Full Length Research Paper
ABSTRACT
Nurses comprise the largest group of the health care workforce and play a central role in patient care activities. This study explored nurses’ perspectives about context specific job factors and coping strategies for back pain experiences among nurses in Lusaka, Zambia. An interpretive paradigm qualitative research design was used. Participants were selected using maximum variation including enrolled and registered nurses and nursing administrators. Data was collected using focus group discussions, transcribed verbatim and analyzed using content analysis. All thirty-two participants expressed experiencing back pain, correlated with job related factors. Context related job factors for back-pain experiences comprised workload and work environment factors. Inadequate staffing, high patient load, long work hours, mode of performing tasks, inappropriate equipment and work settings were cited as contributing factors. Pain relief medication, exercises, physiotherapy, dietary supplements and rest were coping strategies used. The study concluded that perspectives about context specific job-related factors for back-pain experiences nurses identified were job-related factors like inadequate human resource, high patient load, long work hours and mode of performing tasks. Raising self-awareness, physical activity, adequate infrastructure, manual handling training in clinical contexts and making changes in workflow are approaches that could minimise the effects of back pain experiences among nurses.
Key words: Back pain, nurses, context factors, strategies, qualitative study.
INTRODUCTION
Back pain commonly limits professional activities in the nursing profession (Richardson et al., 2019). Back pain refers to pain from the upper back to the interior gluteal folds, with or without leg pain (Chan, 2017). The prevalence of back pain among nurse’s ranges between 33 and 84% (Alnaami et al., 2019; Richardson et al., 2019; Johnson and Emmanuel, 2016; Nkhata et al., 2015).
This high occurrence of back pain in nurses is of major concern because it is a key cause for absence at work concern because it is a key cause for absence at work and a decrease in working efficiency that exerts economic costs and strain on the health system (Alnaami et al., 2019; Richardson et al., 2019). Direct and indirect costs of back pain in terms of quality of life for nurses are enormous (Johnson and Emmanuel, 2016). This is because back pain is associated with an incremental risk of chronic disease that can lead to a loss of functional health status and a loss in workforce expertise (Alnaami et al., 2019; Abedini et al., 2014). The compounded effect of nurses with back pain on the health system and patient outcomes of low resource countries is of great concern; considering that, some patients are highly dependent and may require constant attention from nurses, who because of experiencing back pain, may not be able to adequately perform the healthcare activities needed (Chan, 2017).
In most low resource settings, poor ergonomics and the lack of equipment to perform nursing tasks may be associated with back pain (Dlungwane et al., 2018; Johnson and Emmanuel, 2016). Consequently, nurses with back pain have impaired physical, social, and mental well-being (Abou El-Soud et al., 2014). Sadly, the burden of back pain in developing countries is exacerbated by low levels of education about back care, low social support, staff shortages, poor working conditions and poor job satisfaction (Dlungwane et al., 2018). In addition, social, cultural and economic contextual factors may negatively impact the experience of back pain among nurses. The compounded effect of these factors has an ill effect on the health system, nurses and patient outcomes.
Nurses form the largest group within a country’s healthcare workforce and central to patient care. Understanding the perceptions of nurses’ back pain is important in identifying intervention strategies that may decrease the scale of the problem. Most published reports in low income countries are focussed on the prevalence of back pain among nurses (Semachew et al., 2018). However, work-related low back pain among clinical nurses was reported in Tanzania (Mwilila and Frantz, 2008). Nonetheless, there are inadequate qualitative studies that have explored the lived experiences on context factors for back pain in the work settings among nurses. The perspectives on preventing musculoskeletal disorders in nurses (Richardson et al., 2019) and the nurses experiences of manual handling in health care (Kay et al., 2015) were reported in Australia. Qualitative methods are useful to study the experiences of nurses within the context of their work settings because informants can provide useful information that can enable one to understand their experiences and generate new information that is important in making decisions. Further, there are inadequate qualitative studies that have been done on context specific factors for back pain experiences among nurses especially in low-income settings (Richardson et al., 2019; Kay et al., 2015; Mwilila and Frantz, 2008). Context specific factors are
environmental influences such as experiences that have an impact on the phenomenon under observation (Woolf and Aron, 2013). The aim of this study was to explore the perspectives of nurses about their experience of back pain and context specific job factors and coping strategies. It was believed that understanding the nurses’ perspectives on context specific job factors would develop an evidence base from lived experiences of nurses that will be useful in developing practical and effective back pain intervention approaches to promote health and productivity in the work settings.
MATERIALS AND METHODS
Study design
This was a qualitative research design, which used an interpretive paradigm and a phenomenological research approach. An interpretive paradigm is concerned with the understanding of the phenomenon from individual subjective experiences including participant observations during the interviews (Thomas, 2010). While the phenomenological approach in qualitative research focuses on the commonality of a lived experience within a group with the goal of arriving at a description of the nature of a phenomenon (Cresswell, 2013). This approach was useful in this study because it gives voice to participants using decision making techniques (Varga-Atikins et al., 2011). Furthermore, the approach was useful in gaining insight, understanding of stakeholder perspectives and their opinions of back pain experiences for nurses in Zambia.
Participants and sampling strategies
To gain greater insight in the matter under study, participants were selected using a maximum variation sampling approach. Inclusion criteria comprised enrolled and registered nurses including nurse practitioners, nursing managers and administrators from a public facility in the peri-urban area of Lusaka. The facility provides various health services to both in and out patients including public health programmes at community level such as, interventions for common conditions including maternal and child health, HIV and AIDS, tuberculosis, water sanitation and malaria (LDHO, 2017). There are approximately seventy-five nurses working at this facility. To allow identification of common themes amongst a diverse sample the researchers, with the help of the principal nursing officer, identified and recruited registered nurses, enrolled nurses, midwives, public health nurses, nurse managers and administrators who were available at the time of data collection and serving in different departments.
Data collection
A total of three focus group discussions (FGDs) with the aid of a discussion guide, that had semi-structured questions, were used for data collection. The principal investigator (PI) conducted the interviews and an open communication approach was used to ensure that participants communicated their back-pain experiences with ease. The interviews were recorded using an electronic audio recorder and transcribed verbatim by professional transcribers. During the interviews, notes were taken on dynamic emotional aspects such as, reluctance and strong feelings attached to certain opinions or vocabulary used during the FGD. Socio demographic and work data were also obtained using a self-administered questionnaire before each FGD. Data verification was done during the FGD by asking participants to further elaborate on information and having participants respond to the summary of their responses.
Data analysis
Data analysis was done using Atlas.ti 8 for windows. Each transcript was analysed line by line to facilitate the capture of emergent themes during data collection. The PI checked the accuracy of the transcriptions by comparing the audio recordings with transcripts. The PI and DE independently analysed the transcript from FGD 1, compared codes and created a preliminary code book. Further, analysis involved a process of familiarizing with the data; highlighting significant quotes; expanding the codebook; coding the rest of the data; developing clusters of meaning and sorting categories and linkages to establish themes and sub-themes. This process allowed active engagement with the data and dependability and knowledge was generated using the participant’s perspectives that were grounded in the actual data. Conformability was enhanced when the same themes emerged from the data of subsequent focus group discussion transcripts. Quotations of text were extracted into separate documents under thematic headings and checked for consistency with the narrative contents which ensured robust representation of the audio and transcript data. Verification of themes and categories was done by the authors after studying and discussing the transcripts. Data saturation was considered when there were no more new emerging ideas or themes from the data.
Ethics
Ethical approval for this study was obtained as part of a bigger project entitled: the effectiveness of a contextualized back pain campaign for nurses in Lusaka, Zambia from the Stellenbosch University Health Research Ethics Committee (Reference #: S18/06/125s; Project ID:7431); the University of Zambia Health Sciences Research Ethics Committee, the National Health Research Authority, the Lusaka District Health Office and the participating Health Centre. Written informed consent and permission to record the interviews were also obtained from the participants beforehand.
RESULTS
Participants’ demographic descriptions
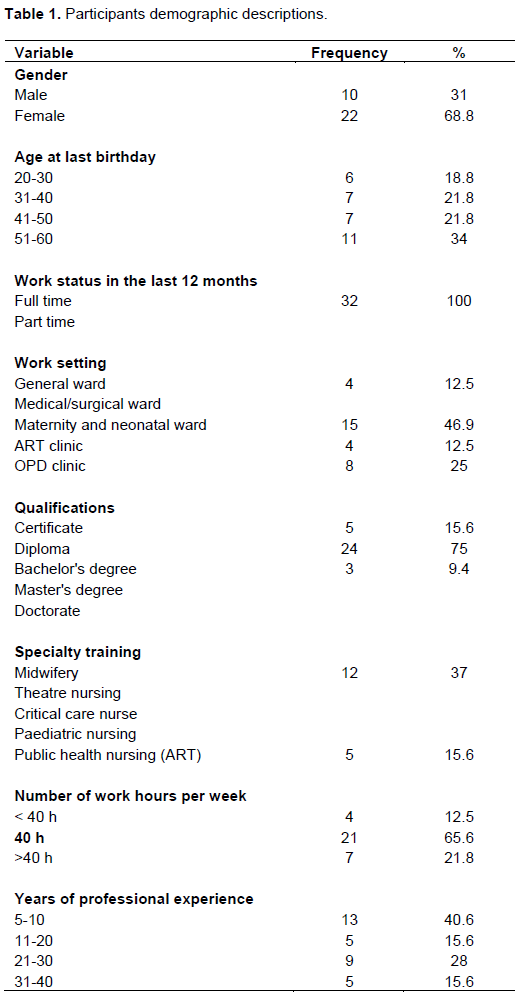
Thirty-two (32) out of forty (40) invited participants took part in the FGDs, 68.8% (n=22) were female. The other eight (8) invited participants were on official assignments at the time of interview. The age range was between 20 and 60 years and the most common age group was 51-60 at 34% (n=11). All the participants were in full time employment and the majority 75% (n=24) were registered nurses. Thirty-seven percent of the participants had undergone specialty training in midwifery and were working in the maternity and neonatal wards. Table 1 gives details on the participants’ demographic descriptions.
Interview results
The average time for the recorded interviews was 60 min. All interviews were conducted in the dental department staff room at the health center. This was the participants preferred setting because it was readily available at the time of interviews and within their work premises.
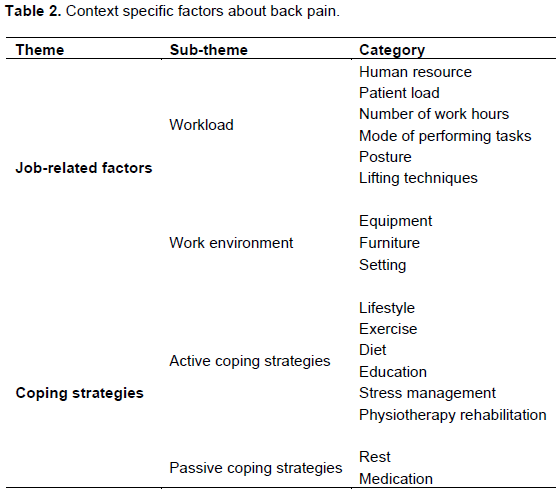
The major themes that emanated from the FGD are outlined in Table 2. These factors are “specific to the context” because they are explicit to these study settings and relate to the information, experiences and incidences as narrated by the participants.
All participants indicated having experienced back pain at one point in the course of their work routines as nurses which has lasted for more than three days for some.
The following elaborates on each theme. Verbatim accounts of participants expressions are presented and illustrations of key statements used have been presented without identifiers beyond ‘participant’, ‘ward’, and ‘FGD’ were the quotes emerged from. Table 3 gives details on the identifiers that have been used.
Participants’ perspectives about context specific factors of back pain experiences
Job-related factors
Workload:
(1) Patient load and human resource: Participants regarded high workload, which involved a high patient load on the wards and outpatient department (OPD) clinics and being inadequately staffed as contributing to their backpain experiences. Participants reported that these demands resulted in exertion because workload on the wards did not warrant them enough time to rest. Additionally, the high demands at work influenced the nurse’s ability to pay enough attention to protecting their back and it influences the quality of service rendered.
“The workload is too much, sometimes there are just too many patients, and maybe only one nurse is taking care of them so, from just doing the nursing of those patients, the back really gets painful.” Female part; Maternity ward, D1
“I would like to add on work overload, sometimes you work alone, on the ward and we don't have enough timeto rest by the time you are knocking off your back and your feet are paining. The patient nurse ratio should really be adhered to because nurses are seeing more patients than they’re supposed to.” Female part; Admission ward, D2
(2) Working hours: Participants resounded that the number of working hours spent on the wards and in direct patient care were too long especially during night duty and the morning to afternoon (07:30 to16:00 h) shift because nurses stand for very long periods. According to the participants, these long hours make their work very stressful resulting in back pain.
“During night duty, especially in labor ward , we are working for so many hours, no time to rest not even a bit. You start at 6:00 in the evening and you are standing the whole night up to 6:00 in the morning, by the time it’s morning, eish, your back is paining. Female part; Maternity ward, D1
“I have especially when I am doing night duty, we are working for so many hours, no time to rest not even a bit, it’s like you go for work, you start at 6:00 pm and you are standing the whole night, by the time it’s morning, your back is paining.” Female part; Admission ward, D3
(3) Mode of performing tasks: Participants expressed that the mode in which most nursing tasks were performed such as suturing, giving medication and bed bathing was also strenuous and a part of most backpain experiences because these activities demand that they assume awkward postures such as kneeling to attend to patients who maybe laying down on the floor. According to the participants narrations their posture during work, included bending, twisting and lifting which if remains unchecked, contributes to their back-pain experiences.
“The other thing is when we are suturing, we need to sit on a comfortable chair but, we are standing and bending most of the time, the moment you finish you can’t even stand up right you can have backache even two or three days.” Female part; Maternity ward, D1
“We usually conduct a diverted outreach and we palpate mothers on the ground, so you have to kneel and bend..you go up and about, bending, doing all sorts of things,…then we have a lot of mothers that we are supposed to palpate, so by the end of palpation you have back pain and it lasts for more than three days.” Female part; Maternity ward, D2
Participants also echoed that often, because of being inadequately staffed, they were using inappropriate lifting techniques during their work routines. This is because sometimes the wards are very busy and there are no fellow nurses or equipment to assist with the lifting or moving of patients. According to the participants, this makes it very difficult for them to apply lifting techniques because a single nurse must perform the tasks alone.
“The other thing is the lifting techniques and all that exercise. Sometimes we are using the wrong techniques when lifting the patients especially when you are alone you even disregard the proper lifting techniques because you must lift the patient from a wheelchair to a stretcher which is slightly high, or from a bed which is high to a bed which is low.” Male part; OPD ward, D1
“…. especially in outpatient’s department with shortage…poor lifting techniques are used like when lifting the patients from the bed to the stretcher and stretcher to bed. I find that very straining to the muscles Male part; OPD ward, D3
Work environment:
(1) Work related equipment: Participants narrated that basic equipment such as stretchers or trolleys, required to assist in moving patients during their work shifts, were either inadequate or unavailable in their context. Participants expressed that this increased their chances of experiencing back pain because nurses are forced to lift or move patients using their own body strength which posed a great risk for back injuries for them. Participants expressed that access to the right equipment and regular education about lifting techniques could prevent the occurrence of back pain.
“There is certain equipment that we can use for lifting patients, transferring patients, and all that but we don’t have at this institution even just basic trolleys, you have to carry a patient from maybe the vitals table to go and see the doctor or to the bed, and all those add towards the back pain.” Male part; OPD ward, D2
“I think especially in patients with staff shortage lifting the patients from the bed to the stretcher and stretcher to bed I find that very straining to the muscles because the equipment that we can use for lifting patients, transferring patients, and all is not there.” Female part; Admission ward D3
(2) Hospital or health facility furniture: Participants also voiced that most of the furniture that was being used in the work place was inappropriate for the type of work that they were doing. The specific furniture mentioned was the nurses’ workstations regarding chairs and desks that were not ergonomically designed or positioned. Participants mentioned that this made them sit at angles which were very uncomfortable and caused them to experience back pain by the end of the day or a session. Additionally, participants also expressed that the patient’s furniture in the wards and clinics were mismatched with the type of nursing activity because they were either too low or too high for them. As a result, this makes them perform most of the nursing tasks using postures that were strenuous and uncomfortable.
“I’ve noticed that most of our furniture is not appropriate for the type of work that we are doing. It’s either too high or too low, uncomfortable so we don’t sit in a position which is comfortable, we tend to sit either at an angle so, by the end of a session, we experience a lot of back pains.” Female part; Admission ward, D1
“In the antenatal wards also, the beds are too low and as you are bending to do all the things you can get backache.” Female part; Maternity ward, D3
“I have also experienced back pain, but the worst was when I was with a patient just almost to deliver. I don’t know whether the bed was slightly low or what, but immediately I tried to move, there was a click on my back and that was it.” Female part; Maternity ward, D2
“But then of course the other thing is being able to provide adequate and proper furniture and equipment, or the stuff to use so that we do not experience some of these back aches that come about because of lack of proper equipment.” Female, part; Maternity ward D3
(3) Work environment/infrastructure: Participants reported a lack of basic facilities such as suitable tea rooms in their work setting. They compared their resting rooms to those of doctors and concluded that nurses had no suitable place to rest, especially during the nightshifts. They expressed that this impacted and contributed to their back pain especially because nurses could only sit to rest on the chairs or tables when there was an opportunity. Participants believed that creating a suitable space was nurses could rest would help relieve stress and minimise the effects of back pain.
“When I look at the infrastructure, it’s like nurses are not considered to say they should have a moment of resting. Doctors are usually given a room where they can rest, but nurses, hey, uh-uh. It’s like nurses should not rest at all.” Female part; OPD ward, D1
Hospital infrastructure was also revealed to contribute to stress related job tasks. Hospital bed space capacity was limited; however, with the dire need for health care, some patients are admitted, even beyond capacity. The latter resulted in some patients being given floor beds. Consequently, this made performing nursing tasks and movements within the wards difficult because of inadequate space.
“Like in the labor ward, sometimes women come when it’s very busy and the beds are full, they deliver on the floor. So, as you are bending to do all the things then you can get backache.” Female part; Maternity ward, D2
Coping strategies for back pain
Participants’ accounts on coping strategies for back pain experiences indicated that individuals employed both active and passive strategies to manage their back pain. Active coping strategies involved taking personal responsibility for pain management, lifestyle activities such as physical exercises, physiotherapy rehabilitation and stress management and attempts to function despite having pain. Passive coping strategies comprised managing pain using an outside source or rest (Carroll et al., 2002), such as utilizing pain relief medication.
Lifestyle
(1) Exercise and diet: A subset of participants believed in lifestyle coping activities such as exercise, a healthy weight and diet to manage their back pain. Furthermore, participants expressed that they used a healthy diet and taking vitamins to build their bodies in order to cope with the demands of the job.
“When I go back home it’s when I deal with the consequences of back pain and that’s when I start doing stretches, I make sure I do a bit of jumping and jumping because if I don’t that day, I will have terrible back pain.” Female part; Admission ward, D1
“If it’s light, at least you’ll be bending, standing up, bending just like that. We are also looking at bones so the diet we need to take more care…...taking calcium supplements, vitamins or fruits in the diet also helps.” Female part; TB ward, D2
“Sometimes even the weight, we need to check our weight or the type of food we are eating. Usually, if you are heavy honestly you find even if you are doing a simple procedure will be difficult. We need to watch our diet because of obesity…. obesity is really an enemy to health.” Female part; Maternity ward, D3
(2) Physiotherapy rehabilitation: Some participants revealed that they attend physiotherapy and engaged in rehabilitation exercise activities to manage and minimize the effects of back pain. They expressed that being taught the correct exercise which could be done during work, such as proper stretching, would further help them in coping with back pain.
“I do physiotherapy exercises everyday because I noticed that if I don’t do physio in the morning, I won’t even be able to work. So, I do the exercises that I was taught, but if the pain is too much, I end up seeing the physiotherapist for a few physio sessions so that maybe they massage me a bit, then the pain goes.” Female part; Maternity ward, D2
(3) Stress management: Participants in the FGDs mentioned that they were stressed due to work pressures well as financial stressors which contributed to body and back pains. Participants acknowledged that even if they knew about stress management and managed patients with stress, they experienced challenges managing their own stress levels.
"And stress management though we don't know how to manage our stress. We are very good at caring for the patients, but for ourselves, it's not there. You know we are stressed financially, so with stress literally the whole body is aching, but we are not able to manage our bodies adequately.” Female part; Maternity ward, D3
Use of pain relief medication and rest
Most participants reported resting and using pain relief medication to cope with back pain. Pain relief medication was the most frequently used coping strategy.
“When you have the back ache, of course what usually happens is you are given pain killers and a sick note to go and rest until you feel better. I feel its part and parcel of the job, it’s something that will come and go eventually. So, …I take a couple of Paracetamols or Brufen and continue with work.” Male part; OPD ward, D2
“When experiencing the back pain…. that back pain won’t finish within a day. It will take you for two to three days, it’s still there, unless you take a Panadol, then you will feel like it subsides. And because now we are aging Panadol does not even work so, we take something heavier…. you go to an extent of taking Diclofenac.” Female part; Maternity ward, D3
“I have experienced back pain and even now I have back pain. When I stand, that’s when it’s even worse. I took a short leave, I thought when I went on a short leave, I will feel better, but the pain is still there and it’s like increasing.” Female part; Maternity ward, D1
Notably one participant mentioned having changed work departments to cope with the effects of back pain. However, the participant also expressed that this didn’t help much, resulting in the participant opting to use pain relief medication on a regular basis. Another participant explained that apart from use of pain relief medication, she also uses an orthopaedic belt to obtain back pain relief.
“I changed, we went to the orthopedics, yah. I’m still having the same pain, now every night I must take a painkiller.” Female part; Admission ward, D1
“I keep on taking some painkillers … then my belts every day, I have to put on belts to help me relief the back pain.” Female part; Maternity ward, D3
DISCUSSION
The nursing profession is an essential and large component of the healthcare workforce. Back pain experienced by nurses can have a negative impact on personal well-being, patient care and health system efficiency and costs. It is therefore important to identify factors that contribute to their back-pain experiences; as this information may play an essential role in developing interventional approaches that can promote well-being (Abedini et al., 2014). This study aimed to explore the perspectives about context specific factors and coping strategies for back pain experiences among nurses, in Lusaka, Zambia.
Findings in this study revealed that nurses perceive several work-related contextual factors to be linked to their experience of back pain. The factors are job-related and work environment. Job-related factors include workload influenced by work hours, human resource and mode of performing tasks, while work environment involves the infrastructure and facility furniture. Aspects of work load which includes reduced human resource, high number of patient load, long working hours and mode of performing tasks were context factors that were identified in this study. The number of working hours spent on the wards and in direct patient care were said to be too long especially during night duty. The mode in which most nursing tasks were performed was described too strenuous because nursing postures during work, includes bending and twisting. These findings are similar to the reported high demands of nursing work in hospitals in Tanzania (Mwilila and Frantz, 2008) and the United States of America (Geiger-Brown et al., 2004). In addition, demanding working conditions such as long hours, heavy lifting and low staffing levels exerted a personal toll that reduced quality of life for nurses even during off hours (Geiger-Brown et al., 2004; Mwilila and Frantz, 2008). High demands, including a wide range of tasks and duties, lack of adequate personnel and lifting heavy objects were also described as problems that increased the probability of experiencing back pain among the nurses in the United Kingdom (Boniface et al., 2016) and Iran (Abedini et al., 2014). Although these outcomes for high income and lower to middle income countries are compared, it is important to note that the work conditions and the contextual factors of these settings may not be comparable (Semachew et al., 2018). For high income countries, the actual conditions and standards for nursing work may be better, compared to those of lower to middle income countries which often operate on limited heath care budgets and are compounded by a higher disease burden (Boughattas et al., 2017).
Awkward postures assumed during work activities including inappropriate and poor lifting techniques were constantly connected with back pain experiences in the present study. This aspect has also been expressed in other studies (Heidari et al., 2019; Mwilila and Frantz, 2008; Geiger-Brown et al., 2004) and is worsened by lack of equipment and poor work settings. Repetitive postures and movements may be a cause of cumulative pressure to the musculoskeletal system causing back pain among nurses. Nurses routinely perform activities such as lifting and transferring patients in/out of the bed or from the floor. These activities are repetitive, labour intensive and involve direct contact with the patients (Chung et al., 2013). In the current study, participants specified assuming awkward postures because the patient beds were either too high or too lower for them and sometimes because of high patient turn-out, some patients were nursed on floor beds. This may suggest that even though postural and handling techniques are taught during training, staff shortages and lack of equipment may make it difficult for nurses to practice the techniques effectively.
Nursing activities assume lots of physical care that involves movement and patient support which sometimes may have unpredictable events due to weight and poor gripping which may lead to injuries for the nurse (Alnaami et al., 2019; Heidari et al., 2019). These outcomes may suggest that there is a mismatch between job activities performed by nurses to meet work demands and their physical abilities or the need for more advanced technologies and/or equipment to assist with the load. However, some of these job activities may be controlled by the individual nurse and could also be corrected through training although; it may not be the ultimate remedy. Therefore, prevention activities must be directed towards enhancing work practice capacity such as providing educational programs, raising self-awareness and encouraging proper physical activity, stretching exercises, and instructions personal coping strategies in response to back pain experiences (Richardson et al., 2019). The aforementioned factors may allow nurses to have personal control of their work situation and subsequently may decrease the occurrence and severity of back pain injuries. Additionally, increasing the staffing capacity would not only benefit the nurses’ health but will also improve the quality of health care services that is provided to patients.
Working environment with regards to equipment, furniture and settings were also identified as being unavailable, inadequate or inappropriate for the type of work that nurses do. Additionally, lack of basic facilities such as tea rooms where nurses could rest was also mentioned as a factor that composited their back-pain experiences. Similar impressions of participants’ perspectives about work settings, inappropriate furniture and lack of equipment were also expressed as factors for back pain experiences among nurses in Tanzania (Mwilila and Frantz, 2008). Other studies (Richardson et al., 2019; Abedini et al., 2014) also identified that the absence of hospital equipment particularly for lifting and moving obese patients accounted for the risk of back injury among nurses. These accounts show that work environment, not being functionally adapted for routine tasks that nurses perform, may hinder nurses from putting into practice functional and injury prevention skills they acquire during training. Earlier studies (Richardson et al., 2019; Geiger-Brown et al., 2004) have suggested that problematic work settings faced by nurses may be addressed by redesigning the work place setting, and provision of lifting equipment and appropriate furniture. This approach is recommended because it reduces the risk of back injury by minimizing the demands on the worker if used correctly. Though, in low-income settings this may remain unattainable because of budget constraints and nurses have little or no control over this work situation. But for optimal health and well-being of nurses, it is essential that their work environment be a key budget consideration to warrant redesigning of infrastructure and provision of the appropriate equipment and furniture. Modifying equipment or some features of the working system to reduce risk of back pain injury among the nurses may also be achieved by promotion of multiple approaches in the work place. This would include developing a culture of safety, manual handling training in clinical contexts, making changes in workflow, staffing support to allow teamwork and access to available equipment (Richardson et al., 2019). For low-income settings, these activities are practical as they may draw minimal budgeting. A lack of attention to these important factors may lead to a loss in workforce with a direct impact on patient care.
Participants’ coping strategies for back pain experiences demonstrated the use of both active and passive strategies. While use of pain relief medication was widely used, physical exercises, physiotherapy rehabilitation, dietary supplements, stress management and rest were other strategies implored. Other studies have also reported use of pain medication, dietary supplements (Mwilila and Frantz, 2008), stress management, physiotherapy or occupational therapy as coping strategies for back pain (Richardson et al., 2019; Geiger-Brown et al., 2004). These studies also identified the elimination of stooped working positions, a no lift policy and use of lifting teams as strategies for minimizing the effects for back pain (Richardson et al., 2019; Geiger-Brown et al., 2004). Elimination of stooped working positions where nurses are encouraged to sit down at the bedside is achievable in low-income settings and can be enhanced through training. However, because of inadequate staffing levels the nurse and patient ratio at a given time may hinder the performing of nursing activities in sitting position because nurses may work to get their work assignments done. Change of jobs was also a coping strategy that was reported in previous studies (Richardson et al., 2019; Boniface et al., 2016; Geiger-Brown et al., 2004). This option for most low-income settings is not practical because the opportunity for job changes is limited. Using active self-management strategies to cope with back pain especially in low income settings appear to be an approach that can substantially reduce the levels of back pain and disability. This is because active self-management strategies can reduce pain efficacy beliefs, depressive symptoms and fear avoidance beliefs (Crowe et al., 2010). Active coping strategies may also lead to behaviour modification or a change in attitudes, abilities, or coping strategies (Richardson et al., 2019). This may be beneficial in promoting health and well-being among nurses in their work settings.
Notably in this study, some participants echoed that some of their back pain discomforts were due to stress. However, even though they managed other people with stress, they had difficulty in managing and coping with their own stress. Factors like excessive workload, lack of social support and not having enough control over job-related decisions may cause cumulative stress that can interfere with physical health and performance (Segal et al., 2018). This suggests that developing and incorporating support system that would promote physical stress relief such as relaxation and stretch exercise activities in the work settings may help nurses to regain their balance.
LIMITATIONS
It is important to note that participants were sourced from one health care centre in the per-urban region of Lusaka. Hence, their perspectives may be specific to their work context and may thus only be generalizable to similar contexts. The participants reflected on their own perspectives about back pain; and they were exposed to several different other factors that interact which could be the cause of back pain disability. However, even though the outcomes from this study are specific to participants who took part in these study similar situations may occur in other settings.
CONCLUSION
Nurses identified context specific factors as job-related factors comprising workload factors and work environment factors as the main contributors for back pain. Workload factors were high workload, inadequate human resources, high patient load, long work hours and mode of performing tasks; while environmental factors comprised equipment, furniture and work settings. To cope with back pain, participants used both active and passive strategies such as physical exercises, physiotherapy rehabilitation, dietary supplements, stress management, pain relief medication and rest. To address the problem of back pain in nurses, a multipronged approach involving health care system factors, infrastructure, organisational factors and education is advocated.
ACKNOWLEDGEMENT
The authors appreciate the financial support and sponsorship from the National Research Foundation (NRF) (No:105219) in South Africa.
CONFLICT OF INTERESTS
There are no conflicts of interest.
REFERENCES
|
Abedini S, Morowatisharifabad MA, Enjezab B, Barkhordari A, Fallahzadeh H (2014). Risk Perception of Nonspecific Low Back Pain among Nurses: A Qualitative Approach. Health Promotion Perspectives 4(2):221-229 |
|
|
Abou El-Soud AM, El-Najjar AR, El-Fattah NA, Hassan AA (2014). Prevalence of low back pain in working nurses in Zagazig University Hospitals: an epidemiological study. Egypt Rheumatology Rehabilitation 41(1):09-15. |
|
|
Alnaami I, Awadalla NJ, Alkmaar M, Alburidy S, Alqarni A, Algarni A, Mahfouz AA (2019). Prevalence and factors associated with low back pain among health care workers in southwestern Saudi Arabia. BMC Musculoskeletal Disorders 20(1):56-61 |
|
|
Boniface G, Ghosh S, Robinson L (2016). District nurses' experiences of musculoskeletal wellbeing: a qualitative study. British Journal of Community Nursing 21(7):350-355 |
|
|
Boughattas W, ElMaalel O, Maoua M, Bougmiza I, Kalboussi H, Brahem A, Chatti S, Mah-joub F, Mrizak N (2017). |
|
|
Low Back Pain among Nurses: Prevalence, and Occupational Risk Factors. Occupational Diseases and Environmental Medicine 5:26-37. |
|
|
Carroll L, Mercado AC, Cassidy JD, Côté P (2002). A population-based study of factors associated with combinations of active and passive coping with neck and low back pain. Journal of Rehabilitation Medicine 34(2):67-72. |
|
|
Chan SG (2017). Factors Associated with Low Back Pain Among Nurses in Critical Care Units, Hospital Universities Malaysia Age (years) 20(30):31-40. MS.ID.000613. |
|
|
Chung YC, Hung CT, Li SF, Lee HM, Wang SG, Chang SC, Pai LW, Huang CN, Yang JH (2013). Risk of musculoskeletal disorders among Taiwanese nurse's cohort: a nationwide population-based study. BMC Musculoskeletal Disorders 14:144-147. |
|
|
Cresswell JW (2013). Qualitative inquiry and research design: Choosing among the five approaches. Thousands Oaks, CA: SAGE Publications Inc., pp. 77-83 |
|
|
Crowe M, Whitehead L, Gagan MJ, Baxter D, Panckhurst A (2010). Self-management and chronic low back pain: a qualitative study. Journal of Advanced Nursing 66(7):1478-1486. |
|
|
Dlungwane T, Voce A, Knight S (2018). Prevalence and factors associated with low back pain among nurses at a regional hospital in KwaZulu-Natal, South Africa. Health SA Gesondheid 23(0):a1082. |
|
|
Geiger-Brown J, Trinkoff AM, Nielsen K, Lirtmunlikaporn S, Brady B, Vasquez EL (2004). Nurses perception of their work environment, health and well-being: A qualitative perspective. Aaohn Journal (52)1:16-22 |
|
|
Heidari M, Borujeni MG, Rezaei P, Abyaneh SK (2019). Work-related musculoskeletal disorders and their associated factors in nurses: A cross-sectional study in iran. The Malaysian Journal of Medical Sciences 26(2):122. |
|
|
Johnson OE, Emmanuel E (2016). Prevalence and risk factors of low back pain among workers in a health facility in South-South Nigeria. British Journal of Medicine and Medical Research 11(8):1-8. |
|
|
Kay K, Evans A, Glass N (2015). Moments of speaking and silencing: Nurses share their experiences of manual handling in healthcare. Collegian: The Australian Journal of Nursing Practice, Scholarship and Research 22(1):61-70. |
|
|
Mwilila MC, Frantz J (2008). Work-related low back pain among clinical nurses in Tanzania. Unpublished master's thesis.etd.uwc.ac.za/xmlui/handle/11394/2781. |
|
|
Nkhata LA, Esterhuizen TM, Siziya S, Phiri PDC, Munalula-Nkandu E, Shula H (2015). The prevalence and perceived contributing factors for work-related musculoskeletal disorders among nurses at the University Teaching Hospitals in Lusaka, Zambia. Science Journal of Public Health 3(4):508-513. |
|
|
Richardson A, Gurung G, Darrett S, Harcombe H (2019). Perspectives on preventing musculoskeletal injuries in nurses: A qualitative study. Wiley Open Nursing, pp. 1-5. |
|
|
Segal J, Smith M, Robinson MAL, Segal R (2018). Stress in the workplace. |
|
|
Semachew A, Workineh Y, Ayalew E, Animaw W (2018). Low back pain among nurses working in clinical settings of Africa: A systematic review and meta-analysis of 19 years of studies. Bio Rxiv, p.507053. |
|
|
Thomas PY (2010) Towards developing a web-based blended learning environment at the University of Botswana. PhD Dissertation. University of South Africa. |
|
|
Varga-Atkins T, McIsaac J, Bunyan N, Fewtrell R (2011). Using the nominal group technique with clickers to research student experiences of e-learning. A project report written for the ELESIG Small Grants Scheme Liverpool: University of Liverpool. |
|
|
Woolf SH, Aron L National Research Council (2013). Physical and Social Environmental Factors. In: US Health in International Perspective: Shorter Lives, Poorer Health. National Academies Press (US). |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


