Full Length Research Paper

ABSTRACT
Triage tools have been shown to increase efficiency and accuracy of obstetric triage, but no published tools exist for low income settings. A novel guideline was developed and implemented in the tertiary maternity hospital of Sierra Leone. A triage system was implemented using a quality improvement approach. A novel triage guide, mentorship, improved patient flow and training were introduced. Prospective data was collected at three points over 5 months, capturing allocated triage category accuracy according to the system. The number of patients correctly triaged was 43.22% (n=51) before implementation, 81.82% (n=117) two weeks after training and 87.85% (n=159) two months after training. There was strong evidence (p=0.002) for the 44.63% (95% CI 34.50% - 54.89%) increase in correct triage. Implementation of an obstetric triage system increased the amount of correctly triaged patients. Further research to evaluate patient outcomes, wait times and robust validation of this triage tool is needed.
Key words: maternity, obstetric, emergency, triage, system, tool, guide, low income, low resource, developing country
INTRODUCTION
Emergency medicine triage guides have been shown to improve quality and efficiency of care in emergency departments, providing a standardised structure (Rosedale et al., 2011). Obstetric departments in high income settings have been slower to adopt a formal structure, despite this being identified as an area for improvement (Macones et al., 2016; Angelini and Howard, 2014). A large UK survey in 2015 suggested that 81% of hospitals do not have a formal obstetric triage system in place (Kenyon et al., 2017). Recently, some maternity units have been adopting a more formal approach, with good results (Kenyon et al., 2017; Ruhl et al., 2015; Quaille, 2018; Humphrey et al., 2017; Paisley et al., 2011; Smithson et al., 2013). The Obstetrical Triage Acuity Scale (OTAS) system in Canada is one of the first published and validated obstetric triage tools, with implementation leading to reduced use of resources and waiting times with an increase in staff satisfaction (Smithson et al., 2013).
There are no published and validated triage tools suitable for a low resource setting, despite quality of care on arrival in referral centres being documented as an area in need of improvement (Forshaw et al., 2016). In Ghana, a middle-income country, a team designed and implemented a triage system successfully and sustainably in a maternity referral centre (Floyd et al., 2018). Despite its success, the authors highlighted the impact of the limitations of resources and environment on the implementation of any triage system. This demonstrates both the potential use of a triage tool specific for a low-income setting, and the importance of ensuring that any system implemented is designed to be effective with the available resources. The drive to increase timely hospital referrals in low income settings is crucial; however this raises pressure on under resourced and over capacity facilities (Goodman et al., 2017). Therefore, improvement of patient flow and ensuring optimum use of resources is more vital than ever.
Context and objectives
There was no formal triage at Princess Christian Maternity Hospital (PCMH), Sierra Leone. Delay in care and lack of identification of emergency cases on arrival had been raised by staff as an issue during quality improvement discussion groups. The Outpatient Department (OPD) was seeing a mean of 1,163 patients a month; where patients are mainly presented collectively in the morning, with only one small private space to assess patients. As the only referral centre for the country, a streamlined triage is vital to ensure that critical cases are treated promptly.
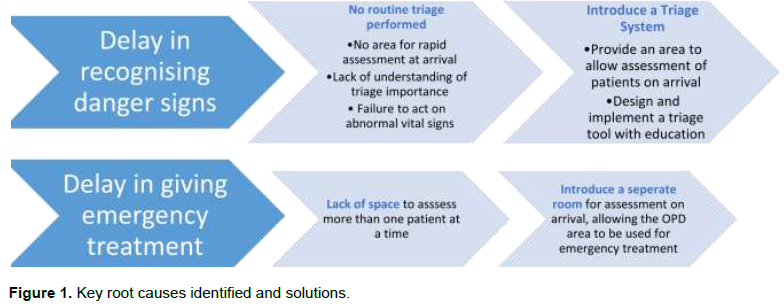
A root-cause analysis was performed using a fish bone diagram by hospital management and senior staff, facilitated by non-governmental organisation (NGO) Welbodi Partnership. It was found that several key issues could be resolved through development and implementation of a triage guide designed specifically to meet the skills and resources available to the department. For this to work, the patient flow would need to be adjusted to create an initial space to allow rapid assessment and allocation of a triage urgency for all incoming patients. Figure 1 summarises the key root causes identified, and the actions planned to address this. Two objectives were drawn from the root cause analysis: Provide an assessment area and design as well as implement a triage tool. The intention was that this would increase the recognition of danger signs and ensure immediate provision of emergency treatment.
METHODOLOGY
Planning
Two senior midwives were identified to lead this quality improvement project with prospective data collection. A midwife working for Welbodi Partnership supported them throughout the process. Using a quality improvement model, in December 2016 an aim statement was created (Healthcare Quality Improvement Project, 2015). It was decided that the primary outcome would be the correct triage of patients on arrival, reflecting whether the implementation of a triage tool was influencing clinical practice. Therefore, after the baseline data was collected, this aim statement was developed:
“To increase the correct triage of patients according to the PCMH obstetric triage tool in PCMH Outpatients’ Department from 43 to 80%, from December 2016 to April 2017”.
To achieve this, the PCMH triage tool was designed, to unify practice and allow for a good basis for training (Appendix 1). As there were no published maternity triage systems for a low-resource setting, a guide was developed in partnership with the hospital and external experts, using tools from high-income settings to inform its development (Smithson et al., 2013). The format was based on the South African Triage System (SATS) which is a successful system and well established used for adults and children in the tertiary adult facility in Sierra Leone, Connaught hospital (Rosedale et al., 2011). The tool would not be able to be verified before use, so great effort was made to get feedback from as many staff and experts as possible, pooling clinical judgements and available evidence.
Implementation
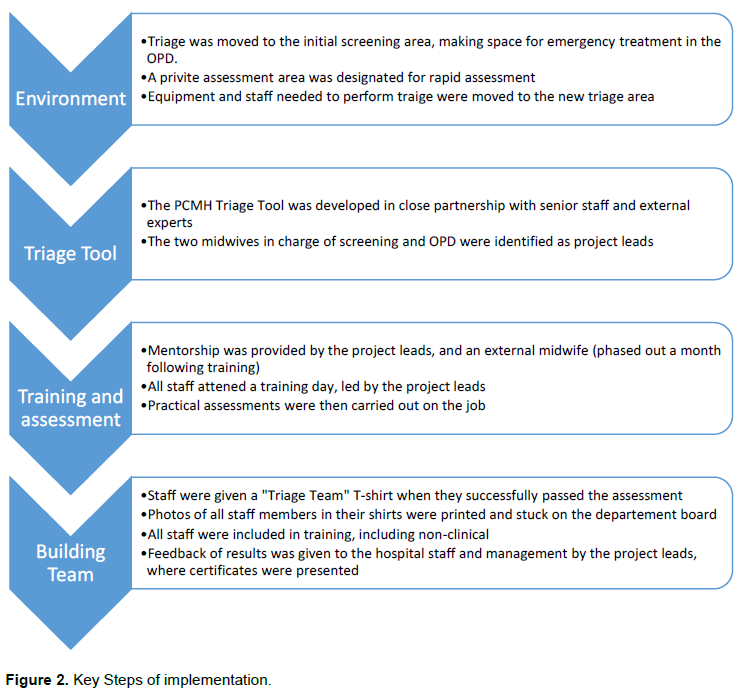
The triage tool was put into practice in December 2016, supported by clinical mentorship from the project leads and the Welbodi Partnership midwife. An initial assessment area where patients could be categorised was set up, before going to either wait or be treated, as shown in Figure 2. A private area to allow a better history and assessment to be undertaken was introduced. The nurse in the initial assessment area uses the triage tool to calculate the urgency. The patients’ card is then marked with the urgency and the corresponding marker colour, and shown to the OPD waiting area. The cards allow the order in which patients should see the doctor to be easily determined. During their wait time, further tests such as urinalysis can be performed and if the patient’s condition changes, reassessment would be carried out.
Initially this created disruption and frustration for the clinical staff, as triage, particularly nurse led, was a new concept for the hospital. Despite this, the feeling of the department quickly became more positive. Staff saw that implementation led to improved patient flow and a more efficient and less chaotic working environment.
Official training took place for all nurses, midwives and porters on OPD and screening, as well as key members of senior hospital staff, in February 2017. Thirty two staff were split into morning and afternoon session so as not to disrupt the clinical work. Staff that were unable to undergo training that day were trained individually later by a mentor. Following this, all staff were assessed triaging three consecutive patients using a standardised checklist. Staff were allowed three attempts to pass, and if they failed the third attempt, they would have to retake the training. The two porters discussed individual scenario-based conversations as they were not directly involved in assessing patients. They were included as they often meet patients first, so an understanding of the new system would aid the smooth running of the department.
60% of staff passed on their first attempt, 32% on the second and 8% on their third. At two weeks following training, 48% of staff had successfully passed, at three weeks 84% and at three months all staff had successfully passed. When staff passed, they were photographed receiving “Triage Team” T-Shirts, which were then printed and displayed on the team photo board and posted to the WhatsApp group. This received good feedback from staff and helped to build a sense of pride, motivation and improved morale. Clinical mentorship and logistical support from Welbodi Partnership was provided to the department throughout the design and implementation, and then gradually withdrawn from one month following training. As the two project leads were instrumental throughout the process, the complete handover to them was smooth. By March 2017 during the final data collection, the project was receiving no further support from Welbodi Partnership.
Data collection and analysis
Data collection was challenging, as before the intervention there was no documentation of triage, patients’ history or presenting condition. Maternal and neonatal mortality outcomes are available for the hospital; however, there were too many other influential factors, such as seasonal variation and other interventions, to accurately interpret this data. It proved impossible to initially collect accurate waiting times with the resources available, therefore only the accuracy of triage was initially collected. The correct and given triage urgency categories (according to the PCMH Triage Tool) given to patients was collected prospectively at three points over five months. These were one-week periods each with data collected on weekday mornings. This timing was chosen as the volume of patients is the highest at this point and includes routine as well as emergency referrals. No sample size calculation was performed, as this was a pragmatic audit, with the most data collection possible achieved with the available resources.
Baseline data was collected through observation of staff practice by the Welbodi Partnership midwife, in order to capture informal triage of patients. As no official triage was being used it was difficult to categorise the given urgency, however through watching staff perform initial assessments and then hearing how quickly staff wanted them to be seen, a categorisation was recorded according to the corresponding time in the PCMH Triage Tool. The time of arrival and time seen by a doctor were recorded alongside the given and actual triage category according to the triage tool, using the Welbodi Partnership midwife.
The patients who were not called on arrival by a nurse for anything other than registration and vitals (without acknowledging the results) were classed as not triaged. Through this method the data would then give a clearer picture of any improvements in assessments rather than just an improvement or initiation in documentation. Data was then collected twice more in the same way by the same midwife: at two weeks and two months after training. At two months after training, all external support had been withdrawn. Observation of practice was undertaken, recording the correct and actual triage urgency category allocated per person. Following training, the given urgency was recorded by the nurses, along with the condition and the findings of the patient, allowing the data to also be collected directly from the patient cards. This was used in conjunction with the observation used at the first data collection to validate the data and reduce bias.
Waiting times from triage is assessed or treated by a doctor, nurse or a midwife and were collected two months after implementation, as documentation and the patient flow improved. They were collected over a period of seven weekdays for all admitted patients, where two times and triage urgency were recorded in the notes. Whether or not the patient was seen by a doctor within the given urgency time was collected. For emergency cases, the time from triage to having care initiated by a healthcare practitioner was measured.
Statistical analysis of differences between percentages was performed using Stata (version 16.0). Ethics approval was not required as it was an audit of a standard hospital practices, reviewing a quality improvement project. All data was anonymised, and patients’ care was not compromised by the data collection.
RESULTS
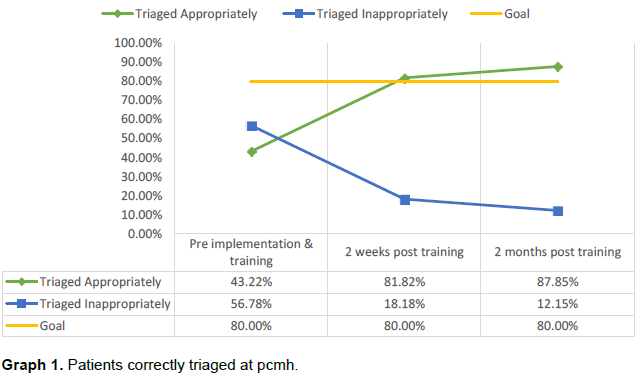
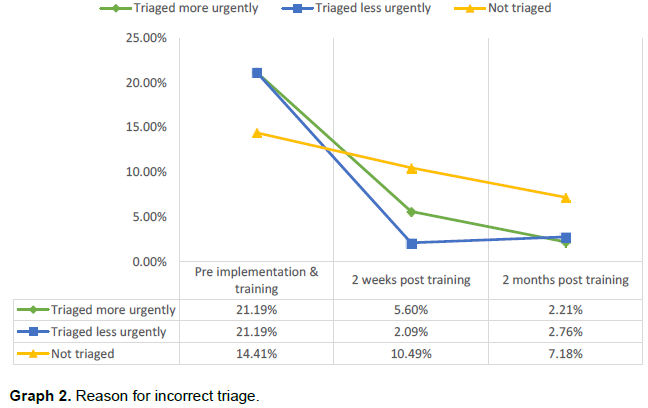
As presented in Graph 1, the number of patients correctly triaged increased from 43.22% (n=51) before implementation, to 81.82% (n=117) two weeks then 87.85% (n=159) two months after training. There is very strong evidence that this 44.63% (95% CI 34.50% - 54.89%) increase in correctly triaged patients was not due to chance (p=0.002). A total of 442 patients were audited, 10% before implementation (n=118), 14% two weeks after (n=143) and 13% two months after (n=181) of total cases admitted to OPD in the corresponding month. The number of patients incorrectly triaged reduced from 42.38% (n=50) to 4.97% (n=9). As displayed in Graph 2, of the 4.97% triaged incorrectly two months following implementation, 2.21% (n=4) were triaged more urgently and 2.76% (n=5) less urgently than the guideline. The number of patients not triaged at all reduced from 14.41% (n=17) to 7.18% (n=13).
100% of emergency cases received immediate care from a nurse. Two months following training, the mean waiting times to see a doctor was 60 min for very-urgent cases (6% within 10 min), 55 min for urgent cases (65% within 1 h) and 91 min for non-urgent cases (95% within 4 h). The total numbers audited were divided into 26 emergencies (6%), 62 very-urgent (15%), 81 urgent (19%) and 244 non-urgent (59%) cases.
DISCUSSION
This project demonstrates that in Sierra Leone an obstetric triage tool, alongside mentorship and improved patient flow, increased the number of correctly triaged maternity patients attending hospital. This was a successful quality improvement project, with the aim statement surpassed two weeks following training, in line with the only other triage system implementation published outside of a high-income setting (Kenyon et al., 2017).
Whether the tool places patients in the right time frame needs further work. Clinical outcomes would be useful to allow analysis around whether the use of the tool improves care. This would also allow adjustments to the criteria to be made as necessary and allow validation. A robust validation of the tool would be important in future use and to allow evaluation for use in other settings. Despite this, the number of incorrectly triaged patients was reduced consistently for all reasons, suggesting that the tool is reducing the number of patients triaged less urgently than they should be.
The tool appears to have the potential to be sustainable, with an increase in correctly triaged patients even after the withdrawal of Welbodi Partnership support. A strong ownership and sense of pride was fostered throughout the process through celebrating achievements, feedback of results and the leads of the areas heading the project. This contributed a great deal to the success of implementation. A follow up audit would be useful to assess how long lasting this change may be and documenting any development of the system.
The fact that the waiting time for very urgent cases is a mean of 60 min, compared to 55 min for urgent cases needs further work and investigation. The unit was extremely confined: 1 h was a relatively fast time to see a doctor with just one consultation room and potentially several serious cases. This highlights the multiple considerations needed to be made when implementing a project. It may be worth considering three categories with slightly different criteria, merging the urgent and very urgent categories. Overall, it is encouraging that emergency signs are attended to immediately; very urgent and urgent cases are seen by 60 min on average. The non-urgent cases are correctly waiting the longest at an average of 90 min, still well within the 240 min cut off.
There may have been measurement bias from the data collection midwife, who was also providing clinical mentorship. She may have more leniently coded the post training triaging due to an investment in the project. Validation was carried out with the notes at this point in an attempt to reduce this, and is unlikely that such a large increase is entirely due to this. She had been working in the area for several months previously, which may have reduced the impact of her presence during collection. However, the staff knew they were being audited and this may have led to observer bias. It is possible that the true number of patients being triaged correctly at the start of the project was lower than the baseline data suggests, as staff may have been more likely to triage whilst being watched. This was also the case at the subsequent collections; therefore each measurement would have been affected in the same way.
CONCLUSION
An obstetric triage tool, alongside clinical mentorship, increased the amount of maternity patients correctly triaged according to the guidelines. This was maintained after external support had been withdrawn for one month, indicating the use of the tool could be sustainable. Waiting times reflected the given urgency time frame, except for very-urgent cases which the staff reported was due to limited space. Further research looking at patient outcomes, as well as adaptation and validation of the tool, would suggest whether implementation in other comparable settings would be beneficial. There is the potential for a structured triage system to help low income referral hospitals manage their challenging workload with limited resources. A re-audit after a longer period of time would help to better gauge sustainability.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors appreciate Sister Fatmata J. Momodu, who was instrumental in this project and hugely respected throughout the hospital. She sadly died before the submission of this paper; otherwise she would have been an author. Thank you to all the hard working staff at Princess Christian Maternity Hospital.
REFERENCES
|
Angelini D, Howard E (2014). Obstetric triage: A systematic review of the past fifteen years: 1998-2013. The American Journal of Maternal and Child Health Nursing 39(5):284-297. |
|
|
Floyd L, Bryce F, Ramaswamy R, Olufolabi A, Srofenyoh E, Goodman D, Owen M (2018). The introduction of a midwife-led obstetric triage system into a regional referral hospital in Ghana. Midwifery 61:45-52. |
|
|
Forshaw J, Raybould S, Lewis E, Muyingo M, Weeks A, Reed K, Byamugisha J (2016). Exploring the third delay: An audit evaluating obstetric triage at Mulago National Referral Hospital. BMC Pregnancy and Childbirth 16(1):300. |
|
|
Macones G, Pattker, Cm Mascola M, Heine, P (2016). Committee Opinion Number 667: Hospital-Based Triage of Obstetric Patients. The American College of Obstetricians and Gynaecologists, 128(1):537-540. |
|
|
Goodman D, Srofenyoh E, Olufolabu A, Kim S, Owen M (2017). The third delay: Understanding waiting time for obstetric referrals at a large regional hospital in Ghanal. BMC Pregnancy and Childbirth 17(216). |
|
|
Healthcare Quality Improvement Partnership (2015). A Guide to Quality Improvement Methods. |
|
|
Humphrey MD, Foxcroft KF, Callaway LK (2017). Obstetric risk score - revalidated for triaging high-risk pregnancies in rural areas. The Australian and New Zealand Journal of Obstetrics and Gynaecology 57(1):63-67. |
|
|
Kenyon S, Hewison, A, Dann S, Easterbrook J, Hamilton-Giachrtsis C, Beckmann A, Johns N (2017). The design and implementation of an obstetric triage system for unscheduled pregnancy related attendances: A mixed methods evaluation. BMC Pregnancy and Childbirth 17(309):503-505. |
|
|
Paisley K, Wallace R, Durant P (2011). The Development of an Obstetric Triage Acuity Tool. The American Journal of Maternal Child Nursing 36(5):290-296. |
|
|
Quaille H (2018). Implementing an Obstetrics-Specific Triage Acuity Tool to Increase Nurses' Knowledge and Improve Timeliness of Care. Nursing Women's Health 22(4):293-301. |
|
|
Rosedale K, Smith ZA, Davies H, Wood D (2011). The effectiveness of the South African Triage Score (SATS) in a rural emergency department. South African Medical Journal 101(8):537-40. |
|
|
Ruhl C, Scheich B, Onokpise B, Bingham D (2015). Interrater Reliability Testing of the Maternal Fetal Triage Index. Journal of Obstetric, Gynaecologic and Neonatal Nursing 44(6):710-716. |
|
|
Smithson D, Twohey R, Rice T, Watts N (2013). Implementing an Obstetrical Triage Acuity Scale: Inter-Rater Reliability and Patient Flow Analysis. American Journal of Obstetrics and Gynaecology 209(4):287-293. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


