Full Length Research Paper
ABSTRACT
While multidisciplinary consultation meetings on therapeutic protocols, psychological management, treatment of pain for patients living with cancer are setting up, their nutritional status in Côte-d'Ivoire is almost absent in oncology units. This study aimed to assess the nutritional profile of adult patients with cancer, followed at the oncology service of the University Hospital of Treichville. A descriptive and analytical cross-sectional study was conducted over a 40-day period, from an anonymous questionnaire and involving fifty-three (53) cancer patients. sociodemographic, clinical and biological data as well as qualitative parameters on food consumption (24-hour recall) were collected. The results revealed that the mean age was 51 years with a female predominance (87.5%). The nutritional status of patients was evaluated according to several parameters: The Body Mass Index (BMI) accounted for 8.33% of malnourished patients with 37.5% of patients being obese or overweight. Weight loss in the 6 months preceding the survey concerned 77.55% patients, 30.61% of whom were severely malnourished. Albuminemia and the Nutritional Risk Index (NRI) showed that respectively 13.5% of the patients were malnourished and 22.5% of patients were at risk of complications related to undernutrition. In 18.87% of cases, surveyed patients had taken less than three meals a day. Therefore, prevalence of undernutrition/malnutrition was high in the study population. No single parameter was sufficiently sensitive and specific. Based on this, the combination of several parameters is necessary for an objective assessment for intervention. Nutritional management of patients living with cancer deserves to be integrated into the overall therapeutic project.
Key words: Nutrition, cancer, undernutrition, nutritional assessment, food intake.
INTRODUCTION
Cancer is a real public health issue and a leading cause of death in the world. The World Health Organisation (WHO) estimated 14.1 million new cases of cancer worldwide and 8.2 million deaths from cancer in 2012, compared to 12.7 million and 7.6 million, respectively, in 2008 (Ferlay et al., 2015).
In Côte d'Ivoire, adjusted data from the Abidjan Cancer Registry from 2007 to 2011 showed 4533 new cases during these five years and 80% are discovered at an advanced stage involving the completion of heavy and very expensive treatments and a high mortality rate of 88%. Although it is recognized that there is an increase of cancer in the world, and more particularly in Côte d'Ivoire, it is linked to population growth and the development of diagnostic or screening capacities that is also likely to result from increased exposure to some behavioral or environmental risk factors, which are multiple and sometimes entangled.
In cancer patients, nutritional care is required. Indeed, cancer cells, through some mediators, induce major metabolic changes in patients’ body. In addition, anti-cancer treatments cause additional metabolic stress (Bernstein et al., 1985).
All these changes can impact nutritional and energetic needs. States of extreme malnutrition and weight loss (undernutrition) are often observed (Schneider, 2004).
Undernutrition and malnutrition in cancer patients are so commonly associated with tumor disease that it is often considered an integral part of the cancer evolution and therefore trivialized. However, it is admitted that many cancer patients die from cachexia and that malnutrition limits the tolerance and efficacy of treatments. The prevalence of malnutrition in patients with cancer has been reported to range from about 20% to more than 70% in worldwide studies, with differences related to patient age, cancer type, and cancer stage (Arends et al., 2017).
Here, we must first solve the problem of rigorous evaluation, providing relevant data that will inform decision-making through the development of nutritional policies that guarantee health for all.
Nutritional assessment is the best way to determine whether people's nutritional needs are being met once food is available and accessible (FAO, 2019).
Nutritional assessment provides timely, quality and evidence-based information to set goals, plan, monitor and evaluate programs to eradicate hunger, reduce the scourge of malnutrition in populations in general and undernutrition in sick subject particularly.
Thus, free and global access to country information on food and nutrition strengthens decision-making to achieve better nutrition for all (FAO, 2019).
This study mainly aimed to assess undernutrition in cancer patients in Côte d'Ivoire at the cancer service of the University Hospital of Treichville. Specifically, it was about conducting a nutritional survey in cancer patients by the determination of anthropometric, biological parameters as well as nutritional indexes and dietary intakes parameters to realize an intervention project.
METHODS
Survey: Collection of socio-demographic and clinical data
This involves a descriptive and analytical cross-sectional study, which took place from November 5th to December15th 2015 in the Cancer service of the University Hospital of Treichville in Abidjan (Côte d'Ivoire) and in the Care unit for cancer patients called "Bona Dona Oncology Center (COBA)" located in Treichville, a municipality of Abidjan. Our study population included fifty-three (53) patients. The inclusion criteria were patients ≥ 16 years, followed for cancer, hospitalized or not, and receiving oral, enteral or parenteral nutrition. Exclusion criteria were unconscious patients or those who refused to participate in the survey. We had a form (in Appendix) developed as a direct or semi-direct questionnaire which, according to the items, have been sent to patients or relatives, medical and hospital catering staff (if necessary). With this form, socio-demographic and clinical data as well as information about the ingesta of the previous 24 h (recall of the 24 h) were collected. The interrogation occurred either during medical consultations with physicians, or in an annex room where patients were referred by oncologists, or at the patient's bedside for inpatients and outpatients in chemotherapy. Socio-demographic data comprised age, sex, professional status, area of ​​residence, etc.
Clinical data were based on information collected from the attending physician: Personal and family history of the patient, the tumor site, the progressive stage of the disease (loco-regional or metastatic), the existence of factors favoring a reduction of food intake (infectious syndrome, digestive disorders, sensory disturbances, debilitating pain, etc.) as well as the treatment in progress or already received.
Determination of nutritional status
This biometric part was performed in order to identify the current anthropometric and biological measurements (weight, size, body mass index (BMI), albumin) of patients for the assessment of their nutritional status.
All subjects were systematically weighed using an electronic scale. The size was measured with a toise for patients walking easily or collected by healthcare assistants on identification documents for patients who were very bedridden, hospitalized or in chemotherapy. Information about previous weight was noted if available. Samples for electrophoresis of proteins, for albumin dosage, were carried out only after patients and relatives’ agreement, by a biologist hired for the survey. All samples were analyzed at the "Laboratory of Medical and Biological Analysis of Arras", located in Treichville, for the electrophoresis of serum proteins, mainly for albumin. The following parameters have been entered:
i) The anthropometric measurements concerning the current weight (kg) and the patient’s weight 6 months before;
ii) The percentage of weight loss over the 6 months preceding the evaluation according to the formula:
Percentage of weight loss = [Usual weight - current weight / Usual weight] × 100
Body Size (m) and Body Mass Index (BMI) in kg / m2 according to the formula:
BMI = Weight (kg) / Size² (m)
Biological data (albuminemia) was collected from electrophoresis of serum proteins. A blood sample in a red tube was performed by a technician in all consenting enrolled patients either after the consultation or at the patient's bedside for hospitalized patients or for patients in chemotherapy. A label with an anonymity number for each patient was affixed to each tube. All the tubes of the day were placed on a rack and sent to the laboratory for analysis.
Also, nutritional score which refers to Buzby index or Nutritional Risk Index (NRI) has a prognostic value in assessing the nutritional risk of patients that has fully been validated. It is calculated as follows:
NRI= (1.519 × albumin, g/l) + 41.7 (current weight / usual weight) × 100 (Buzby et al., 1980).
Clinical undernutrition was defined as either BMI ≤ 18.5 kg/m2 in adults <75 years; BMI ≤ 21 kg/m2 for subjects over 75 years, or weight loss >10% in 6 months, regardless of BMI. This clinical malnutrition was considered severe when the BMI was <17 kg/m2. According to the Buzby index, malnutrition was determined by an NRI <97.5. This undernutrition was called severe when the NRI <83.5.
Assessment of last 24 h food intake
An inventory of food intake from breakfast, lunch, dinner and snacks was made for each patient. During this interrogation, the ingested amounts (1/4, 2/4, 3/4, 4/4) were specified for most patients and the composition of meals provided useful information for further intervention case by case.
Statistical analysis
Database was established from the Epi Info software. Data analysis was carried out using the software R and the significance test according to Fisher test, was at 5% threshold (p< 0.05). To explore the relationship between weight change and blood albumin level (albuminemia) or the association between tumor stage and albuminemia, Fisher test was also performed to determine variables and interactions which remained significant (P < 0.05).
RESULTS
Socio-demographic and clinical data
The mean age of our study population was 51 years with extremes ranging from 24 to 76 years. A relatively young population, say about 50% of patients were under 50. This poses real development issues because of disability caused by cancer for a segment of active population.
There was a strong female predominance (86.79%) due to a high prevalence of women's cancers in the cancer patient population (Table 1). The early detection means increasingly available for certain types of cancer (breast, cervix) through activities of the National Cancer Control Program in Côte d'Ivoire and NGOs.
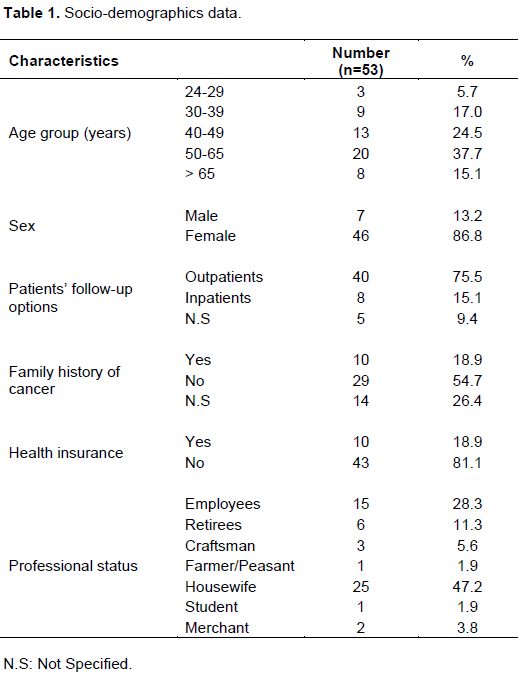
Most patients (≥ 75%) were not hospitalized. However, it could be noted that 50% of them had a day hospitalization, which could reach 24 h in few cases for chemotherapy treatment. Heredity factor of family history of cancer accounted for 18.87%. These results could provide a profile of populations at risk of developing a cancer and requiring primary prevention measures.
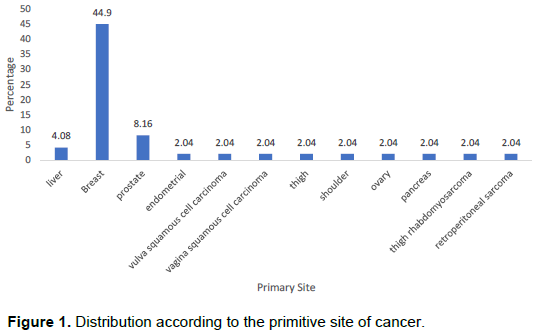
Distribution according to the primitive site of cancer
Breast cancer with a rate of about 45% was the most common cancer, followed by cervix cancer with 16.33% and prostate cancer 8.16%. The mobilization of cancer NGOs around breast cancer and the availability of powerful diagnostic tools such as immunohistochemistry have favored a high prevalence of this cancer (Figure 1).
Nutritional parameter
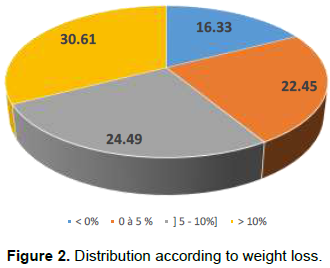
Distribution according to the percentage of weight loss
The percentage of weight loss was evaluated over the 6months preceding the survey with severely malnourished patients reaching 30.61% (Figure 2).
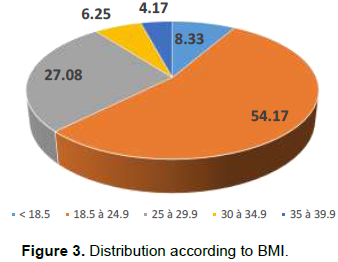
Distribution by body mass index (BMI)
According to this parameter, malnourished patients accounted for only 8.33%. Further, there was a significant percentage of overweight patients (27.08%) and obese ones (10.42%) (Figure 3).
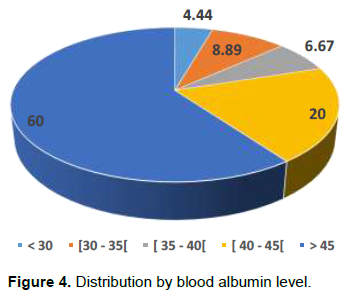
Distribution according to albuminemia
Malnourished patients according to the serum albumin level (albuminemia <35 g/l) accounted for 13.5% from whom 33% were severely malnourished. 60% of patients had albumin >45 g/l (Figure 4).
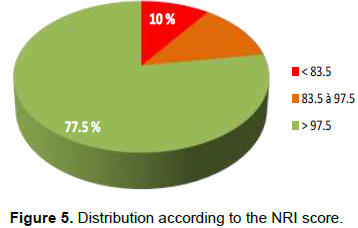
Distribution according to the Nutritional Risk Index (NRI)
Calculation of the nutritional risk index established that 22.5% of patients in our study population were malnourished, from which 45% were severe malnutrition. Meanwhile, nearly 77.5% of patients had no risk of undernutrition (Figure 5).
Bivariate models analysis
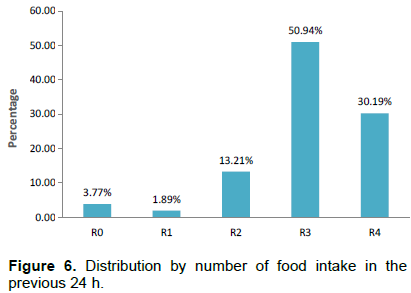
Distribution according to the number of food intake in the previous 24 h (24-h recall)
It is found that more than 80% of patients took at least 3 meals the day before the survey. It is difficult to extrapolate this result to the usual number of patients' daily meals because half (50%) of these patients had a form of anorexia. However, as a prelude to the chemotherapy they were going to receive the next day, these patients strove to take meals in order to better withstand the side effects of anticancer drugs (Figure 6).
Food diversity based on the 24-h recall
Here, we used the individual dietary diversity score (IDDS) as proposed by FAO and based on fourteen (14) food groups such as cereals (1), tubers and white plantains (2), dark green leafy vegetables (3), veggies and vegetables rich in Vitamin A (4), fruits rich in Vitamin A (5), oils and fats (6), other vegetables (7), other fruits (8), giblets (9), meats and poultry (10), fish and seafood (11), eggs (12), legumes, nuts and seeds (13), milk and milk products (14).
The more the diet is diversified (high number of food groups consumed), the better is its quality. It is apparent from the analysis of the results that the dietary diversity score varies between 1 and 7 with an average of 4 ± 1.49.
The most consumed foods, a day before the surveywas cereals (rice 90%, millet, etc.), consumed by 90% of the population. Tubers and white plant roots were consumed by 65% ​​of the study population, while groups of fish and seafood and other vegetables are respectively consumed by 55% of patients. On the over hand, the consumption of some foods such as milk and milk products and vegetables rich in vitamin A remained very low (Figure 7).
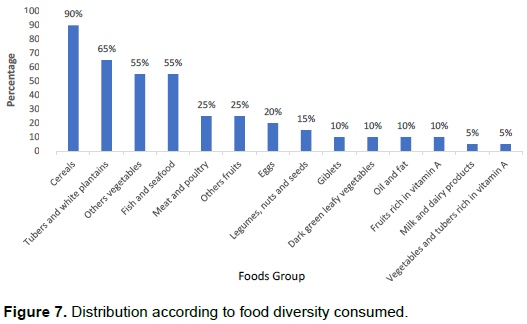
Figure 7 shows a distribution of patients into two (2) categories according to the dietary diversity score, that is, patients with a low level of diversity which means having consumed between 1 and 4 food groups (IDDS ‹ 4) and patients with acceptable diversity levels who consumed between 5 and 7 food groups (IDDS ≥4). Thus, our results showed that 70% of patients had a low level of diversity vs 30% with a high level of dietary diversity.
DISCUSSION
The high prevalence of women cancers in our study (87%) is justified by the intensification of prevention and control of breast and cervix cancers (awareness campaign on breast self-examination, opening of a sinology unit for almost free explorations at Treichville University Hospital and caravans for precancerous lesions of the cervix). Prostate cancer (8.16%) followed cervix (16.33%) and breast (44.90%) cancers in terms of frequency of occurrence in our investigation. It should be noted an increase in the prevalence of adult obesity from 2008 (6,2%) to 2016 (10,3%) in Côte-d’Ivoire (CIA World Factbook, 2017). Obesity is associated with a significant risk of developing hormone-dependent cancers such as prostate and breast cancer (Key et al., 2001). These results are like those obtained by the Abidjan Cancer Registry in its 2012 to 2013 biennial report (Abidjan Cancer Registry. Data 2007-2011) which recorded 2479 new cases of cancer including 956 cases in men and 1523 cases in women, distributed as follows for the mentioned organs: breast cancer 531 cases, 21.42%, cervix cancer 280 cases, 11.29% and prostate cancer 252 cases, 10.16%. The issues of undernutrition and malnutrition in cancer patients first raised the question of their screening and assessment. To date, there is still no formal consensus in the nutritional assessment of cancer patients. However, analysis of some parameters such as weight loss, BMI, albumin and NRI score have allowed many authors to identify patients who are malnourished or at risk of undernutrition (Senesse and Vasson, 2012). 30.61% of patients with severe malnutrition were objectified from the percentage of weight loss (% weight loss > 10% or even 15%) in the previous six months before the survey. Some patients were unable to report their usual reference weight because of a mild cognitive deficit, although some of them were convinced that they lost weight from the clinical expression of the cancer to the day of the survey. Apart from tumor disease, the patient's weight loss is also linked to socio-economic issues (loss of financial autonomy and inaccessible treatments) or psychological (return to parents’ home and lack of self-esteem) or pathological (depression).
According to BMI, undernutrition affected 8.33% of patients (BMI <18.5). However, and unlike weight loss, BMI is a static criterion for nutritional assessment. BMI showed 27.08% of overweight patients and 10.42% of obese patients. In fact, BMI tends to mask chronic undernutrition not only in patients with edema or ascites, but especially in overweight or obese patients. Among these patients, even more than 10 to 15% of unintentional weight loss that occurred had no influence on their BMI reference (before any involuntary weight loss related to cancer). In our study, less than 10% of patients with breast cancer had a BMI <18.5, while weight loss was 75%. These data are comparable to those obtained by Sanz-Ortiz et al. (2008). Indeed, in the prospective multicenter observational study, conducted by Sanz-Ortiz et al. (2008), 561 patients mainly with head and neck cancer, aerodigestive tract and lung were assessed.
Undernutrition was observed in relation to BMI for 18.2% of patients while weight loss involved 90.7% of patients.
Finally, having a BMI greater than 24.9 (overweight or obesity) does not protect against undernutrition. 37.5% of patients had a BMI> 24.9 while weight loss was observed in 77.55% of them. These results were like Pressoir et al. (2003) results. Their works were conducted in cancer centers where 38.8% of patients with a weight loss identified in the six months preceding the assessment had a higher BMI or equal to thirty (30).
Another widely used and validated parameter in the nutritional assessment of patients is albuminemia (serum albumin level). Albumin is the most abundant serum protein (35-50 g/L) and an insufficient protein supply may be harmful (Stobäus et al., 2015) especially now that we are well aware of the prognostic importance of sarcopenia (Baracos and Kazemi-Bajestani, 2013; Raynard et al., 2017) which transports many endogenous or exogenous compounds (fatty acids, bilirubin, minerals, etc.). It is moreover, responsible for 80% of the oncotic pressure.
Its renewal rate, essentially hepatic, is rather slow and its elimination takes place in the digestive tract, kidney and liver. Its long half-life (20 days) and its distribution between the vascular sector (40% in healthy subjects) and the interstitial area (60%) limit the specificity of albumin as a marker of nutritional assessment. We obtained 13.5% of undernourished patients (albuminemia <35 g/L) compared with the blood albumin level of the patients evaluated. These values ​​ do not reflect the degree of malnutrition of our study population objectified by the kinetics of weight loss. 60% of patients had albumin levels above 45 g/L, of which 50% had hyperalbuminemia (albumin ≥ 60 g/L). This phenomenon was observed in most chemotherapy patients who received blood transfusion less than 12 to 24 h prior to the assessment. The influence of the treatment including paclitaxel, a cytotoxic chemotherapeutic agent extracted from western yew (Taxus brevifolia), combined with albumin particles, called "nab-paclitaxel (nanoparticle albumin-bound paclitaxel)" on the blood albumin level of patients remains to be studied too. The parameters of these transfused patients compared to the serum albumin level are not interpretable (significant bias). In addition, the sensitivity of albuminemia and its specificity in the screening or assessment of undernutrition remains debatable.
After the Second World War, the University of Minnesota conducted an experiment on food restriction. The purpose was to measure physiological and psychological effects of starving and to draw conclusions to assist victims. Thus, 32 subjects were subjected to a six-month dietary restriction providing half of their nutritional needs. The results showed a weight loss of more than 25% while albuminemia varied only from 43 to 40 g/l (Friedman and Fadem, 2010). These results corroborated what is observed, for instance, in anorexia nervosa, during chronic undernutrition there is a body adaptation that results in preservation of the protein mass and albumin. Thus, the decrease in nutritional intake, to some extent, does not impact albumin. It is likely that in these situations of chronic undernutrition, the amino acids required for albumin synthesis come from hepatic proteolysis via the lysosomal-dependent system (Vom Dahl and Häussinger, 2014).
In this study, patients with serum albumin <30 g/L (30% of malnourished patients according to serum albumin level) were hospitalized with impaired general health status (reduced dietary intakes, pain, anorexia) that are life-threatening. A case of death in one inpatient has been reported by the nursing staff 48 h after its assessment. At the analysis, this patient had severe hypoalbuminemia. His albumin level was 26.5 g/L with a BMI at the normal limit. Indeed, according to a meta-analysis gathering 90 studies and 291,433 patients, the risk of death increased by 137% for each loss of 10 g/L of albumin. It was noted that 15 studies in this meta-analysis found a significant association between mortality risk and hypoalbuminemia. Hypoalbuminemia, regardless of nutritional status, reflects a risk of morbidity and mortality (Vincent et al., 2003). In fact, hypoalbuminemia is defined as a prognostic factor for morbidity and mortality in hospitalized patients (Harvey et al., 1981). Thus, albuminemia is more specific for the risk of morbidity and mortality associated with undernutrition rather than for undernutrition itself.
A composite nutritional assessment criterion, the Nutritional Risk Index (NRI) was used as a method of assessing the risk of complications related to the nutritional status in cancer patients. The main advantage of NRI is to be able to correct the imperfections of each factor (albumin and weight loss) by combining them. NRI therefore has a positive predictive value for identifying patients at risk for complications, particularly infections (Kyle et al., 2005). In our study, 22.5% of cancer patients were found to be at risk of infectious complications, morbidity and mortality related to malnutrition due to NRI. These results were in fact underestimated because of the hyperalbuminemia (albuminemia ≥ 60 g/L) found in several transfused patients (20% of the evaluated patients) less than 12 h before the evaluation whereas in more than 60% of these patients, the rate of weight loss revealed a state of severe undernutrition, predictive of hypoalbuminemia or albumin levels within the limits of normal.
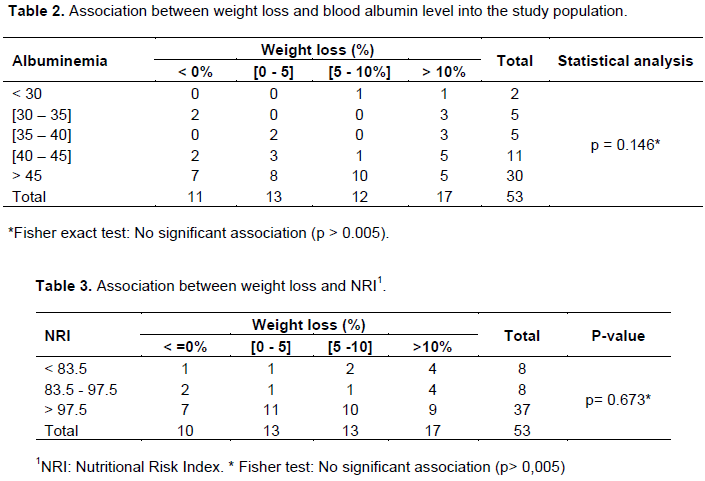
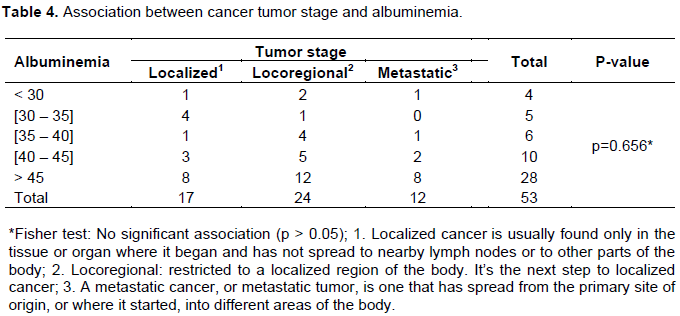
Some bivariate models were performed, and no significant association was found between patient’s weight loss and albuminemia or NRI as well as tumor stage versus albuminemia (Table 2, 3, 4). The lack of association may be explained by the small number of subjects in the relatives’ numbers. This was the primary limitation of this study. However, the small sample size allowed us to perform a more comprehensive and integrative approach when evaluating the nutritional status of these patients.
The number of food intake, food diversity consumption and the individual dietary diversity score (IDDS) have been assessed. The low dietary diversity could be explained by food aversions that can also develop as a result of a perceived link between an unpleasant event (adverse effect of treatment for example) and the ingestion of a type of foods (Van Cutsem and Arends, 2005). Meanwhile, patients whose number of food intake was better (four times), about 30% in the study population, had a better level of IDDS (IDDS › 5) compared to those which has standard number of food intake (3 times) or less (1 or 2 times) with an IDDS ≤ 4.
The improvement of the individual dietary diversity score in patients could be related to the number of daily food intake of the patient, except for any situation of food shortage or food insecurity. A better level of IDDS (IDDS › 7) could bring to the population, the most essential nutrients to improve their quality of life, reducing mortality and complying with treatments (Drescher et al., 2007).
CONCLUSION
The nutritional status in cancer patients in Côte d'Ivoire is marked by an acute undernutrition, characterized by significant unintentional weight loss in most patients. The assessment of nutritional status remains a major issue because there is no absolute diagnostic criterion or "gold standard". It must therefore always include a clinical aspect, associated with anthropometric measurements, supplemented by a biological or even biophysical exploration for a more precise and objective evaluation.
The assessment of nutritional status must be integrated during the disease announcement. Depending on this assessment outcomes and the scheduled oncology treatment, a specialized consultation should be requested. Adapted nutritional cares must be provided to cancer patients.
FUTURE OUTLOOK
In developing countries and in the case of Côte-d’Ivoire, the triple burden of undernutrition/malnutrition, poverty (50% of the patients in this study were without fixed incomes and 80% uninsured) and weakness of the technical platform, despite the dedication of caregivers, remain major challenges of public health and research. This requires special attention from decision-makers (public authorities and donors) and the general population through prevention and control means adapted to the socio-economic status of population. To achieve this, the establishment of a local food table made of products rich in antioxidants, polyphenols and other nutritional substances which are indicated in the prevention and reduction of cancer-related morbidity and mortality is essential.
CONFLICT OF INTERESTS
The authors have not declared any conflicts of interests.
ACKNOWLEDGEMENTS
The authors are grateful to the authorities of University Hospital Centre of Treichville in Abidjan (Côte d'Ivoire) and the Care Unit for Cancer Patients called "Bona Dona Oncology Center (COBA)" who give authorization to do this study.
The authors also appreciate all the participants in this study, medical staff and their patients as well as Prof CASANELLI D’Istria, Medical and Scientific Director of the University Hospital Centre of Treichville for the supervising of the ethical side of the study.
REFERENCES
|
Arends J, Baracos V, Bertz H, Bozzetti F, Calder P, Deutz N (2017). ESPEN expert group recommendations for action against cancer-related malnutrition. Clinical Nutrition 36(5):1187-1196. |
|
|
Baracos V, Kazemi-Bajestani SM (2013). Clinical outcomes related to muscle mass in humans with cancer and catabolic illnesses. The International Journal of Biochemistry & Cell Biology 45:2302-2308 |
|
|
Bernstein I, Treneer C, Kott J (1985). Area postrema mediates tumor effects on food intake, body weight, and learned aversions. American Journal of Physiology 249:296-300. |
|
|
Buzby GP, Mullen JL, Matthews D C (1980). Pronostic nutritional index in gastrointestinal surgery, The American Journal of Surgery 139:160-167. |
|
|
CIA World Factbook (2017). Obésité en Côte-d'Ivoire - Taux de prévalence chez les adultes. |
|
|
Drescher LS, Thiele S, Mensink GBM (2007). A New index to measure healthy food diversity better reflects a healthy diet than traditional measures. The Journal of Nutrition 137:647-651. |
|
|
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F (2015). Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. International Journal of Cancer 136(5):E359-86. |
|
|
Food and Agriculture Organization (FAO) (2019). Food and Agriculture Organization of the United Nations. |
|
|
Friedman AN, Fadem SZ (2010). Reassessment of albumin as a nutritional marker in kidney disease. Journal of the American Society of Nephrology 21:223-230. |
|
|
Harvey KB, Moldawer LL, Bistrian BR, Blackburn GL (1981). Biological measures for the formulation of a hospital prognostic index. The American Journal of clinical nutrition 34(10):2013-2022. |
|
|
Key TJ, Verkasalo PK, Banks E (2001). Epidemiology of breast cancer. The lancet Oncology 2(3):133-140. |
|
|
Kyle UG, Schneider SM, Pirlich M, Lochs H, Hebuterne X, Pichard C (2005). Does nutritional risk, as assessed by Nutritional Risk Index, increase during hospital stay? A multinational population-based study. Clinical Nutrition 24(4):516-524. |
|
|
Pressoir M, Desné S, Berchery D, Rossignol G, Poiree B, Meslier M (2003). Prevalence, risk factors and clinical implications of malnutrition in French Comprehensive Cancer Centres. British Journal of Cancer 102(6):966-971. |
|
|
Raynard B, Hebuterne X, Goldwasser F, Ait AH, Dubray PL, Barthelemy P, Rosso E, Phoutthasang V, Bories C, Digue L, Laharie D (2017). Crossed perceptions about malnutrition in patients and their doctors in oncology. Bulletin du cancer 104(11):921-928. |
|
|
Registre du Cancer d'Abidjan. Données de (2007 à 2011). |
|
|
Sanz Ortiz J, Moreno Nogueira JA, García de Lorenzo, Mateos A (2008). Protein energy malnutrition (PEM) in cancer patients. Clinical and Translational Oncology 10(9):579-582. |
|
|
Senesse P, Vasson M P (2012). Nutrition chez le patient adulte atteint de cancer : quand et comment évaluer l'état nutritionnel d'un malade atteint de cancer ? Comment faire le diagnostic de dénutrition et le diagnostic de dénutrition sévère chez un malade atteint de cancer ? Quelles sont les situations les plus à risque de dénutrition ? Nutrition Clinique et Métabolisme 26:165-188. |
|
|
Stobäus N, Müller MJ, Küpferling S, Schulzke JD, Norman K (2015). Low recent protein intake predicts cancer-related fatigue and increased mortality in patients with advanced tumor undergoing chemotherapy. Nutrition and Cancer 67(5):818-824. |
|
|
Van Cutsem E, Arends J (2005). The causes and consequences of cancer associated malnutrition. European Journal Oncology Nursing 9(2):51-63. |
|
|
Vincent JL, Dubois MJ, Navickis RJ, Wilkes MM (2003). Hypoalbuminemia in acute illness: is there a rationale for intervention? A meta-analysis of cohort studies and controlled trials. Annals of Surgery 237(3):319-334. |
|
|
Vom Dahl S, Häussinger D (2004). Role of amino acids in the control of proteolysis. In: Cynober L editor. Amino Acid Metabolism and Therapy in Health and Disease. Boca Raton CRC Press pp. 275-289. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


