermore, pretreatment with Cilostazol produced improvement of Isoproterenol- induced histopathological changes. Cardiomyocytes were arranged in interlacing bundles with normal histological pattern. However, few pathological changes were still evident in the form of areas of lost striations, intercellular and intracellular vacuolations as well as few mononuclear inflammatory cells. This is in accordance with Dhakad et al. (2017) who showed that there was reduction in percent infarction of myocardium of Cilostazol and milrinone treated rat hearts as compared to increased infarct size in Isoproterenol treated Wistar rats.
Abbas and Kabil (2017) showed that Cilostazol treatment improved histopathologic features with few degenerative changes in cardiomyocytes with less myofibrillar loss and vacuolization when compared to Doxorubicin group. Doxorubicin group showed loss of striation and inflammation, myofibrillar loss with sarcoplasmic eosinophilia cytoplasmic vacuolization, patchy necrosis and inflammatory cells. She investigated the possible protective effects of pentoxifylline (PTX) and Cilostazol on Doxorubicin-induced cardiotoxicity in rats.
On comparing the cardioprotective effects of Febuxostat and Cilostazol in the present study, there was significant decrease in QTc interval and significant increase in arrhythmia with Febuxostat compared to Cilostazol. Cilostazol led to more reduction in TNF-a and cTnI than Febuxostat but this was insignificant. These results coincide with those of Kangawa et al. (2016) who studied the anti-inflammatory effects of the selective phosphodiesterase 3 inhibitor, Cilostazol and those of Abbas and Kabil (2017) who investigated the effect of Pentoxifylline and Cilostazol against rat heart injuries Induced by Doxorubicin.
Pretreatment with Febuxostat and Cilostazol led to significant improvement in the pathological changes caused by Isoproterenol. This is in line with Dhakad et al. (2017) who showed that there was reduction in percent of infarction of myocardium in Cilostazol and milrinone treated rat hearts as compared to increased infarct size in Isoproterenol treated Wistar rats. This is in line with Jain et al. (2018) who revealed that administration of Febuxostat (10 mg/kg/day) significantly reduced the effects of Isoproterenol on myocardial structure when compared with control group.
Yet, there was no significant difference between Febuxostat and Cilostazol regarding histopathological changes.
CONCLUSION
Pretreatment with Cilostazol is more cardioprotective than Febuxostat as it led to more reduction in TNF-α without increasing arrhythmias or affecting QT and QTC intervals as compared to Febuxostat.
Recommendations
(1) Further experimental studies are required to clarify the protective mechanisms of Febuxostat and Cilostazol in treatment of Isoproterenol induced cardiotoxicity.
(2) Further experimental studies are required to clarify the cause of decreased QT, and QTC intervals and arrhythmia in Febuxostat treated rats.
(3) Clinical studies are required to confirm the experimental data and elucidate the potential protective role of Febuxostat and Cilostazol.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abbas N, Kabil S (2017). Pentoxifylline and Cilostazol Against Rat Heart Injuries Induced by Doxorubicin. Egyptian Journal of Basic and Clinical Pharmacology 7 p. |
|
|
Badore NS, Das PK, Pillai S, Thakur A (2017). Role of Ginkgo biloba Extract, Against Isoproterenol Induced Cardiac Toxicity in Rats. Indian Journal of Pharmaceutical Education and Research 51(4):691-699. |
|
|
Deng XY, Chen JJ, Li HY, Ma ZQ, Ma SP, Fu Q (2015). Cardioprotective effects of Timosaponin B II from Anemarrhenae asphodeloides Bge on Isoproterenol-induced myocardial infarction in rats. Chemico-Biological Interactions 240:22-28. |
|
|
Dhakad P, Kumar P, Kumar S, Sharma A, Mishra R, Dixit A (2017). Cardio Protective Action of Cilostazol, Milrinone and Their Combination over Isoproterenol Induced Myocardial Infarction in Wistar Rats. International Journal of Cardiovascular and Cerebrovascular Disease 5(1):8-14. |
|
|
Eom YW, Jung HY, Oh JE, Lee JW, Ahn MS, Youn YJ, Ahn SG, Kim JY, Lee SH, Yoon J, Yoo BS (2016). Isoproterenol Enhances Tumor Necrosis Factor-Related Apoptosis- Inducing Ligand-Induced Apoptosis in Human Embryonic Kidney Cells through Death Receptor 5 up-Regulation. Korean Circulation Journal 46(1):93-98. |
|
|
Filho HJL, Ferreira NL, DeSousa RB, deCarvalho ER, Lobo PLD, Filho JGL (2011). Experimental model of myocardial infarction induced by Isoproterenol in rats. Brazilian Journal of Cardiovascular Surgery 26(3):469-476. |
|
|
Gamssari F, Mahmood H, Ho JS, Villareal RP, Liu B, Rasekh A, Massumi A (2002). Rapid ventricular tachycardias associated with cilostazol use.Texas Heart Institute Journal 29(2):140. |
|
|
Hao G, Duan W, Sun J, Liu J, Peng L (2019). Effects of Febuxostat on serum cytokines IL 1, IL 4, IL 6, IL 8, TNF α and COX-2 Experimental and Therapeutic Medicine 17(1):812-816. |
|
|
Jain B, Chaudhari S, Khatal S (2018). Evaluation of xanthine oxidase inhibitor Febuxostat in myocardial fibrosis. International Journal of Research in Pharmacy and Pharmaceutical Sciences 3(6):11-15. |
|
|
Kangawa Y, Yoshida T, Abe H, Seto Y, Miyashita T, Nakamura M, Kihara T, Hayashi SM and Shibutani M.(2016). Anti-inflammatory effects of the selective phosphodiesterase 3 inhibitor, Cilostazol, and antioxidants, enzymatically-modified Isoquercitrin and a-lipoic acid, reduce dextran sulphate sodium-induced colorectal mucosal injury in mice. Experimental and Toxicologic Pathology 69(4):179-186. |
|
|
Parikh H (2015). Investigation of cardioprotectivc effects of Crataegus oxycantha and its molecular mechanism. Current Research - Cardiology 2:4. |
|
|
Siriporn C, Chattipakorn I, Savitree T, Jantira S, Nipon C (2014). Phosphodiesterase-3 inhibitor (Cilostazol) attenuates oxidative stress-induced mitochondrial dysfunction in the heart. Journal of Geriatric Cardiology 11(2):151. |
|
|
Tanno S, Yamamoto K, Kurata Y, Adachi M, Inoue Y, Otani N, Mishima M, Yamamoto Y, Kuwabara M, Ogino K, Miake J, Ninomiya H, Shirayoshi Y, Okada F, Yamamoto K, Hisatome I (2018). Protective Effects of Topiroxostat on an Ischemia-Reperfusion Model of Rat Hearts. Circulation Journal 82(4):1101-1111. |
|
|
Wang S, Li Y, Song X, Wang X, Zhao C, Chen A, Yang P (2015). Febuxostat pretreatment attenuates myocardial ischemia/reperfusion injury via mitochondrial apoptosis. Journal of Translational Medicine 13(1):209 |
|
|
William B, Kenneth G, Michael A, Jeffrey S, Philip B, Whelton A, Hunt B, Castillo M and Gunawardhana L (2018). Cardiovascular Safety of Febuxostat or Allopurinol in Patients with Gout. New England Journal of Medicine 378(13):1200-1210. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


