ABSTRACT
Genetic polymorphisms of certain classes of glutathione S-transferase (GST), enzyme responsible for the biotransformation of drugs and xenobiotics, have been associated with risk of several cancers such as cervical cancer. The aim of this study is to investigate the impact of glutathione S-transferase M1 and T1 deletion on high-risk human papillomavirus (HR-HPV) infections and on dysplasia. A case-control study was carried out on 1069 endocervical samples from West African women including 482 HR-HPV positive and 139 patients had cervical lesions according to visual inspection with acetic acid and Lugol (VIA/VILI) screening. Deletion of the GSTM1 and GSTT1 genes was determined using conventional PCR and genotypes of HR-HPV by real-time PCR. An association with a reduced risk for HR-HPV infection was observed in Ivorian population with GSTT1-null (OR = 0.61, 95% CI = 0.40 - 0.92, p= 0.02) and GSTM1-active/GSTT1-null genotypes (OR = 0.56, 95% CI = 0.35 - 0.90, p= 0.02). In West African, women with GSTT1-null genotype had 1.72-fold higher risk for infection with HPV66 (p= 0.044) and reduced risk (OR = 0.39) for HPV35. Whereas women with GSTM1-null/GSTT1-active genotype had 2.32-fold higher risk for HPV18 infection (p= 0.042). GSTT1-null genotype was associated to cervical lesions in West African with a reduced risk (OR = 0.63, p= 0.017). The results of the present study demonstrate that GSTT1-null could be associated with cervical lesions and HPV35 infection with reduced risk. GSTM1-null associated with GSTT1-active could play a role in increasing the risk for HPV18 infection.
Key words: Cervical cancer, GSTM1, GSTT1, HR-HPV, West Africa.
Cervical cancer is a major challenge for developing countries. The human papillomavirus (HPV) is considered as the main etiological agent responsible for cervical cancer (Walboomers et al., 1999). In 2018, the global incidence of cervical cancer was estimated at 570,000 cases with 311,000 deaths (Bray et al., 2018). About 85% of cases related to cervical cancer occur in low-income countries (Chuang et al., 2016; Randall and Ghebre, 2016). The disease was the fourth most common diagnosed cancer in women worldwide and the second in terms of incidence and mortality in developing countries (Bray et al., 2018). The highest incidence and mortality rates are recorded in Southern Africa followed by East and West Africa (Guinea, Burkina Faso and Mali) (Bray et al., 2018). According to WHO, cervical cancer related mortality might increase by 42% to reach 442,926 deaths in 2030 (WHO, 2015). The largest increase will occur in low- and middle-income countries and could be due to specific factors influencing HPV infection and cervical cancer in sub-Saharan Africa. Persistent HPV infections remain the main cause of precancerous lesions and cervical cancer (Walboomers et al., 1999; Schneider et al., 1992). Despite the fact that HPV infected women are at high risk for cervical cancer, not all infected women develop the disease as the infection is most often detected in asymptomatic people (Wheeler et al., 1993). Only a minority would develop cancer; the neoplastic lesions can regress spontaneously. Malignant transformation occurs during a period of 15 to 20 years in the infected epithelium of the cervix (Zur Hausen, 2002)and also involve the host genetic factors in the progression of the disease.
Among these genetic factors there is mounting evidence about glutathione S-transferase (GST) gene polymorphisms. Glutathione S-transferase (GST) is a polymorphic enzyme involved in the conjugation of reduced glutathione to harmful electrophilic compounds and in chemo-resistance to anticancer agents. Isoenzymes of GST are involved in detoxification of carcinogen and play a very important role in the cellular defense system. GSTs belong to the family of cytosolic enzymes (GST, EC 2.5.1.18) divided into 8 classes: mu (GSTM), alpha (GSTA), pi (GSTP), theta (GSTT), zeta (GSTZ), sigma (GSTS) ), kappa (GSTK) and omega (GSTO) (Hayes and Pulford, 1995, Hayes and Mclellan, 1999). GST enzymes are soluble with a molecular mass of about 25 kDa. The most studied polymorphisms of GST genes consist of mu, theta and zeta classes and the subclasses are mainly GSTM1, GSTT1, GSTP1. The present study will focus on the polymorphisms of the GSTM1 and GSTT1 genes in West African women. So far, a single nucleotide polymorphism (G2619C at 534 position 7 exon) or a complete deletion of the gene was reported for GSTM1 subclass with three known alleles: GSTM1*A, GSTM1*B and GSTM1*0. The first two alleles differ by a single nucleotide in exon 7 of the gene with no influence on the enzyme activity. The null allele GSTM1*0 also called GSTM1-null results in the absence of the GSTM1 enzyme. People with complete deletion of the GSTM1 gene seem unable to metabolize epoxides or quinones (Hayes and Pulford, 1995; Hayes and Strange, 2000). The frequency of the null allele GSTM1*0 is estimated at 50% in Caucasians and 27% in Asian population. GSTT1 gene polymorphisms (A310C) result in the substitution of threonine residue into proline at position 104 of the amino acid sequence (Eaton and Bammler, 1999)with three alleles named GSTT1*A, GSTT1*B and GSTT1*0. The latter also called GSTT1-null differs from the first two alleles by an absence of enzymatic activity with a frequency estimated at 20 and 61% in Caucasian and Asian population respectively. Insufficient detoxification caused by gene polymorphism of the metabolizing enzymes or dysregulation in the elimination system of toxins (oxidative stress) from the body can lead to increased exposure to reactive carcinogenic derivatives and contribute to the malignant cellular reaction in women infected with HPV.
According to studies, oxidative stress was associated with an increase in viral replication in cells infected (Scholz et al., 1996), and the increase in oxidants has been associated with neoplastic progression of HPV16 (De Marco et al., 2012). Several studies in our laboratory have identified a number of high-risk HPVs associated with cervical lesions in West Africa other than 16 and 18 (Zohoncon et al., 2020). The importance of studying GSTM1, GSTT1 genes deletion and high-risk HPV infection and precancerous lesions is very necessary. Several studies have investigated the association of GSTM1 and GSTT1 deletion in the acquisition of precancerous lesions and study cervical cancer in different countries with the exception of Africa. In this first pioneering study of a population of women from several West African countries, we have examined and verified the hypothesis that the deletions of GSTM1 and GSTT1 are associated with HR-HPV infection and the precancerous lesions.
Ethical aspects
The women recruited gave their free and informed consent to participate in the study according to the Helsinki Declarations. The research protocol was approved by the Ethics Committee for Health
Research (CERS) of Burkina Faso on January 10, 2018 with reference number 2018-01-012. The information obtained from the patient are kept strictly confidential. The results were used for a better therapy of women.
Type, site and study population
The study population consisted of 1,069 samples randomly selected from 2,133 endocervical samples collected from women in the general population of five West African countries, namely Benin, Burkina Faso, Côte d'Ivoire, Niger and Togo. HPV sampling and genotyping were carried out in 2017 as part of an earlier study funded by the “Agence Universitaire de la francophonie” (AUF). Ten cities were selected for sample collection in the five countries according to their importance in terms of population density and geographic location.
This is a cross-sectional, case-control study. We considered the high-risk HPV positive samples as the cases and the high-risk HPV negative samples as the controls. The distribution of the number of samples by city was: 99 cases and 111 controls chosen from 234 samples in Ouagadougou (Burkina Faso), 63 cases and 76 controls from 239 samples in Kara (Togo), 183 cases and 214 controls from 484 samples in Abidjan-Bouaké-Yamoussoukro (Côte d’Ivoire), 108 cases and 134 controls among 484 samples in Parakou-Cotonou-Borgou/Alibori-Abomey Calavi (Benin) and 29 cases and 52 controls chosen from 250 samples in Niamey (Niger). The sample size in each country was calculated according to the prevalence of HPV in the country. In total, there were 482 cases and 587 controls. Among the 1069 samples selected, 139 patients were carriers of lesions and 897 patients were without lesions according to the VIA/VILI tests.
Cervical specimen collection and screening for precancerous lesions
After sensitizing the study respondents about how to prevent HPV infection and cervical cancer risk, and obtaining free and informed consent from the women, a questionnaire was administered to the women to collect their socio-demographic, behavioural and clinical information. Endocervical swab samples were taken from the uterus of the respondents using a sterile cotton swab and a single use speculum; behind screening was done for visual inspection using acetic acid and Lugol (IVA/VILI) to determine cervical lesions or dysplasia in the women. An examination could specify the lesions types were not known. Patients with a positive VIA or VILI test were considered to have cervical lesions or dysplasia, and those with a negative VIA / VILI were considered to have normal cytology.
The samples obtained were immersed in a transport medium from the DNA-Sorb-A kit (Sacace Biotechnologies, Como, Italy) and stored at -20°C in the laboratory of the various sites. In CERBA/LABIOGENE (Pietro Annigoni Biomolecular Research Center / Molecular Biology and Genetics laboratory) of Ouagadougou (Burkina Faso), DNA was extracted, high-risk HPV genotypes were characterized and GSTM1 and GSTT1 deletion was done.
DNA extraction
The DNA of the endocervical samples was extracted using the commercial kit called "DNA-Sorb-A" from sacace biotechnologies® according to the manufacturer's protocol. The extracted DNA was stored at a temperature of -20°C in order to carry out PCR amplifications.
HR-HPV detection
HR-HPV was detected with the HPV Genotypes 14 Real-TMQuant kit (SACACE Biotechnologies®, Italy) using real-time multiplex PCR test for detection of 14 high-risk genotypes (HPV-16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68). For PCR amplification, each DNA sample, to be amplified was distributed in 4 tubes at the rate of 10 μl/tube. Each tube previously contained 15 µl of the reaction mixture and target specific genotypes. Positive and Negative controls given by the supplier have been performed following the same procedure.
The reaction mixture of 15 μl in the 4 tubes was composed of a mixture of Hot Start DNA, PCR-buffer-FRT and respectively the primers L1, E6 and E7 of the target regions of 3 to 4 HR-HPV and internal control (PCR-mix-1 16, 18, 31, IC; PCR-mix-1 39, 45, 59, IC; PCR-mix-1 33, 35, 56, 68; PCR-mix-1 51, 52, 58, and 66). The amplification program was 1 cycle of 95°C for 15 min, followed by 5 cycles of 95°C for 5 s, 60°C for 20 s and 72°C for 15 s and finally 40 cycles of 95°C for 5 s, 60°C for 30 s and 72°C for 15 s. The results were interpreted using Microsoft Excel program software called HPV Genotypes 14 Real-TM.xls (SACACE Biotechnologies®, Italy) according to the manufacturer's protocol.
GSTM1 and GSTT1 polymorphisms characterization
The method used for the genotyping of GSTM1 and GSTT1 is a conventional multiplex PCR described by Chen et al. (Chen et al., 1997). The primers used were _F’: 5’GAACTCCCTGAAAAGCTAAAGC-3’ and R’ : 5’GTTGGGCTCAAATATACGGTGG-3’ for GSTM1; _F’ : 5’-TTCCTTACTGGTCCTCACATCTC-3’ and R’ : 5’-TCACCGGATCATGGCCAGCA-3’ for GSTT1 ; _F ’: 5’CAACTTCATCCACGTTCACC-3’ and R’ : 5’GAAGAGCCAAGGACAGGTAC-3’ for internal control (β-globine). Each well contained 10μl of Taq Gold 360 Master Mix Ampli, 1μl of each primer, 7μl of sterile water, 2μl of DNA. The PCR amplification program began with a denaturation step at 94°C for 5 min followed by 35 cycles at 94°C for one min, 57°C for 1 min and 72°C for one minute, ending with an extension at 72°C for 7 min.
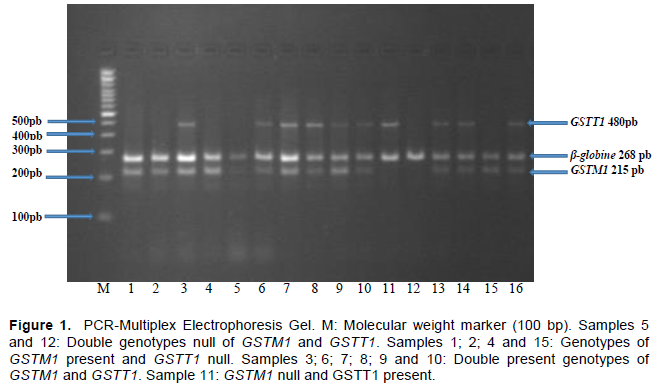
PCR amplification products were revealed by 3% agarose gel electrophoresis containing ethidium bromide. The bands of 215 bp, 480 bp and 268 bp were allocated to GSTM1, GSTT1, and β-globin, respectively (Figure 1). The absence of PCR products corresponding to GSTM1, GSTT1 was considered to be zero genotype and invalid PCR in the absence of PCR products corresponding to β-globin.
Statistical analysis
Our data were analyzed by Excel 2016 software, SPSS Statistics 25.0.0.0, Epi Info 7.2.2.6. The confidence interval was set at 95% and the fisher test was used for the comparison. The difference was statistically significant for p <0.05.
Sociodemographic characteristic of the study population
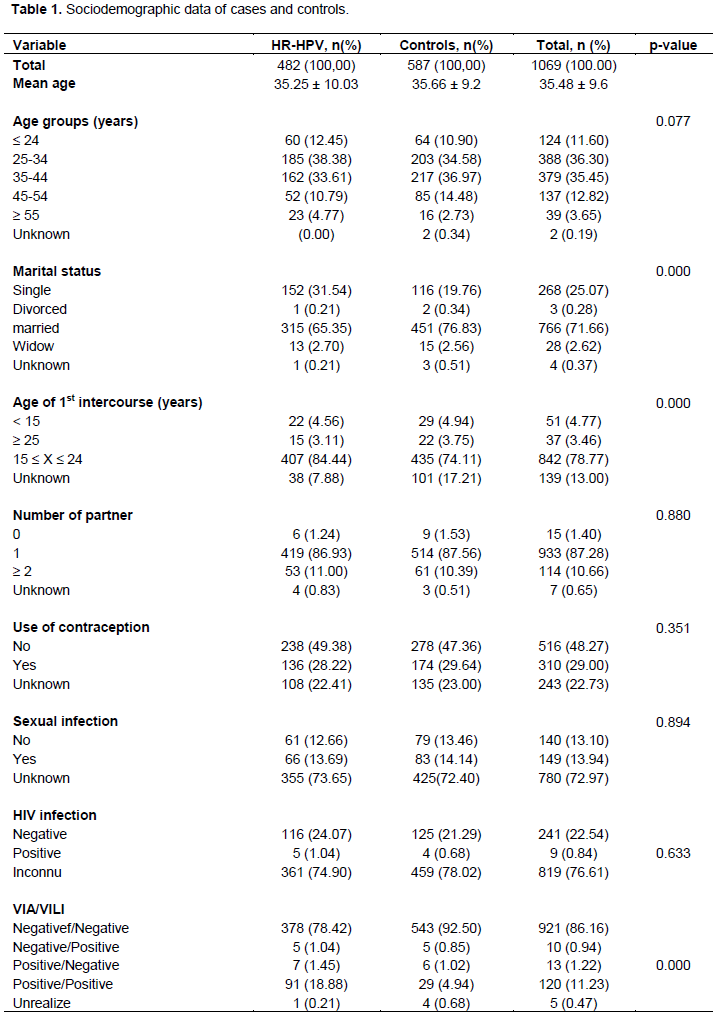
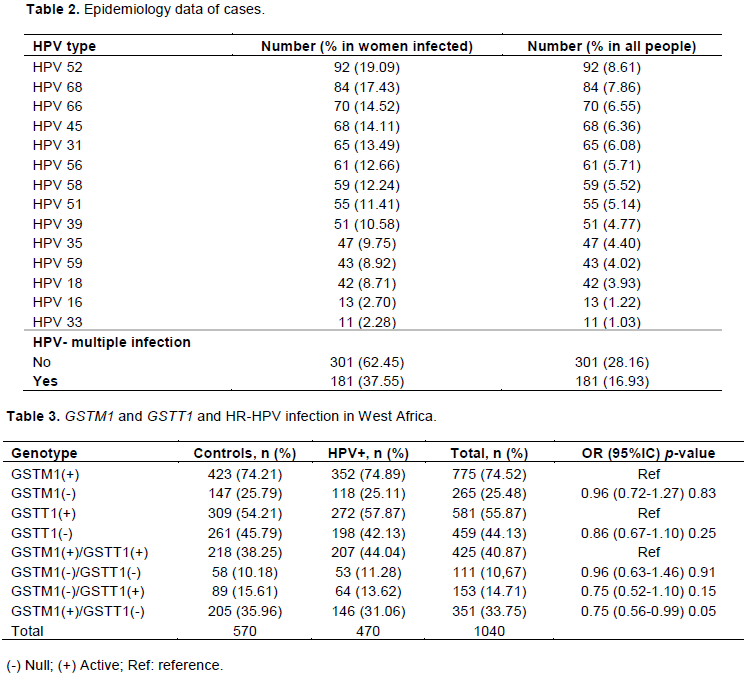
The present study concerned 1069 samples. Table 1 shows the sociodemographic characteristic of the study population. Their ages range from 15 to 72 years with a mean of 35.48 ± 9.6 years. The median age was 35 years. 25-34 and 35-44 age groups were the most represented with frequencies of 36.30 and 35.45%, respectively. The study population was made of 64.36% of women who were less than 30 years old. The married wives in our study represented 71.66% of the study population. Women who had their first sexual intercourse between 15 and 24 years old represented 78.77% (842/1069). The number of sexual partners ranged from zero to more than two. About 29% of women said they were on contraception, 13.94% had contracted a sexually transmitted infection during their life, 0.84% said they were diagnosed with HIV. VIA/VILI tests were negative in 86.16% of the study population. HR-HPV infections accounted for 45.09% (28.16 single infections and 16.93% multiple infections). The most frequent HR-HPV in cases and controls were HPV 52 (Table 2)
GSTM1, GSTT1 polymorphism and HPV infection in western Africa
In our study 29 (2.71%) samples were considered invalid after PCR because no band was detected during electrophoresis migration. One thousand and forty (1040) samples produced valid results during PCR testing. Table 3 shows GSTM1 and GSTT1 and HR-HPV infection in West Africa. The presence of the GSTM1 and GSTT1 was observed in 74.52 and 55.87% of the population, respectively. The absence of GSTM1 also called GSTM1-null was observed in 25.48% (265/1040) of which 25.79% (147/570) were in the controls and 25.11% (118/470) were in positive cases for HR-HPV (OR = 0.96; 95% CI = 0.72 - 1.27; p= 0.83). That of the GSTT1 also called GSTT1-null is 44.13% with 45.79% in controls and 42.13% in positive cases for HR-HPV (OR = 0.86; 95% CI = 0.67 - 1.10; p= 0.2).
In the GSTM1 and GSTT1 associations, we found 40.87% (425/1040) of GSTM1-active/GSTT1-active, 10.67% of GSTM1-null/GSTT1-null (OR = 0.96; 95% CI = 0.63 - 1.46; p= 0.91); 14.71% and 33.75% of GSTM1-null/GSTT1-active (OR = 0.75; 95% CI = 0.52 - 1.10; p= 0.15) and GSTM1-active/GSTT1-null (OR = 0.75; 95% CI = 0.56 - 0.99; p= 0.05) respectively in the population. The analysis had shown in the general population non-significant associations of glutathione-S-transferase deletion and HR-HPV infection (Table 3).
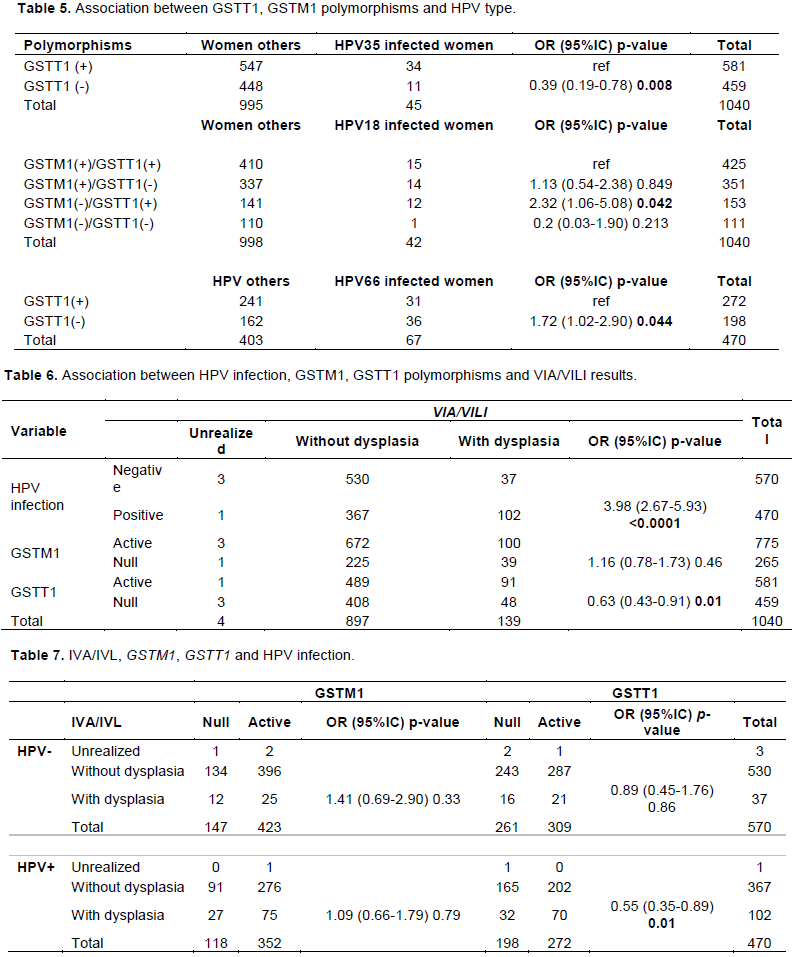
On the other hand, statistically significant associations in our population was observed in carrying out of the GSTM1-null/GSTT1-active genotype with a 2.32-fold higher risk in HPV 18 infection compared to GSTM1-active/ GSTT1-active in the study population (95% CI = 1.06 - 5.08; p= 0.042). Carriers of the GSTT1-null genotype had a 1.72-fold higher risk of HPV 66 infection compared to other HPV genotypes (CI = 1.02 - 2.90; p= 0.044). However, there was a decrease in HPV 35 infection for women with the GSTT1-null genotype in the study population (OR = 0.39; 95% CI = 0.19 - 0.78; p= 0.008) (Table 5).
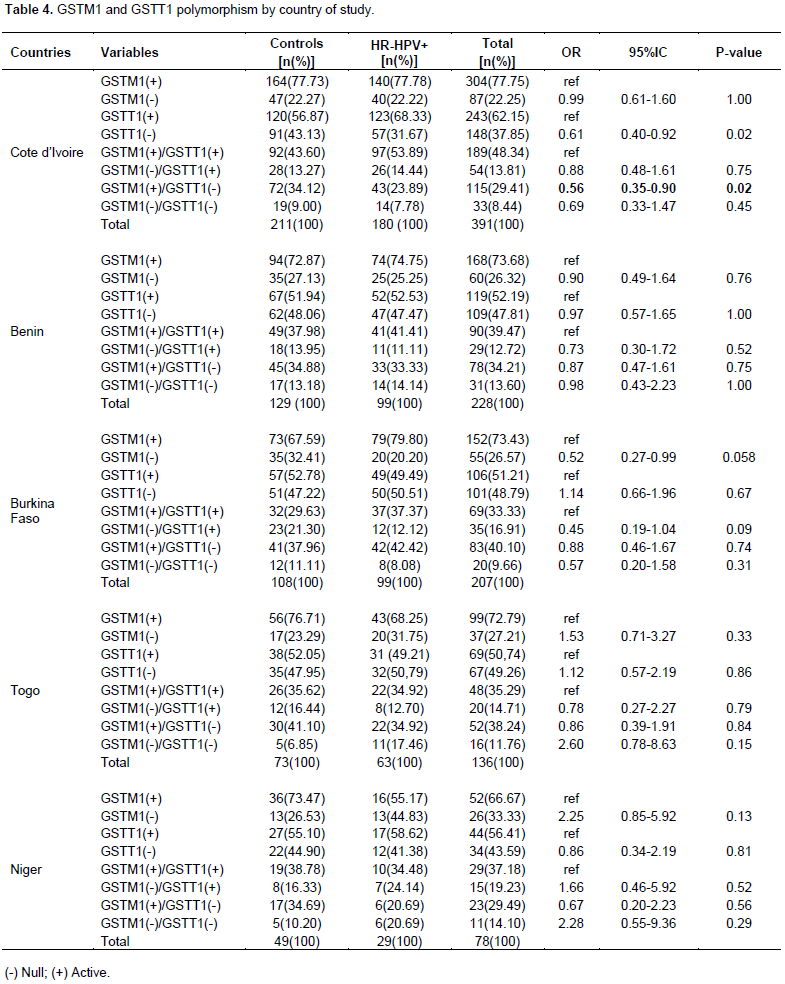
GSTM1 and GSTT1 polymorphism and HR-HPV infection in different countries of study
Table 4 reveals the distribution of the deletion polymorphisms of GSTM1 and GSTT1 in the different countries of our study. GSTM1-active and GSTT1-active were 77.75 and 62.15% respectively in Côte d’Ivoire, 73.68 and 52.19% in Benin, 73.43 and 51.21% in Burkina Faso, 72.79 and 50.74% in Togo, and 66.67 and 56.41% in Niger. GSTM1-null, GSTT1-null, GSTM1-active/GSTT1-null, GSTM1-null/GSTT1-active, and GSTM1-null/GSTT1-null in this study did not show any significant difference between positive cases of HR-HPV and controls in the population of Burkina Faso, Togo, Benin and Niger. On the other hand, in the Ivorian population, we observed a significant difference by comparing the cases with the controls for GSTT1-null and the association between GSTM1-active/GSTT1-null. Their frequency in the population was respectively 37.85% (OR = 0.61; 95% CI = 0.40-0.92; p= 0.02) and 29.41% (OR = 0.56; 95% CI = 0.35-0.90; p = 0.02) with reduced risk of infection (OR <1). GSTM1-null in Niger, the associations GSTM1-null/GSTT1-null in Niger and in Togo had marginal risks of 2.25; 2.28 and 2.60 respectively.
GSTM1, GSTT1 polymorphisms and HPV infection in cervical lesions or dysplasia
Table 6 shows the distribution of HR-HPV infection and the deletion polymorphisms studied as a function of the results of the VIA/VILI tests. In women, HR-HPV infection was significantly associated with cervical lesions with the risk of 3.98-fold higher compared to women with negative HPV (95% CI = 2.67-5.93; p <0.0001). GSTT1-null had statistically significant frequencies with a reduced risk of cervical lesions compared to GSTM1-active (OR = 0.63; 95% CI = 0.43 - 0.91; p = 0.01). Unlike the GSTT1-null genotype,
GSTM1-null and the double null genotype did not have statistically significant results. However, a risk of 0.55 was found in the double genotype GSTM1-active/GSTT1-null compared to GSTM1-active/GSTT1-active genotype in cervical lesions (95% CI = 0.35-0.86; p = 0.009). Table 7 presents the HPV, GST statuses as a function of the test results; women carrying GSTT1-null genotype, and HPV positive had a statistically significant result. Cervical lesions are linked to reduction in risk compared to GSTT1-active (OR = 0.55; 95% CI = 0.35-0.89; p = 0.01).
GSTM1, GSTT1 deletion and socio-demographic characteristic
The study did not show significant results of the respondents’ socio-demographic characteristic such as age, marital status, age of 1st intercourse, contraception using, sexual partner, sexual infection, HIV infection with deletion of GSTM1 and GSTT1.
The present study aims to assess the risk of Glutathione S-Transferase M1 and T1 polymorphisms in HR-HPV infection and cervical lesions or dysplasia in women. In literature, very few studies have been carried out on HR-HPV infection in relation to the deletions of GSTM1 and GSTT1. Our study is the first in sub-Saharan Africa and West Africa particularly, where HPV infection is very common.
In this study, 29 samples (02.71%) were invalid after PCR testing. Different studies on polymorphisms have largely used blood samples (Ueda et al., 2010; Agodi et al., 2010). In our study, we used endocervical cells samples. There were very few samples, with a low DNA concentration when checked with the nanodrop. Endocervical cells could explain this low DNA concentration after extraction. This would therefore lead to illegible bands after electrophoresis.
Oxidative stress, according to studies, had been associated with an increase in viral replication (Scholz et al., 1996; Koike, 2009). According to De Marco et al. (2012), increased oxidants are associated with the neoplastic progression of HPV16 (De Marco et al., 2012). Several factors are responsible for oxidative stress. The genetic factors are the most crucial and influential. The main enzyme P450 cytochromes, catalyze the different oxidation reactions in phase I, producing oxidative stress by the metabolic activation of chemical carcinogens and xenobiotics (Lang and Pelkonen, 1999). The products resulting from this phase are reactive electrophilic intermediates and can cause lipids, proteins and DNA damage (Shackelford et al., 2000). Glutathione S-transferases, one of the groups of phase II enzyme, neutralize these reactive electrophiles by conjugating them with glutathione, making them more soluble in water (Ketterer et al., 1993; Wilce and Parker, 1994; Armstrong, 1997), and thus eliminating oxidative stress. The deletions of genes by these enzymes could lead to the persistence of oxidative stress, causing viral multiplication, DNA damage by reactive electrophiles attacks or chromosomal instability, and consequently the carcinogenic process.
According to Ueda et al. (2010) certain high-risk HPV-infections were associated with polymorphisms of glutathione S-transferase. Our study did not show an association between the GSTM1-null, GSTT1-null genotypes and HR-HPV infection in West Africa population. These results are similar to those found by Agodi et al. (2010) in Italy. Their results and ours suggested that the deletion of GSTM1, GSTT1 genotypes is not associated in general with HPV-infection. However, particularities could exist according to the HR-HPV types.
The study also showed that the double GSTM1-active/GSTT1-null genotype was associated with HR-HPV infection, particularly in Côte d'Ivoire, with a relative risk always <1 (OR = 0.56). These results, although significant, showed no increased risk of HR-HPV infection, but rather a decrease in risk. The double GSTM1-active/GSTT1-null genotype could protect women from HPV-infection. GSTs could modulate signal transduction pathways involved in cell survival and apoptosis, by controlling the activity of protein members of the mitogen-activated kinase family (MAPK) (Laborde, 2010; Singh, 2015). In normal conditions, ASK1 would be sequestered by GSTM1 enzyme and forming the GSTM1/ASK1 complex. In oxidative stress conditions or heat shock, there is dissociation of the complex and activation of ASK1 and subsequently the induction of the apoptosis process. It could contribute to kill cell-infection although GSTT1 is an exposure factor.
In addition, in the general population of study, by comparing each type of HR-HPV in the study population and each type of HR-HPV with the other remaining HR-HPV, there is an association with increased risk between infection with HPV18 and double genotype GSTM1-null/GSTT1-active (OR = 2.32; p = 0.042). Agodi et al. (2010), as in this study, did not find a significant association between the suppression of the GSTM1, GSTT1 genes and infection with HPV16 despite the fact that this is considered the most common in premalignant and malignant cervical lesions (Muñoz et al., 2003). The study also showed an association between HPV66 infection and the GSTT1-null genotype with an increased risk (OR = 1.72; p= 0.04) and another association between HPV35 infection and the GSTT1-null genotype (OR = 0.39; p= 0.008) with risk reduced. These results differ from those found by Ueda et al.(2010) in Japan who reported a significant association between HPV16/18 infection and the GSTT1-null genotype (p= 0.029) compared to the other HR-HPV. However, we have not found in the literature an association between HPV66 and HPV35 infection with GSTT1-null genotype. This could be explained by the very few number of studies on HR-HPV infection and polymorphism of glutathione S-transferase. This peculiarity of HPV66, HPV35 association with GSTT1-null in West Africa could also be due to the diversity of emergence of other high-risk HR-HPV (than HPV16/18), which are more frequent in these countries (Zohoncon et al., 2020).
In literature according to several studies and reviews, GSTT1-null and GSTM1-null could be associated with the development of cervical cancer (Lee et al., 2004; Ueda et al., 2005; Ueda et al., 2010; Wang et al., 2011; Liu and Xu, 2012; Sun and Song, 2016; Liu et al., 2017). However, our data were collected by questionnaires and the visual inspection tests were done with acetic acid and lugol (VIA/VILI) for the detection of cervical lesions or dysplasia in the endocervix. Lack of confirmations of the lesions types and grade by biopsy after the VIA/VILI tests constitutes a limitation of the study. Although the IVA/IVL screening tests recommended for low-resource countries are necessary, the results are not very specific like those of histology or cytology.
Regarding the deletions of GSTM1 and GSTT1 genes and the cervical lesions, there is an association between GSTT1-null genotype and cervical lesions by VIA/VILI detection (p= 0.01) with a decrease in risk (OR = 0.63). Satinder et al. (2017) in India, also found a reduced risk linked to cervical cancer (OR = 0.5; p= 0.04) in carriers of the GSTT1-null genotype. The GSTs, according to certain studies do not lead to detoxification complete (van Bladeren, 2000). The conjugate could be reversible or not stable and could lead to high toxic metabolite. It was demonstrated that the GST-dependant conjugation involving GSTT1-null enzyme for certain substrate such as hydrocarbon mono- or di-halogens would lead to very reactive electrophile responsible for carcinogenesis (Hayes and Pulford, 1995, van Bladeren, 2000). In view of these results, the GSTT1-null genotype could contribute to a reduction in the risk of acquiring lesions and cancer of the cervix.
Our results showed an absence of association between GSTM1-null and cervical lesions (p= 0.46). Several studies have shown this absence in association between the GSTM1-null genotype and the intraepithelial lesions in Italy (Agodi et al., 2010; Palma et al., 2010), India (p= 0.67) (Sharma et al., 2015), and Serbia (p= 0.07) (Stosic et al., 2014). An absence of GSTM1-null association was also noted in India in Squamous cell carcinomas (SCC) and adenocarcinoma (AC) (Abbas et al., 2013; Satinder et al., 2017) and in cervical cancer in Turkey (p= 0.73) (Kiran et al., 2010). In addition, in women with SCC and AC in Brazil, Tacca et al. (2018) determined survival of 80.0% in women with GSTM1-active and 73.3% in women with GSTM1-null after a 60-month follow-up and also found statistically insignificant results (p= 0.368). These results suggested that the genotype GSTM1-null could not be associated with lesions and cervical cancer.
In terms of gene-gene interactions, the study showed a reduction in the risk of cervical lesions (OR = 0.55; p = 0.009) for carriers of the GSTM1-active / GSTT1-null double genotype. Furthermore, Satinder et al. (2017) found an OR <1 also statistically significant in India for the double genotype GSTM1-active / GSTT1-null for cervical cancer (OR = 0.4; p= 0.02) and SCC (OR = 0.4; p= 0.04). This is contrary to our study which focused on cervical lesions by IVA/IVL detection. The double GSTM1-active/GSTT1-null genotype would contribute, just like the GSTT1-null genotype to reduce the risk of cervical lesions according to our study. GSTT1 and GSTM1 could play an important role in oxidative stress or in the metabolization of xenobiotic or regulation cell, which could partially compensate for the absence of one of two.
The enzymes responsible for the metabolism of carcinogens would be important risk modifiers in carcinogenesis (Sheweita, 2000). Thus, in the case of persistent infection with HR-HPV, oxidative damage to DNA caused by enzyme deletion could indeed serve as a mechanism to facilitate the integration of HPV, and subsequently, carcinogenesis (Williams et al., 2011). In the study, in women infected with HR-HPV, there were no statistically significant results (p= 0.79) in cervical lesions by VIA/VILI detection in carriers of GSTM1-null genotype. Nunobiki et al. (2015) also showed statistically insignificant results (p= 0.35) of the GSTM1-null genotype in intraepithelial lesions de haut grade (HSIL) in Japan among women infected with HPV. The mean results of the GSTM1-null genotype could not contribute to cervical lesions in women with HPV-infection.
GSTT1-null genotype had statistically significant results (OR = 0.55; p= 0.01) in women with HR-HPV+ and its risk could be reduced for cervical lesions. However in Japan (Nunobiki et al., 2015), Hungary (Cseh et al., 2011) and India (Joseph et al., 2006), they found an increased risk. In the studies by Nunobiki et al. (2015) GSTT1-null was significantly associated with low grade to high grade lesions in HR-HPV positive patients in Japan (OR = 3.45). According to the studies of Cseh et al. in Hungary after 7 years following women with HPV positive, a risk of 1.89-fold higher was attributed to the development of HSIL compared to controls. Joseph et al. determined in India a 19.25-fold higher risk of acquiring invasive cancer and HSIL in women with GSTT1-null genotype, and HPV16 positive compared to controls with normal cytology and low-grade lesions.
As for the double null genotype, we did not find significant results in West Africa for HPV infection and cervical lesions by VIA/VILI detection. In India, Romania and Serbia, non-significant results for the interactions of both null alleles were demonstrated (Stosic et al., 2014; Sharma et al., 2015; Daniel et al., 2016). However GSTs role was demonstrated in cells (Laborde, 2010; Gao et al., 2011; De Marco et al., 2012; Singh, 2015; Wang et al., 2016). Cseh et al. (2011) in Hungary after 7 years of follow up determined a relative risk of 2.35 of HSIL development for women infected with HR-HPV carrying a double null genotype compared to those who have at least one genotype present. Environmental factors could more or less contribute as a cofactor to cervical lesions. It would be more interesting to study the environmental factors as a source of xenobiotic contribution in detoxification genes deletions relation, which could play an important role.
The different case/control studies on the deletions of GSTM1 and GSTT1 by other authors, in addition to performing biopsies unlike ours, included the action of passive and active smoking and exposure to wood smoke (Palma et al., 2010; Abbas et al., 2013; Stosic et al., 2014; Sharma et al., 2015; Satinder et al., 2017; Tacca et al., 2018). Thus, these authors determined statistically significant results between cancer and smoking (Abbas et al., 2013; Tacca et al., 2018); exposure to wood smoke (Satinder et al., 2017), and between cancer, smoking, and GSTM1 and GSTT1 polymorphisms (Sobti et al., 2006; Sharma et al., 2015). In this study, socio-demographic characteristics of the respondents such as smoking and exposure to wood smoke were not included. Two other authors carried out a study on a patient followed-up in Hungary and Brazil (Cseh et al., 2011; Tacca et al., 2018). The size of our samples was disproportionate between the number of women positive for at least one of the positive VIA/VILI tests and those with negative VIA/VILI (139/897), which also does not allow analysis by country.
Our results suggest a reduction in the progression of high-risk HPV infection in the Ivory Coast Republic, in carriers of GSTT1-null and of the double GSTM1-active/GSTT1-null in women with HR-HPV infected. Among women with HR-HPV infection, GSTT1-null genotype could reduce the risk of progression of HPV35 infection and increase HPV66 infection in West Africa. The risk of progression of HPV18 infection would be favored by the GSTM1-null/GSTT1-active genotype in HR-HPV positive women from West Africa. The risk reduction in the acquisition or progression of cervical lesions by VIA/VILI detection could be justified by carrying out the GSTT1-null genotype in the study population and women with HPV infection. GSTM1-active/GSTT1-null may be associated with the reduction of precancerous lesions in West Africa. A study including other genetic cofactors, environmental and confirmed lesions and cancer, would be necessary to shed more light on the various factors influencing carcinogens of cervical cancer.
The authors have not declared any conflict of interests.
We would like to thank the “International Centre for Genetic Engineering and Biotechnology (ICGEB)” for the funding of this research work through the project: "Implication of the host genetic factor in Human Papillomavirus Infection and its associated Cervical lesions and cancer in West African Women". Ref. No. CRP/BFA17-01. We also thank the “Agence Universitaire de la Francophonie” for the financial support and the CERBA/LABIOGENE.
REFERENCES
|
Abbas M, Srivastava K, Imran M, Banerjee M (2013). Association of Glutathione S-transferase (GSTM1, GSTT1 and GSTP1) polymorphisms and passive smoking in cervical cancer cases from North India. International Journal of Biomedical Research 4:655-662.
Crossref
|
|
|
|
Agodi A, Barchitta M, Cipresso R, Marzagalli R, La Rosa N, Caruso M, Castiglione MG, Travali S (2010). Distribution of p53, GST, and MTHFR polymorphisms and risk of cervical intraepithelial lesions in sicily. International Journal of Gynecologic Cancer 20(1):141-146.
Crossref
|
|
|
|
|
Armstrong RN (1997). Structure, catalytic mechanism, and evolution of the glutathione transferases. Chemical Research in Toxicology 10(1):2-18.
Crossref
|
|
|
|
|
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians 68(6):394-424.
Crossref
|
|
|
|
|
Chen C-L, Liu Q, Pui C-H, Rivera GK, Sandlund JT, Ribeiro R, Evans WE, Relling MV (1997). Higher frequency of glutathione S-transferase deletions in black children with acute lymphoblastic leukemia. Blood 89(5):1701-1707.
Crossref
|
|
|
|
|
Chuang LT, Temin S, Camacho R, Dueñas-Gonzalez A, Feldman S, Gultekin M, Gupta V, Horton S, Jacob G, Kidd EA (2016). Management and care of women with invasive cervical cancer: American Society of Clinical Oncology resource-stratified clinical practice guideline. Journal of Global Oncology 2(5):311-340.
Crossref
|
|
|
|
|
Cseh J, Pazsit E, Orsos Z, Marek E, Huszar A, Balogh S, Ember I, Kiss I (2011). Effect of glutathione-S-transferase M1 and T1 allelic polymorphisms on HPV-induced cervical precancer formation. Anticancer Research 31(9):3051-3055.
|
|
|
|
|
Daniel M, Cătană A, Popp RA, Dumitraș DE, Stamatian F, Buzoianu AD, Rotar IC (2016). Genetic polymorphisms of glutathione S transferase and cervical intraepithelial neoplasia. Revista Romana de Medicina de Laborator 24(4):377-386.
Crossref
|
|
|
|
|
De Marco F, Bucaj E, Foppoli C, Fiorini A, Blarzino C, Filipi K, Giorgi A, Schininà, ME, Di Domenico F, Coccia R (2012). Oxidative stress in HPV-driven viral carcinogenesis: redox proteomics analysis of HPV-16 dysplastic and neoplastic tissues. PloS ONE 7(3).
Crossref
|
|
|
|
|
Eaton D, Bammler T (1999). Concise review of the glutathione S-transferase and their significance to toxicology. Toxicological sciences: An Official Journal of the Society of Toxicology 49:156-164.
Crossref
|
|
|
|
|
Gao M, Li Y, Long J, Shah W, Fu L, Lai B, Wang Y (2011). Induction of oxidative stress and DNA damage in cervix in acute treatment with benzo [a] pyrene. Mutation Research/Genetic Toxicology and Environmental Mutagenesis 719(1-2):52-59.
Crossref
|
|
|
|
|
Hayes JD, Mclellan LI (1999). Glutathione and glutathione-dependent enzymes represent a co-ordinately regulated defence against oxidative stress. Free Radical Research 31(4):273-300.
Crossref
|
|
|
|
|
Hayes JD, Pulford DJ (1995). The glutathione S-transferase supergene family: regulation of GST and the contribution of the lsoenzymes to cancer chemoprotection and drug resistance part I. Critical Review in Biochemistry and Molecular Biology 30(6):445-520.
Crossref
|
|
|
|
|
Hayes JD, Strange RC (2000). Glutathione S-transferase polymorphisms and their biological consequences. Pharmacology 61(3):154-166.
Crossref
|
|
|
|
|
Joseph T, Chacko P, Wesley R, Jayaprakash P, James FV, Pillai MR (2006). Germline genetic polymorphisms of CYP1A1, GSTM1 and GSTT1 genes in Indian cervical cancer: associations with tumor progression, age and human papillomavirus infection. Gynecologic Oncology 101(3):411-417.
Crossref
|
|
|
|
|
Ketterer B, Taylor J, Meyer D, Pemble S, Coles B, ChuLin X, Spencer S (1993). Some function of glutathione transferases In K. Tew, B. Mannervik, T. Mantle, C. Pickett, and J. Hayes (Eds.), Structure and Function of Glutathione Transferases. CRC Press, Boca Raton, Florida.
|
|
|
|
|
Kiran B, Karkucak M, Ozan H, Yakut T, Ozerkan K, Sag S, Ture M (2010). GST (GSTM1, GSTT1, and GSTP1) polymorphisms in the genetic susceptibility of Turkish patients to cervical cancer. Journal of Gynecologic Oncology 21(3):169-173.
Crossref
|
|
|
|
|
Koike K (2009). Hepatitis B virus X gene is implicated in liver carcinogenesis. Cancer Letters 286(1):60-68.
Crossref
|
|
|
|
|
Laborde E (2010). Glutathione transferases as mediators of signaling pathways involved in cell proliferation and cell death. Cell death and Differentiation 17(9):1373-1380.
Crossref
|
|
|
|
|
Lang M, Pelkonen O (1999). Metabolism of xenobiotics and chemical carcinogenesis. IARC Scientific Publications 148:13-22.
|
|
|
|
|
Lee S-A, Kim JW, Roh JW, Choi JY, Lee K-M, Yoo K-Y, Song YS, Kang D (2004). Genetic polymorphisms of GSTM1, p21, p53 and HPV infection with cervical cancer in Korean women. Gynecologic Oncology 93(1):14-18.
Crossref
|
|
|
|
|
Liu C, Zeng Y, Ma X, Qi Y, Zhang S, Lv R, Yu H (2017). An Updated Meta-Analysis: Cervical Cancer Risk Conferred by GSTM1 and GSTT1 Polymorphisms. International Journal of Sciences 6(01):52-63.
Crossref
|
|
|
|
|
Liu Y, Xu L-Z (2012). Meta-analysis of association between GSTM1 gene polymorphism and cervical cancer. Asian Pacific Journal of Tropical Medicine 5(6):480-484.
Crossref
|
|
|
|
|
Muñoz N, Bosch FX, De Sanjosé S, Herrero R, Castellsagué X, Shah KV, Snijders PJ, Meijer CJ (2003). Epidemiologic classification of human papillomavirus types associated with cervical cancer. New England Journal of Medicine 348(6):518-527.
Crossref
|
|
|
|
|
Nunobiki O, Ueda M, Akise H, Izuma S, Torii K, Okamoto Y, Tanaka I, Noda S, Akashi K, Higashida T (2015). GSTM1, GSTT1, and NQO1 polymorphisms in cervical carcinogenesis. Human Cell 28(3):109-113.
Crossref
|
|
|
|
|
Palma S, Novelli F, Padua L, Venuti A, Prignano G, Mariani L, Cozzi R, Tirindelli D, Testa A (2010). Interaction between glutathione-S-transferase polymorphisms, smoking habit, and HPV infection in cervical cancer risk. Journal of Cancer Research and Clinical Oncology 136(7):1101-1109.
Crossref
|
|
|
|
|
Randall TC, Ghebre R (2016). Challenges in prevention and care delivery for women with cervical cancer in sub-Saharan Africa. Frontiers in Oncology 6:160.
Crossref
|
|
|
|
|
Satinder K, Sobti R, Pushpinder K (2017). Impact of single nucleotide polymorphism in chemical metabolizing genes and exposure to wood smoke on risk of cervical cancer in North-Indian women. Experimental Oncology 39(1):69-74.
Crossref
|
|
|
|
|
Schneider A, Kirchhoff T, Meinhardt G, Gissmann L (1992). Repeated evaluation of human papillomavirus 16 status in cervical swabs of young women with a history of normal Papanicolaou smears. Obstetrics and Gynecology 79(5):683-688.
|
|
|
|
|
Scholz M, Cinatl J, Gross V, Vogel J-U, Blaheta RA, Freisleben H-J, Markus BH, Doerr HW (1996). Impact of oxidative stress on human cytomegalovirus replication and on cytokine-mediated stimulation of endothelial cells. Transplantation 61(12):1763-1770.
Crossref
|
|
|
|
|
Shackelford RE, Kaufmann WK, Paules RS (2000). Oxidative stress and cell cycle checkpoint function. Free Radical Biology and Medicine 28(9):1387-1404.
Crossref
|
|
|
|
|
Sharma A, Gupta S, Sodhani P, Singh V, Sehgal A, Sardana S, Mehrotra R, Sharma JK (2015). Glutathione s-transferase m1 and t1 polymorphisms, cigarette smoking and hpv infection in precancerous and cancerous lesions of the uterine cervix. Asian Pacific Journal of Cancer Prevention 16(15):6429-6438.
Crossref
|
|
|
|
|
Sheweita SA (2000). Drug-metabolizing enzymes mechanisms and functions. Current Drug Metabolism 1:107-132.
Crossref
|
|
|
|
|
Singh S (2015). Cytoprotective and regulatory functions of glutathione S-transferases in cancer cell proliferation and cell death. Cancer Chemotherapy and Pharmacology 75(1):1-15.
Crossref
|
|
|
|
|
Sobti R, Kaur S, Kaur P, Singh J, Gupta I, Jain V, Nakahara A (2006). Interaction of passive smoking with GST (GSTM1, GSTT1, and GSTP1) genotypes in the risk of cervical cancer in India. Cancer Genetics and Cytogenetics 166(2):117-123.
Crossref
|
|
|
|
|
Stosic I, Grujicic D, Arsenijevic S, Brkic M, Milosevic-Djordjevic O (2014). Glutathione S-transferase T1 and M1 polymorphisms and risk of uterine cervical lesions in women from central Serbia. Asian Pacific Journal of Cancer Prevention 15:3201-3205.
Crossref
|
|
|
|
|
Sun P, Song W-Q (2016). GSTM1 null genotype and susceptibility to cervical cancer in the Chinese population: An updated meta-analysis. Journal of Cancer Research and Therapeutics 12(2):712-715.
Crossref
|
|
|
|
|
Tacca ALcM, Lopes AK, Vilanova-Costa CAST, Silva AMTC, Costa SHN, Nogueira NA, Ramos JEP, Ribeiro AA, Saddi VA (2018). Null polymorphisms in GSTT1 and GSTM1 genes and their associations with smoking and cervical cancer. Genetics and Molecular Research 17(2).
Crossref
|
|
|
|
|
Ueda M, Hung Y-C, Terai Y, Saito J, Nunobiki O, Noda S, Ueki M (2005). Glutathione-S-transferase and p53 polymorphisms in cervical carcinogenesis. Gynecologic Oncology 96(3):736-740.
Crossref
|
|
|
|
|
Ueda M, Toji E, Nunobiki O, Sato N, Izuma S, Torii K, Okamoto Y, Noda S (2010). Germline polymorphisms of glutathione-S-transferase GSTM1, GSTT1 and p53 codon 72 in cervical carcinogenesis. Human Cell 23(4):119-125.
Crossref
|
|
|
|
|
Van Bladeren PJ (2000). Glutathione conjugation as a bioactivation reaction. Chemico-Biological Interactions 129:61-76.
Crossref
|
|
|
|
|
Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kummer JA, Shah KV, Snijders PJ, Peto J, Meijer CJ, Muñoz N (1999). Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. The Journal of Pathology 189(1):12-19.
Crossref
|
|
|
|
|
Wang D, Wang B, Zhai J, Liu D, Sun G (2011). Glutathione S-transferase Ml and T1 polymorphisms and cervical cancer risk: A meta-analysis. Neoplasma 58(4):352-359.
Crossref
|
|
|
|
|
Wang Y, He J, Ma T-J, Lei W, Li F, Shen H, Shen, Z-Y (2016). GSTT1 null genotype significantly increases the susceptibility to urinary system cancer: evidences from 63,876 subjects. Journal of Cancer 7(12):1680.
Crossref
|
|
|
|
|
Wheeler CM, Parmenter CA, Hunt WC, Becker TM, Greer CE, Hildesheim A, Manos MM (1993). Determinants of genital human papillomavirus infection among cytologically normal women attending the University of New Mexico student health center. Sexually Transmitted Diseases 20(5):286-289.
Crossref
|
|
|
|
|
WHO (2015). Others. Projections of mortality and causes of death, 2015 and 2030. Geneva, Switzerland: The World Health Organization.
|
|
|
|
|
Wilce MC, Parker MW (1994). Structure and function of glutathione S-transferases. Biochimica et Biophysica Acta (BBA)-Protein Structure and Molecular Enzymology 1205(1):1-18.
Crossref
|
|
|
|
|
Williams VM, Filippova M, Soto U, Duerksen-Hughes PJ (2011). HPV-DNA integration and carcinogenesis: Putative roles for inflammation and oxidative stress. Future Virology 6(1):45-57.
Crossref
|
|
|
|
|
Zohoncon TM, Djigma WF, Ouattara AK, Traore IMA, Ouedraogo RA, Traore AEM, Bado P, Ouedraogo TC, Diarra B, Ilboudo M, Capo-chichi CD, Obiri-Yeboah D, Karou SD, Nayama M, Horo A, Kouakou KP, Gomina M, Ouattara S, Sanni A, Akpona S, Ouedraogo C, Simpore J (2020). Mapping of fourteen high-risk human papillomavirus genotypes by molecular detection in sexually active women in the West African sub-region. International Journal of Genetics and Molecular Biology 12(1):11-21.
|
|
|
|
|
Zur Hausen H (2002). Papillomaviruses and cancer: from basic studies to clinical application. Nature Reviews Cancer 2(5):342-50.
Crossref
|
|