Full Length Research Paper

ABSTRACT
This study investigated the level of knowledge and attitude of married male workers about vasectomy and also the factors influencing the attitude of married men working in Babcock University towards vasectomy. Stratified random sampling technique was used to select 200 participants from the academic and administrative work divisions of the University and a self-constructed questionnaire was administered and 150 were retrieved and analysed using both descriptive and inferential statistics. Findings revealed that majority (42.7%) of the participants were between the ages of 31 to 40 years, Christians (97.3%), of the Yoruba tribe (55.3%), had a bachelor’s degree (46%) and were non-academic staff (53.3%). Majority (38%) of participants had adequate knowledge and 62.7% had positive attitude towards vasectomy. There was no association between participants’ level of education and their level of knowledge of vasectomy, however, a significant association was observed between participants’ level of knowledge and their attitude towards vasectomy (χ2cal= 53.89, P≤0.05). The risk of spouse’s health (54%) was the major factor influencing positive attitude and the need of more children (41.3%) was the main factor influencing negative attitude towards vasectomy. There is therefore need to develop awareness programs in order to equip the population with valid information and thus increasing their knowledge about vasectomy. Specific strategies should be developed in order to tackle the identified barriers hindering the acceptance of vasectomy among married men.
Key words: Knowledge, attitude, vasectomy, family planning, married men.
INTRODUCTION
Family planning has beneficial effects in terms of sustainable socio-economic development and protection of the environment (Alemayehu, 2012). Unfortunately, most family planning programs in Nigeria have primarily targeted women (Onasoga et al., 2013) and men often do not participate in reproductive health matters. According to Odu et al. (2006), Nigerian men still have poor knowledge and attitude towards family planning despite global move to increase the involvement of men in reproductive health matters. A concerted effort is there-fore needed to enhance men’s knowledge and increase their involvement in reproductive health (Ezegwui and Enwereji, 2009).
Sterilization, which includes vasectomy, is one of the important options available to married men who have decided to end childbearing, however, a number of identified factors affect the acceptance of vasectomy among men. In a qualitative study conducted by Bunce et al. (2007) using a focus group discussion and in-depth interviews to assess factors affecting vasectomy acceptability in Tanzania. Their findings showed that economical factors, spousal influence, religion, provider reputation and avai-lability, uncertainty about the future and poor vasectomy knowledge were major factors that influenced vasectomy decision making among men.
Knowledge and attitude towards vasectomy have been reported to have significant influence on its uptake among men. For example, a study conducted by Ezegwui and Enwereji (2009) reported that only 6.8% of men may accept vasectomy with the knowledge they currently have while 89% will not. This finding was also linked to the fact that majority of the men believed that sterilization should be left for women only. In the same vein, a study con-ducted in Pakistan reported that men felt that vasectomy could cause impotence and is exclusively meant for prisoners (Nishtar et al., 2012). These are examples of myths held by men which have affected their attitude and acceptance of Vasectomy. Worldwide, only about 3 to 6% of couples are using vasectomy as a method of contraception (Pile and Barone, 2009).
The low acceptance of vasectomy has also been reported in the developed countries. The result of a National survey in the United States of America showed that only 13.3% of married men reported having had a vasectomy done (Anderson et al., 2010). Also, another American survey reported that only 6% of married men have undergone vasectomy (Eisenberg and Lipshultz, 2010). This corroborates the opinion of Shih et al. (2014) that despite the lower risk, high cost-efficiency, and high efficacy of vasectomy compared with female sterilization, more couples from the United States of America rely on female sterilization than vasectomy. Reasons for low use of vasectomy included lack of knowledge and mis-conceptions about the procedure, lack of access, provider bias and patents preferences.
Healthcare professionals and public health educators have important roles to play in order to convey correct information about vasectomy to the population thereby increasing its acceptability. Unfortunately, Okunola et al. (2009) reported that majority of health care workers were unwilling to accept vasectomy and none of them had ever had vasectomy done. Similarly, Ebeigbe et al. (2011) reported that despite good knowledge about vasectomy among Nigerian resident doctors, only 41.3% would opt for it while 89.4% of doctors counselled often for bilateral tubal ligation, only 5.8% did vasectomy.
In order to increase the acceptance of vasectomy among men, awareness programmes need to be developed and conducted to enhance men’s knowledge and promote positive attitude towards vasectomy. It is in light of this that the researchers sought to assess the knowledge and attitude of married men about vasectomy as a method of family planning.
METHODOLOGY
The study adopted descriptive survey research design in generating priority data in measuring and analysing the variables under consideration. The study area was Babcock University, Ilishan-Remo, Ogun state. Stratified random sampling technique was used to select 150 participants from the academic and administrative work divisions of the University. A self-administered 37-item close-ended questionnaire designed based on the study objectives, was administered. The questionnaire included four sections: socio-demographic data, knowledge of vasectomy, attitude towards vasectomy and factors influencing attitude towards the choice of vasectomy. Ethical clearance was obtained from the Babcock University Health Research Ethics Committee. Participants were fully informed about the nature of the study and that their participation was voluntary. Furthermore, the information provided by the participants was treated with confidentiality. The questionnaires were directly administered personally and through three trained research assistants to the respondents at their various offices and collected immediately or later as time permitted. Instructions to guide the participants in filling the questionnaire were included. 200 questionnaires were distributed, 180 were retrieved and 150 were considered appropriate for analysis which involved both descriptive as well as inferential statistics of Chi-square at 5% level of significance. Participants’ knowledge level was graded using the arbitrary scoring system and the respondents’ attitude were scored using the Likert scale.
RESULTS
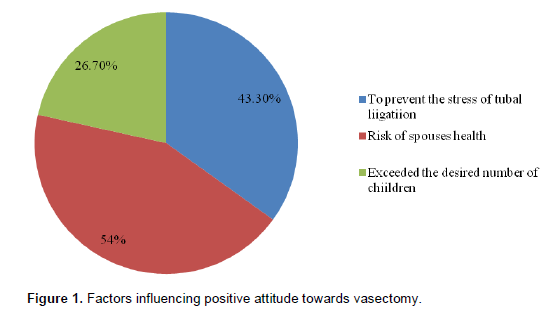
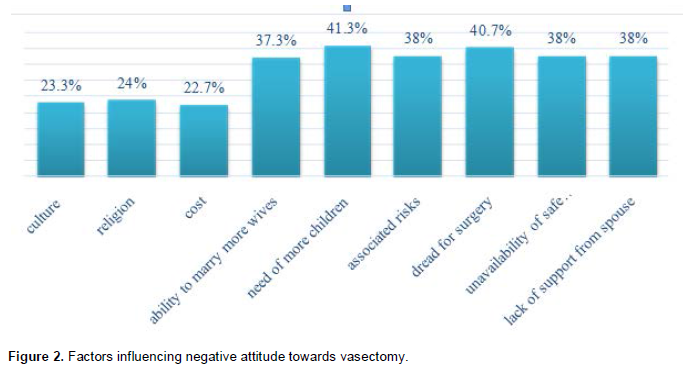
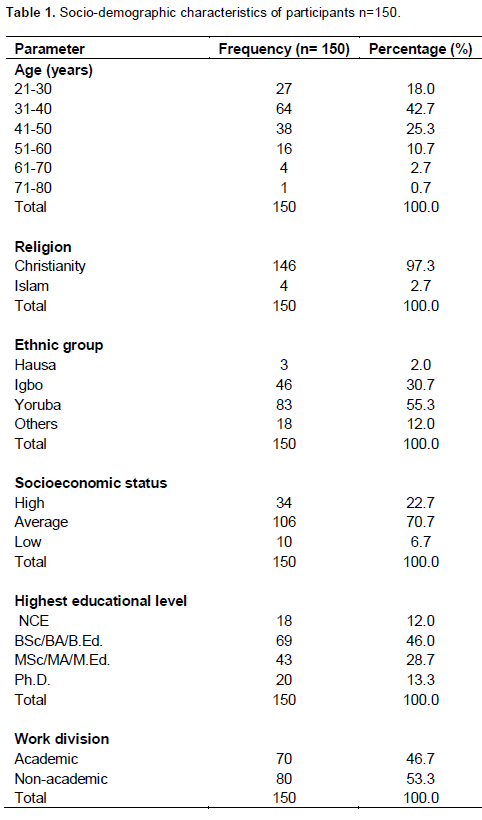
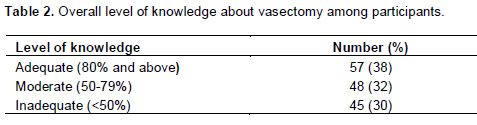
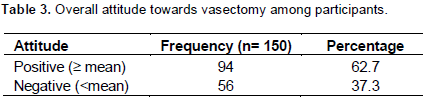
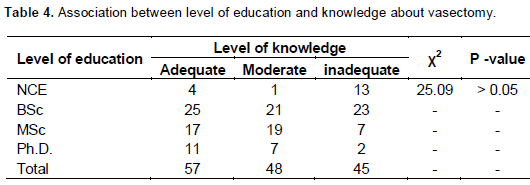
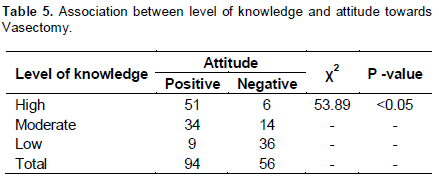
Figure 1 shows that the risk of spouses’ health (54%) was the major factor that influenced positive attitude towards vasectomy among participants. Figure 2 shows the need for more children (41.2%), dread or surgery (40.7%), fear of risk factors (38%), unavailability of safe practices (38%) and lack of support from spouse (38%) and ability to marry more wives (37.3%) were the major factors that influenced negative attitude towards vasectomy among participants. Table 1 shows that majority of the participants were between the ages of 31 to 40 years (42.7%), Christians (97.3%), Yorubas (55.3%), of average socio-economic status (70.7%), had a bachelors degree (46%) and were non-academic staff (53.3%). Table 2 shows that majority of participants (38%) had adequate knowledge while 30% had inadequate knowledge about vasectomy. Table 3 shows that majority (62.7%) of participants had positive attitude while 37.3% had negative attitude towards vasectomy. Table 4 indicates that there was no statistically significant association between participants’ educational level and their level of knowledge about vasectomy (χ2cal = 25.09, P>0.05). Table 5 shows that there was a statistically sig-nificant association between participants’ knowledge level and attitude towards vasectomy (χ2cal = 53.89, P <0.05).
DISCUSSION
Findings of this study have shown that majority of participants were between the ages of 31 to 40 years and had at least a bachelors degree which is not synonymous with the characteristics of participants in a previous study conducted in Nigeria by Onasoga et al. (2013). The difference in educational levels could be due to the fact that the current study was conducted in an educational institution where most people are expected to be educated. However, the age group in this present study is similar to the age group in another study conducted in Ibadan-Nigeria (Okunola et al., 2009).
The result of this study reveals that majority of parti-cipants had adequate knowledge about vasectomy. This finding contradicts the findings of Akpamu et al. (2013) who reported that majority of literate men in Epoma-Nigeria had inadequate knowledge about vasectomy as a method of contraception. Although, the studies were conducted among educated men, the difference in knowledge level could be due to methodological differen-ces and also due to the fact that the present study was an institutional study. To further describe participants’ knowledge about vasectomy, majority (60.7%) knew that a man cannot bear children once he has had a vasec-tomy done. This implies that majority of the participants knew that vasectomy is a permanent method of family planning. This corroborates the report of World health organization (1994) that there is a very small chance that a man’s partner will become pregnant after he has had a vasectomy. In addition, findings from this study revealed that only 10.7% of participants felt that vasectomy requires long period of hospitalization after it is done. Parallel to this, Bounce et al. (2007) opined that vasectomy is a safe, simple and effective but underused method of contraception. Although the safety of vasectomy has been emphasized, interestingly however, majority of the participants in this study knew that vasectomy does not protect against sexually transmitted infections and does not interfere with men’s sexual functions. This is contrary to the report of Bounce et al (2007) who stated that Tanzanian men and women believed that vasectomy would result in decreased sexual performance also in the report of Nishtar et al. (2012) reported that participants believed vasectomy could cause impotence.
A positive attitude is required in decision making about vasectomy uptake. Findings from this study have shown that positive attitude towards vasectomy was observed among majority of participants. Specifically, only very few of the participants (8.7%) believed that family should be left for women alone and only 15.3% believed that vasectomy was a form of castration. This implies that negative attitude towards vasectomy could be linked to myths and misconceptions regarding the procedure. Contrary to the attitude observed among the participants in the present study, the findings of Ezegwui and Enwereji (2009) and Onasoga et al. (2013) showed that 40.7 and 48.5% respectively viewed vasectomy as castration. As component of parti cipants’ attitudinal disposition towards vasectomy, majority disagreed that vasectomy would affect men’s dignity thus opposing the opinions of participants in Nishtar et al. (2012) where vasectomy was viewed to be meant exclusively for prisoners. While assessing further on the reasons for approval and disapproval off vasectomy as a method of family planning, result of this study showed that positive attitude towards vasectomy was majorly influenced by risk of spouses’ health (54%) and stress of tubal ligation (43.3%) while negative attitude towards vasectomy was influenced by need for more children and dread for surgery. This implies that the married men in Babcock University will most likely not consider vasectomy because they are in need of more children. Similar fin-dings were reported in other studies as major factors that influenced men’s decision regarding vasectomy (Dutta et al., 2004; Murthy and Rao, 2003). However, this result is in contrast with a similar study conducted by Onasoga et al. (2013) in which cultural acceptance 82.4% (112), religious acceptance 72.1% (98), ignorance 70.6% (96) and accessibility of family planning clinic 66.2% (90) were the major factors negatively influencing attitude of men towards acceptance of vasectomy.
Another important finding of this study was that participants’ educational qualification did not have a significant association with their level of knowledge about vasectomy. This implies that knowledge of vasectomy may not necessarily be more among the highly educated. A contrary finding was reported by Soaji et al. (2013) who found that level of knowledge about vasectomy was more among people with higher education and also Keramat et al. (2011) reported positive associations between educational levels and choosing to have a vasectomy. With regards to the relationship between knowledge and attitude towards vasectomy, findings showed a statistically significant association between participants’ knowledge level and their attitude towards vasectomy. Positive attitude was observed more among participants with adequate knowledge about vasectomy which opposes the result of Onasoga et al. (2013). Also contrary to this result, a previous study among Nigerian resident gynaecologists reported that despite good know-ledge about vasectomy among doctors, majority were poorly disposed towards use of vasectomy (Ebeigbe et al., 2011). This indicates a need for effective national training programmes targeted at health workers to enhance their knowledge of vasectomy as well as break barriers to personal use of and counselling for vasectomy.
Associated risks, unavailability of safe expertise, lack of support from spouse and ability to marry more wives were additional factors that had negative influence on participant’s attitude towards vasectomy. There is therefore need to develop awareness programs in order to equip the population with valid information and thus increasing their knowledge. This will invariably help individuals to overcome certain barriers. This study identified that spousal support and influence have effect on the acceptability of vasectomy, which is synonymous with the findings of Bounce et al. (2007). Therefore, the women group should be targeted in order to change their attitude toward vasectomy and thus give their support.
CONCLUSION
Contrary to previous studies which reported inadequate knowledge about vasectomy among men in Nigeria, this study has found that men in the study population had relatively adequate knowledge and positive attitude towards vasectomy. Since knowledge level was observed to be significantly associated with individual’s attitude towards vasectomy, it is however, imperative that further education and counselling be provided to improve men’s knowledge thereby promoting positive attitude towards vasectomy as a method of family planning. Specific strategies should be developed in order to tackle the identified barriers hindering the acceptance of vasectomy among married men.
ACKNOWLEDGEMENT
The authors give thanks to God Almighty for giving them strength and wisdom throughout the course of this study. They also acknowledge the efforts of the participants who gave their time to be included in this study. We will not fail to appreciate Professor E.O Ajao for his encouragement and support.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
| Akpamu U, Nwoke EO, Osifo U C, Igbinovia ENS, Adisa A W (2010). Knowledge and acceptance of vasectomy as a method of contraception amongst literate married men in Ekpoma, Nigeria. Afr. J. Biomed. Res. 13:153–156. | ||||
| Alemayehu B (2012). Assessment of male involvement in family planning use among men in South Eastern Zone of Tigray, Ethopia. Sch. J. Med. 2(2): 1-10. | ||||
|
Anderson JE, Warner L, Jamieson D J (2010). Contraceptive sterilization use among married men in the United States: Results from the Male Sample of the National Survey of Family Growth. Contraception 82(3):230-235. Crossref |
||||
|
Bunce BA, Greg G, Hannah S, Veronica F, Peter R, Joseph K, Isaac A (2007). Factors affecting vasectomy acceptability in Tanzania. Int. Fam. Plan. Perspect. 33(1):13-21. Crossref |
||||
| Dutta M, Kapilashrami MC, Tiwari VK (2004). Knowledge, awareness and extent of male participation in key areas in reproductive and child health in an urban slum of Delhi. Health Popul. Perspect. Issues. 27:49-66. | ||||
|
Ebeigbe P N, Igberase GO, Eigbefoh J (2011).Vasectomy: A Survey of Attitudes, Counseling Patterns and Acceptance among Nigerian Resident Gynaecologists. Ghana Med. J. 45(3):101–104. Pubmed |
||||
|
Eisenberg ML, Lipshultz LI (2010). Estimating the number of vasectomies performed annually in the United States: Data from the National Survey of Family Growth. J. Urol. 184(5):2068-2072. Crossref |
||||
|
Ezegwui HU, Enwereji JO (2009). Attitude of men in Nigeria to vasectomy. Int. Health 1(2):169-72. Crossref |
||||
|
Keramat A, Zarei A, Arabi M (2011). Barriers and facilitators affecting vasectomy acceptability (a multi-stage study in a sample from North-eastern Iran), 2005-2007. Asia Pac. Fam. Med. 10(1):5. Crossref |
||||
| Murthy SR, Rao MD (2003). An Analysis of factors influencing the acceptability of vasectomy in Andhra Pradesh. Health Popul. Perspect. Iss. 26:162-182. | ||||
|
Nishtar NA, Sami N, Faruqi A, Khowaja S, Ul-Hasnain F (2012). Myths and fallacies about male contraceptive methods: a qualitative study amongst married youth in slums of Karachi, Pakistan. Glob. J. Health Sci. 5(2):84-93. Pubmed |
||||
|
Odu OO, Ijadunola KT, Komolafe JO, Adebimpe WT (2006). Men's knowledge of and attitude with respect to family planning in a suburban Nigerian community. Niger. J. Med. 15(3):260-5. Pubmed |
||||
|
Okunlola MA, Awoyinka SB, Owonikoko KM (2009). Awareness and practice of vasectomy among married male health workers at the University College Hospital, Ibadan, Nigeria. Niger. Postgrad. Med. J. 16(3):203-6. Pubmed |
||||
| Onasoga OA, Edoni EER, Ekanem J (2013). Knowledge and attitude of men towards vasectomy as a family planning method in Edo State, Nigeria. J. Res. Nurs. Midwifery 2(1):13–21. | ||||
|
Pile JM, Barone MA (2009). Demographics of vasectomy--USA and international. Urol. Clin. North Am. 36(3):295–305. Crossref |
||||
| Saoji A, Gumashta R, Hajare S, Nayse J (2013). Denial Mode for Vasectomy among married men in central India: Causes and suggested strategies. J. Psychol. Psychother. 3:4-7 | ||||
|
Shih G, Zhang Y, Bukowski K, Chen A (2014). Bringing men to the table: sterilization can be for him or for her. Clin. Obstet. Gynecol. 57(4):731-40. Crossref |
||||
| World Health Organization (1994).Vasectomy: What health workers need to know. Retrieved on 23rd March, 2013 from: http://apps.who.int/iris/bitstream/10665/58239/1/WHO_FHE_FPP_94.3_Rev1.pdf?ua=1 | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


