Full Length Research Paper

ABSTRACT
Family members also known as Patients’ Guardians (PG) are involved in caring for acutely ill inpatients in Malawian hospitals. Family participation in caring for acutely ill adult inpatients is adopted from the Family Centred Care approach. Using a focused ethnographic approach, we explored the perspectives of PGs and nurses on the burden of the caring role on PGs and their adaptation. Twelve PGs and eight nurses were purposively sampled to participate in the study. Data collection was done using participant observation, and in-depth interviews. Nvivo 12 software was used for coding and categorising data into themes that emerged. The findings were analysed using Spradley’s Developmental Research Strategy. Three cultural domains emerged from the findings of this study: PG diverse roles and responsibilities, PG burden to the caring role and coping with the caring role. Nurses should effectively assess PGs’ ability to cope with the caring role to facilitate their adaptation.
Key words: Patient’s guardian, family centred care, caring role, adaptation.
INTRODUCTION
Family members commonly known as patients’ guardians (PG) are a familiar sight in Malawian hospitals. This study provides a nursing perspective to a hospital with shortage of nurses in a developing sub-Saharan African country that strives to offer quality care to inpatients by involving PGs.
Family participation in caring for acutely ill adult inpatients has been adopted from the Family Centred Care (FCC) approach. FCC is a partnership approach to healthcare decision making between the family and healthcare provider (Festini, 2014). The principles of FCC are information sharing, respect and honouring of differences, partnership and collaboration and negotiation (Kuo et al., 2012). Due to the benefits of FCC, various healthcare institutions have adopted the practice in acute care adult inpatient settings (Coyne et al., 2013; Ewart et al., 2014; Khosravan et al., 2014; Mackie et al., 2018). Although healthcare institutions have adopted FCC approach in inpatient care, its implementation has been problematic and inconsistent worldwide (Coyne, 2013). Their role in the healthcare delivery system is not stipulated. There is no policy or guidelines that regulate the involvement of PGs to offer care to acutely ill adult inpatients. PGs are sometimes left to do technical aspects of care that require special skills like wound dressing, NGT feeding, monitoring medication and suctioning with neither support nor training nor supervision by HCWs. They are sometimes regarded as a burden to the healthcare delivery system because they overcrowd the hospital and do not know what to do (Hoffman et al., 2012).
The problem is, involving PGs to care for acutely ill surgical inpatients without any preparation inevitably distorts the dynamics of the family unit and leads to a substantial burden on the PG and their families. The extent of such burden is difficult to assess and therefore remains unrecognised by HCWs. This requires a contemporary model of healthcare delivery that may facilitate the family as a system to adapt to the illness of its member. The findings of the study will provide an insight into the experiences of PGs when involved in caring for surgical inpatients. There is limited research on the burden of the caring role on PGs in acute healthcare settings and how family members adapt to such burden. This study aimed to explore the insider views of PGs and nurses on the burden of the caring role on family members who are involved in caring for surgical inpatients at a tertiary hospital in Malawi and their adaptation to the burden of the caring role.
METHODOLOGY
The study was conducted between June 2019 and July 2019. A focused ethnographic approach was used to generate both etic and emic views of the cultural portrait of PGs and nurses in the surgical wards (Cresswell, 2013; Goodson and Vassar, 2011). The participants in this study, especially the PGs would not know each other, although it was assumed that they shared a culture. The focus was on their common behaviour and shared views and experiences in their involvement in caring for adult surgical inpatients in the wards (Wall, 2014).
The study was conducted in adult surgical wards at a tertiary and teaching hospital in Malawi because surgical inpatients require highly specialised care for a short period, preoperatively and postoperatively (Brunner, 2010).
The study population comprised PGs and nurses who were involved in caring for acutely ill adult inpatients in male and female surgical wards. The non-probabilistic purposive sampling method was used to recruit participants for the study based on the inclusion and exclusion criteria.
The following were the inclusion criteria for PGs: being 18 years and above, looking after inpatients in the male or female surgical wards, being in the hospital with the patient for at least 24 consecutive hours and not more than 10 days, and those looking after stable patients. The following PGs were excluded from the study: those whose patients have died or are not stable, someone looking after patients in high dependency unit (HDU) or paediatric units, and not being fluent in either English or Chichewa. Qualified nurses who had worked in the surgical unit for at least one month at the time of the study were included: locum nurses and student nurses working in the surgical wards were excluded from the study. The participants were 12 PGs and 8 nurses. Data saturation determined the sample size.
Data were collected through participant observation and in-depth interviews. Participant observations were conducted in the surgical wards during normal day shifts (from the beginning of a shift at 07:30 to the end at 16:30) because most of the nursing care activities were done during this time. At the beginning of the study, the researcher started with a descriptive observation to understand the routines and norms of the wards and to get an orientation of the setting, the people, and the events that occurred in the wards.
After familiarization, the researcher planned for structured participant observations. Key informants were identified and the researcher developed a rapport with them. Each participant was observed for a minimum of three consecutive day shifts. During observation, the researcher was actively engaged in the activities that were happening in the ward. A checklist for observation was developed by the researcher based on information provided from the researcher's clinical experience in the hospital settings, the scope of practice of nurses, and nursing textbooks and research articles. This guided the focus of the observations. The content of the checklist focused on the activities that PGs performed, behaviour, attitude, and social interaction with nurses and other HCWs, and information shared with nurses.
Field notes were taken immediately after observing an event. These were later on written more formally with personal reflections and formed a basis of follow-up interviews as questions emerged from what was being observed (Thomson, 2011). The researcher conducted in-depth interviews after observing a participant. PGs were interviewed on discharge or a day before discharge. A semi-structured interview guide was used to discover the insider perspectives of PGs and nurses. All participants were asked the same guiding questions but the direction of the interview changed depending on what was being discussed by the interviewee. Interview techniques were adopted from Spradley (2016a)to confirm and verify data. Each interview took approximately 30 min and was audio-recorded. The nurses were interviewed in both English and Chichewa while PGs in Chichewa because most of the PGs were fluent in Chichewa. At the end of each interview, a summary of the issues that were discussed was made to increase the credibility of the study, (Lincoln and Guba, 1985)and to guide the next interviews.
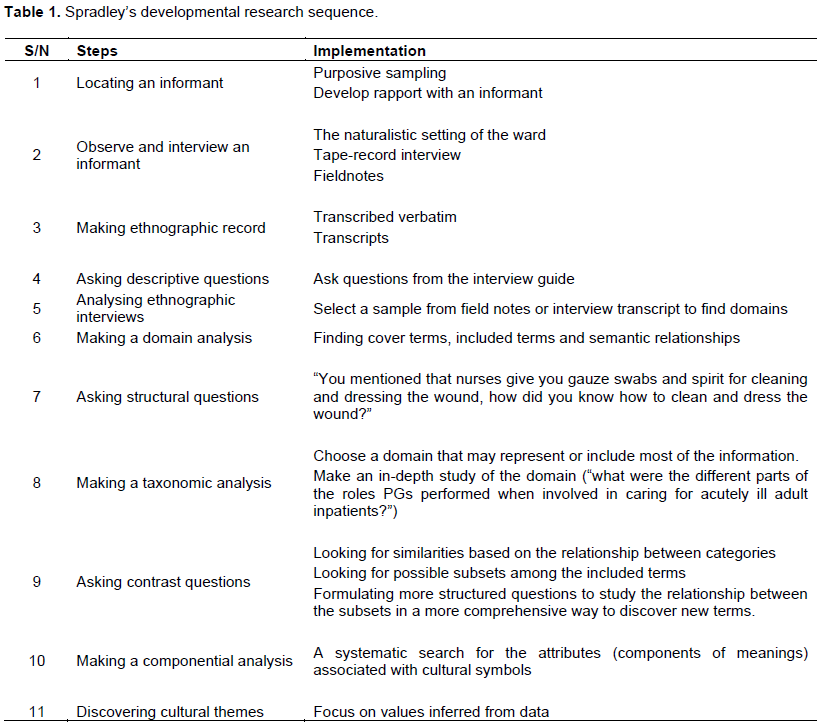
Data analysis was done concurrently with data collection (Elo et al., 2014). Spradley’s Developmental Research Sequence (DRS) method of ethnographic data analysis (Spradley, 2016a, 2016b)was used to analyse data collected from the triangulated data collection methods. The researcher organised the cultural domain of the surgical wards by firstly, describing the cultural scene, the people, and the events that occurred naturally in the wards.
The audiotaped interviews and field notes were transcribed verbatim soon after the interviews to capture all the data that emerged. We then transferred the transcribed data into Nvivo 12 software for coding, then categorising according to the data and themes that emerged from the categories (Polit and Beck, 2017). The analysis used the following steps as described by Spradley’s DRS (1976): domain analysis, taxonomic analysis, componential analysis, and theme analysis (Spradley, 2016b)as illustrated in Table 1.
The study received ethical approval certificate number P.03/19/ 2624. Permission was granted from Kamuzu Central Hospital Research Committee to conduct the study at the institution. Informed consent was obtained from all participants.
RESULTS
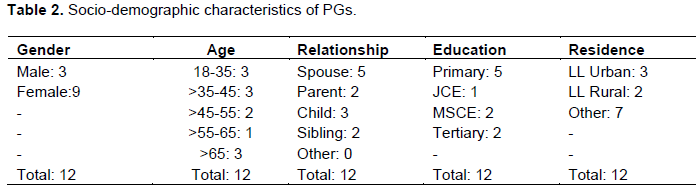
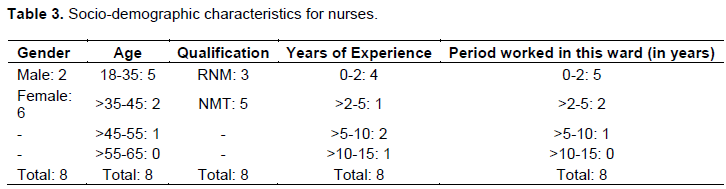
Tables 2 and 3 present the socio-demographic characteristics of the participants.
Cultural domains/themes
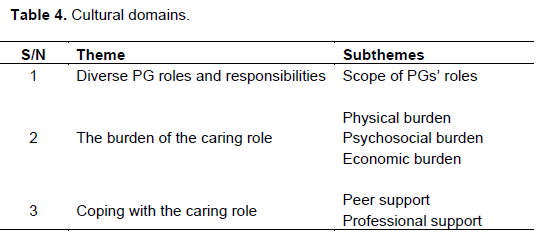
Three cultural domains also known as themes were discovered from the triangulated data collection methods as outlined in Table 4.
PG diverse roles and responsibilities
The findings of this study revealed that PGs were involved in providing inpatients with physical, psychosocial, and spiritual care. Physical care roles included basic and technical roles. PGs performed the following activities to assist their patients to meet their activities of living (AL) because they could not do the activities independently.
[…].. I bathe her in bed because she had an operation so she is unable to walk or get out of bed on her own. After bathing her, I change her clothes and beddings then I give her food […] (PG 10).
PGs also offered technical aspects of care that required some technical knowledge and expertise for one to perform them accurately.
PGs do a lot of things […]draining their {patients} urine from urine bags if they have a catheter on, feeding them, some via NGT or orally or just to make sure that they have food and that they have eaten if they don't need to be fed, helping them to ambulate especially after the op (NP 2).
PGs performed some activities to meet the psychosocial needs of their patients. These included psychosocial care, advocacy, and spiritual care roles. PGs advocated for their patients to ensure that they received quality care.
Sometimes when the patient is complaining about pain, I go to inform the doctor [nurse] to come and provide some medication (PG 8).
They were also involved in performing some religious activities. PGs protected their patients' religious beliefs while in hospital by ensuring that healthcare professionals adhere to their religious beliefs while providing care.
Sometimes we share the word of God with our patients and other guardians (PG 8).
I also make sure that the nurses don't give him blood because it is not allowed in our religion. They said he wanted blood during the operation but I spoke to the doctors to make sure that does not happen (PG 4)
The burden of the caring role
The findings of this study revealed that the caring role has physical, psychosocial and economic burdens on the PGs.
The physical burden of the caring role
The physical impact of the caring role has been categorised into three: poor health status, safety risk and lack of infrastructure and resources for PGs. This includes the physical signs and symptoms that PGs manifested during the time they assumed the caring role.
Some guardians come here to complain about general body pains, headache or backache, and they think they might have malaria, but you see them looking exhausted because they look after their patients day and night without resting (NP 7).
The hospitals are designed to accommodate patients only and not each with a guardian, this leads to overcrowding.
The wards become too congested and overcrowded with patients and their guardians; this can be a good source of transmission of airborne diseases. And when it’s visiting time, we don’t limit the number of visitors per patient and the wards are very overcrowded (NP 8).
PGs’ lack of knowledge of infection prevention principles and nurses’ inability to support or supervise PGs in some of the roles that they perform may lead to transmission of nosocomial infections.
We see some guardians taking their patients to the bathroom without wearing shoes, that place is very dirty and risk for many infections and some guardians touch surfaces with used gloves, we don’t have time to supervise what they do when they wear those gloves, one day if there will be an outbreak here, everyone in the ward will be infected (NP 4).
PGs were also prone to physical injury due to a lack of knowledge on how to perform certain roles.
Sometimes guardians turn their patients, and our beds are short so they bend themselves excessively and twist their backs and end up complaining of backaches (NP 6).
The physical design of the wards does not accommodate PGs, hence during the night, they slept on the floor that was cold and uncomfortable or sat on the bed throughout the night if their patients needed close monitoring.
[…]there is no place for a guardian to sit or rest, we sit on the bed where the patient is sleeping, we sleep on the floor. My whole body is very sore and I have not slept since I came here, so it’s not an easy thing to do[…] (PG 10).
The welfare of PGs was neglected although they offered care to patients just like other professional caregivers. Hospital authorities do not provide PGs with necessities like food and beddings although they are involved in providing care to inpatients.
[…] they have needs like all caregivers, we fight for better working conditions for nurses as caregivers but not for guardians, some stay without food or beddings because the hospital only provides for patients, maybe because no policy talks about them although we work with them (NP 8).
The psychosocial burden of the caring role
PGs take up their new caring role in an unfamiliar environment with no preparation. Their involvement in inpatient care is unplanned and this affects their psychosocial well-being.
They are in an unfamiliar environment where everything looks strange, they are also scared of other patients’ conditions, there are just too many issues there why they are afraid, maybe we also need to ask them. But that is my observation anyway (NP 8).
PGs described their emotional experiences in various ways. Some described the experience as “not easy” and “hard”.
It’s hard for me to see my mother helpless. So I just have to be there for her and help her where possible. The first time I bathed my mother was very hard for me, I just have to sacrifice myself for the sake of my mother […] (PG 10).
The caring role was described as “overwhelming” and “emotionally draining”.
The guardians are very much overwhelmed with a lot of nursing care activities. I know they cannot handle some of those things but they have no choice but to do for the sake of their patients (NP 7).
For me, being a guardian here is emotionally draining because there is a lot that I need to deal with every day, I worry about my husband [the patient], the children at home, I also work, and the way we live here (PG 3).
The sudden assumption of the caring role disrupts the normal functioning of the entire family unit.
My daughters are taking turns to look after the grandchild because the nanny alone cannot be trusted with a little child. I asked my elder daughter to miss school the other day so that she makes sure that the grandchild is well taken care of at home. It is not easy for the children to be alone at home especially at night since I’m a single parent so I am not at peace most of the time because I don’t know if the children are safely back home[…] (PG 9).
Economic burden of the caring role
The caring role negatively affects the economic situation of PGs and their families by reducing their disposable household income, increasing the household expenditure while donating care to the hospital.
The caring role leads to a reduction in household income. PGs who were formally employed would lose their pay when they miss work, those on informal employment would not be able to earn any income if they do not work.
I earn a living by doing some piece work, so now that I am here with my brother, I am not earning any money to support my family (PG 2).
[…] My daughter had also taken some unpaid leave days from work, to help look after her brother because the way he is one person cannot manage to calm him down (PG 7).
Some PGs who are running their small businesses, either close up the business because there is no one they can trust to run the business or the business is run by someone who is not effective enough to generate the amount of income that is usually generated by the owner.
I have a small shop where I sell groceries back home but now I just closed it when coming here because I could not trust it with anyone. So it is very difficult to meet most of the needs when I am here (PG 6).
Families of PGs that lived within Lilongwe visited them at least twice a day. However, those that lived far were not able to visit frequently because it was expensive for them to meet the transport costs.
The cost of coming here three times every day is way too expensive for the family because we don’t plan for this kind of expense but we just have to do it (PG 8).
They do come but not as frequent because of transport problems. We come from far and my children come only when they have money. They are all not working (PG 2).
Apart from transport costs, PGs and their family spend their disposable income to provide the patient and the PG with food and other necessities while in hospital.
They bring us food from home but sometimes we buy it outside the hospital since the food they provide is only enough for the patient. Sometimes those who come to cheer us bring some food and we eat (PG 8).
PGs contribute to the workforce in the healthcare system without being compensated to fill in the gaps in care due to a shortage of staff.
[,]they {PGs} help us, they mostly help us with things that often nurses do not do, [,] We can’t manage to offer most of the care to the patients, individually so they help us to offer those aspects of care (NP 1).
Coping with the caring role
In this study, we found that the sudden acquisition of the caring role by PGs leads to disruption of their routine roles and responsibilities. PGs need to adapt to the burden that comes with the caring roles and responsibilities to offer meaningful care to their patients. The findings of this study revealed that peer and professional support facilitated PGs’ adaptation to the caring role.
Peer support
The findings show that PGs had a good relationship with each other. They helped each other physically, psychosocially, and spiritually; this enabled them to cope with the caring role. PGs shared food and other necessities while in hospital.
We share things like food, beddings and utensils like cups and plates. So some guardians are from far their relatives don’t bring them food every day so we usually share even other things like soap for washing and bathing (PG 9).
PGs looked after each other’s patients when one goes out.
Sometimes when you want to go out you ask the other guardian to look after your patient while you are away. So we find it easier to stay here because of other guardians (PG 9).
The PGs cheered one another up and kept each other company and encouraged one another spiritually by sharing the word of God.
It is good, so far, no problem, we spend a lot of time together and share what we are experiencing here. We cheer each other up and sometimes share the word of God (PG 8).
The PGs welcomed new PGs at the time of admission and gave them information regarding the ward routines. They also consulted each other when they were not sure of what to do to help their patients before they could seek help from the nurses. PGs taught each other how to perform certain activities and helped each other with patient care.
I ask the other guardians when I’m not sure of what to do, some are very good and they show you or they even help you how to do things, or where to get what you want. When we were just admitted, the guardian that was next to my husband’s bed told me all the things I needed to know in this ward (PG 2).
Professional support
Nurses assess whether PGs are coping with their newly acquired caring role or not and they intervene accordingly.
Of course, it happens here, seeing a very exhausted guardian but we counsel and give them information so that they can cope with the situation that they are facing, there isn’t much really that we do, we ask them to ask another relative to come and help them because the guardians sometimes hardly sleep depending on their patient’s condition (NP 3).
Nurses gave PGs some materials that they needed to manage their patients like gloves, cotton wool, and spirit.
Nurses also share with us some things to use such as gloves and when they are finished, they also tell us (PG 9).
Nurses gave information to PGs if they requested it.
But some understand and they will tell you what to do if you ask them (PG 12).
Nurses advised PGs to do some aspect of care to ensure continuity of care at home when the patient is discharged.
We{nurses} advise the guardians to do (the wound care) so that they can continue with the same care at home (NP 1).
DISCUSSION
The insider views of PGs and nurses were explored on the burden of the caring role on family members who are involved in caring for acutely ill adult inpatients at a tertiary hospital in Malawi and how they adapt to the burden of the caring role. An acute illness and emergency hospitalization of one member of the family and the sudden acquisition of the caring role by a PG is viewed as a focal stimulus that disrupts the normal functioning and routines (Clissett et al., 2013)for the rest of the family members. The findings of this study demonstrated that the caring role may lead to poor physical, the psychosocial and economic well-being of the PGs. Peer and professional support facilitate family members’ adaptation to their newly acquired caring role.
The Roy Adaptation Model (RAM) by Sr. Callista Roy (Parker and Smith, 2010)was used to support the discussion of findings of this study. The RAM applies to two concepts, systems, and adaptation (Sitzman and Eichelberger, 2011). Systems in this model have been defined as a group of related and connected units that form a unified whole. This may be an individual, family, group, community, or society (Sitzman and Eichelberger, 2011). The model has the following assumptions: the person is a bio-psychosocial being who is in constant interaction with a changing environment, to respond positively to environmental changes, a person must adapt in the following modes of adaptation: physiologic needs, self-concept, role function, and interdependence. Roy defines adaptation as effective coping mechanisms that promote integrity for a person or group of persons. The model has four major concepts: person, environment, health, and nursing (Roy, 2009; Sitzman and Eichelberger, 2011). All four concepts have been used in this study.
The study found that PGs are involved in offering diverse roles with little or no support from nurses to meet the needs of their patients. This corroborate with findings from Hoffman et al. (2012) and Alshahrani et al. (2018) who stated that the role of PGs in acute care hospital settings is ambiguous. Nurses leave basic and technical aspects of care for PGs due to increased workload. However, some of the roles that PGs willingly perform are physically and emotionally challenging because they lack knowledge and expertise on how to perform them. PGs experience physical symptoms due to environmental challenges in the setting where care is being rendered (Geere et al., 2013). The common physical complaints that participants reported in this study were generalised body pains (back and musculoskeletal pain) due to excessive handling of patients, lifting and turning of patients. Other symptoms reported in this study are tiredness and physical exhaustion due to inadequate rest. Similarly, Geere et al. (2013) reported moderate to severe musculoskeletal pain as one of the common symptoms that caregivers experience due to the lifting of patients. PGs’ lack of knowledge on how to promote their good health when performing certain activities contributed to the generalised body pain that they complained of. Nurses should educate PGs on various lifting techniques to enable PGs to preserve their good health. This would facilitate their adaptation to the caring role.
The hospital environment can be a technically bewildering experience for the PGs with the routines, roles, staff, equipment, and sounds. PGs also experienced a lack of or inadequate sleep due to noise from other patients and HCW at night, uncomfortable sleeping space because they slept on a cold and hard floor, or some sat on a bench throughout the night. Safety, ventilation, acoustic environment, interior layout, room type, furniture and its placement and ergonomics affect the health and well-being of humans in healthcare facilities (Salonen et al., 2013). The wards where PGs were involved in caring for surgical inpatients were usually congested because they were occupied by at least twice the number of people that were meant to use the facilities. Overcrowding can facilitate the spread of airborne diseases among patients and their PGs. The lack of resting facilities for family members is one of the challenges that lead to lack of or inadequate rest for PGs (Gondwe et al., 2011). Soderback and Christenssoon (2008) and Alkali et al. (2014) corroborate with our present findings. The poorly designed hospital infrastructure may increase the anxiety and stress of PGs during their period of hospitalization. Failure to adapt to the newly acquired caring role may lead to high levels of acute and chronic stress, anxiety and depression (Kynoch et al., 2016). Nurses should encourage PGs to have a break from the caring role by exchanging with other family members so that they could rest at home. A policy was recommended to redesign the hospital floor plan to meet the cultural requirements of involving PGs in caring for inpatient in Malawian hospitals to enable PGs to participate in offering care in a conducive environment.
PGs perceive that they are not cared for when they are involved in caring for inpatients and that their needs are not correctly assessed by nurses (Linnarsson et al., 2010). The extent to which PGs feel connected with others, redefine their personal use of time and feel comfortable with their new responsibilities indicates how they are adapting to the transition (Pereira and Botelho, 2011). PGs underwent psychosocial burden when involved in caring for acutely ill adult inpatients in surgical wards. They perceived the caring roles as “hard”, “emotionally draining” and “overwhelming” because they just must be there for their patients even though they are not prepared for such a role.
PGs produce a large amount of output inpatient care because they supplement care provision when nurses leave some aspects of care undone. However, there is no compensation for caring for family members. Admission of a family member in the hospital means added expenditure to the family (Lee et al., 2012; Siffleet et al., 2010). The findings of this study have shown that PGs lose income when they take up the caring role through loss of earnings and increased expenditure of the family’s disposable income. Hospital authorities should consider compensating PGs with necessities such as food to enable them to adapt to the caring role.
PGs adapted to the caring role through active interaction with other PGs and nurses. The socialization process enables adaptation to one’s culture. They offered each other physical, psychosocial, and spiritual support. Despite their diverse cultural orientation, the socialization process that occurred due to their deliberate and frequent interaction enabled them to share common goals and live harmoniously. The Roy Adaptation Model (RAM), assumes that the role of nurses in an acute care hospital setting is to enable successful adaptation of patients and their family members to the changing internal and external environment because the family members’ adaptation is interdependent on the interaction that they have with the nurses (Parker and Smith, 2010). Nurses were key to the adaptation of PGs to their newly acquired caring role. Although nurses had limited time to interact with PGs, they were able to assess PGs coping mechanisms and assisted them to adapt to the caring role. PGs who looked exhausted were advised to ask another family member to take over the caring role to enable the exhausted PG to rest. Nurses provided PGs with gloves, cotton wool and other sundries that they were required to use when caring for their patients. Although nurses focused most of their attention on patients, they managed to teach PGs how to perform certain roles to facilitate effective continuity of care after discharge. Nurses should create family care support groups for PGs to share information and offer psychological support to facilitate their adaptation to the caring role.
Further research is needed to evaluate measures that would facilitate the adaptation of PGs to the caring role in adult acute care hospitals.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Alkali IA, Ahmad MHH, Said I (2014). The Challenges of Nigerian hospital ward setting in providing for family participation. Applied Mechanics and Materials 584:142-151. |
|
|
Alshahrani S, Magarey J, Kitson A (2018). Relatives' involvement in the care of patients in acute medical wards in two different countries-An ethnographic study. Journal of Clinical Nursing 27(11-12):2333-2345. |
|
|
Brunner LS (2010). Brunner & Suddarth's textbook of medical-surgical nursing. Philadelphia: Lippincott Williams & Wilkins. |
|
|
Clissett P, Porock D, Harwood RH, Gladman JRF (2013). Experiences of family carers of older people with mental health problems in the acute general hospital: a qualitative study. Journal of Advanced Nursing 69(12):2707-2716. |
|
|
Coyne I (2013). Families and health-care professionals' perspectives and expectations of family-centred care: hidden expectations and unclear roles. Health Expectations 18(5):796-808. |
|
|
Coyne I, Murphy M, Costello T, O'Neill C, Donnellan C (2013). A survey of nurses' practices and perceptions of family-centred care in Ireland. Journal of Family Nursing 19(4):469-488. |
|
|
Cresswell lJW (2013). Qualitative inquiry and research design: choosing among five approaches. Thousand Oaks CA: Sage Publications. |
|
|
Elo S, Kääriäinen M, Kanste O, Pölkki T, Utriainen K, Kyngäs H (2014). Qualitative content analysis: a focus on trustworthiness. Sage Open 4, 2158244014522633. |
|
|
Ewart L, Moore J, Gibbs C, Crozier K (2014). Patient-and family-centred care on an acute adult cardiac ward. British Journal of Nursing 23(4):213-218. |
|
|
Festini F (2014). Family-centred care. Italian Journal of Paediatrics, 40(1):1-1. |
|
|
Geere JL, Gona J, Omondi FO, Kifalu MK, Newton CR, Hartley S (2013). Caring for children with physical disability in Kenya: potential links between caregiving and carers' physical health. Child Care Health Development 39(3):381-392. |
|
|
Gondwe WTM, Bultemeier K, Bhengu BR (2011). Challenges encountered by intensive care nurses in meeting patients' families' needs in Malawi. African Journal of Nursing and Midwifery 13(2):92-102. |
|
|
Goodson L, Vassar M (2011). An overview of ethnography in healthcare and medical education research. Journal of Educational Evaluation for Health Professionals 8(4). |
|
|
Hoffman M, Mofolo I, Salima C, Hoffman I, Zadrozny S, Martinson F, Horst CVD (2012). Utilization of family members to provide hospital care in Malawi: The role of hospital guardians. Malawi Medical Journal 24(4):74-78. |
|
|
Khosravan S, Mazlom B, Abdollahzade N, Jamali Z, Mansoorian MR (2014). Family participation in the nursing care of hospitalized patients. Iranian Red Crescent Medical Journal 16(1). |
|
|
Kuo DZ, Houtrow AJ, Arango P, Kuhlthau KA, Simmons JM, Neff JM (2012). Family-centred care: current applications and future directions in pediatric health care. Maternal and Child Health Journal 16(2):297-305. |
|
|
Kynoch K, Cabilan CJ, McArdle A (2016). Experiences and needs of families with a relative admitted to an adult intensive care unit: a qualitative systematic review protocol. JBI Evidence Synthesis, 14(11):83-90. |
|
|
Lee WS, Chai PF, Ismail Z (2012). Impact on parents during hospitalisation for acute diarrhoea in young children. Singapore Medical Journal, 53(11):755-759. |
|
|
Lincoln SY, Guba EG (1985). Naturalistic Inquiry. Thousand Oaks CA: Sage Publications. |
|
|
Linnarsson JR, Bubini J, Perseius KI (2010). A meta-synthesis of qualitative research into needs and experiences of significant others to critically ill or injured patients. Journal of Clinical Nursing 19(21?22):3102-3111. |
|
|
Mackie BR, Marshall A, Mitchell M (2018). Acute care nurses' views on family participation and collaboration in fundamental care. Journal of Clinical Nursing 27(11-12):2346-2359. |
|
|
Parker ME, Smith MC (2010). Nursing theories and nursing practice. 3rd ed. Philadelphia: FA Davis Co. |
|
|
Pereira HR, Botelho MAR (2011). Sudden informal caregivers: the lived experience of informal caregivers after an unexpected event. Journal of Clinical Nursing 20(17?18):2448-2457. |
|
|
Polit DF, Beck CT (2017). Generating and assessing evidence for nursing practice, 10th ed. Philadelphia: Lippincott Williams & Wilkins. |
|
|
Roy C (2009). The Roy adaptation model. 3rd ed. Upper Saddle River, NJ: Pearson Prentice Hall. |
|
|
Salonen H, Lahtinen M, Lappalainen S, Nevala N, Knibbs LD, Morawska L, Reijula K (2013). Physical characteristics of the indoor environment that affect health and wellbeing in healthcare facilities: a review. Intelligent Buildings International 5(1):3-25. |
|
|
Siffleet J, Munns A, Shields L. (2010). Costs of meals and parking for parents of hospitalised children in an Australian paediatric hospital. Neonatal, Paediatric and Child Health Nursing 13(3):7-11. |
|
|
Sitzman KL, Eichelberger LW (2011). Understanding the work of nurse theorists: a creative beginning. 2nd ed. Sudbury, Massachusetts: Bartlett Publishers. |
|
|
Soderback M, Christenssoon K (2008). Family involvement in the care of a hospitalised child: A questionnaire survey of Mozambican family caregivers. International Journal of Nursing Studies 45(12):1778-1788. |
|
|
Spradley JP (2016a). The ethnographic interview. Belmont, CA: Waveland Press. |
|
|
Spradley JP (2016b). Participant Observation. Belmont, CA: Waveland Press. |
|
|
Thomson D (2011). Ethnography: a suitable approach for providing an inside perspective on the everyday lives of health professionals. International Journal of Therapeutic Rehabilitation 18(1):10-17. |
|
|
Wall SS (2014). Focused ethnography: a methodological adaptation for social research in emerging contexts. Qualitative Social Research, 16(1). |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


