Full Length Research Paper

ABSTRACT
Nurses are faced with a lot of responsibilities, at work and home. This gives rise to work-family conflict. There are several factors which could affect work-family conflict. This study identifies specific job characteristics and their influence on work-family conflict among nurses working in the teaching hospitals in Anambra State. Descriptive survey design was adopted for the study, as a proportionate sampling technique was used to select 257 nurses from the two teaching hospitals in Anambra State. The instrument for data collection was work-family conflict instrument, and Work-design questionnaire which was adopted, modified and revalidated. The data generated was statistically analyzed using Kruskal-Wallis and Spearman correlation with the aid of Statistical Package for Social Science (SPSS) version 23. Results stated that high level of work-family conflict was reported by nurses. Average number of patients served per day and workload influenced work-family conflict positively with a p-value of 0.044 and 0.00, respectively. Workload and average number of patient served per shift are the job characteristics that influence work-family conflict. Therefore, workload of nurses should be analyzed critically and the review of nurses workload for further adjustments so as to increase their productivity both at work and home.
Key words: Job characteristics, work-family conflict, workload, job autonomy, Nigeria, Anambra State.
INTRODUCTION
Nurses are primarily involved in taking care of the infected (Makola et al., 2015). Same as other employees in different fields, nurses are faced with the demands of work and home responsibilities as their main daily tasks (Makola et al., 2015), and juggling between these two spheres is part of everyday life for millions of employees across the globe (Lembrechts et al., 2015; Karimi et al., 2012). Recently, in the health sector, there has been an increase in competitive pressures, which has led to increase in time demands on workforce so as to increase productivity, leaving less time available for the employees to be with their families (Akintayo, 2010). This has led to difficulty in combining work and family responsibility, which makes work-family conflict an important issue in the 21st century (Harrington and Ladge, 2009).
Work-family conflict is a type of conflict that exists when responsibilities from work and family domain are not compatible. This makes it difficult for the individual to cope as a result of the arising pressure from either work or family roles (Ogbogu, 2013; Greenhaus and Beutell, 1985). Today, in Nigeria, more than 90% of employees are faced with the challenges of work-family conflict (Ugoani, 2013). Among Nigerian female medical doctors and nurses, work-family conflict also exists (Fang, 2017).
The imposition of roles from work on family roles leading to work-family conflict could occur from three sources (Akhigbe and Koleoso, 2016); they are time-based conflict, strain-based conflict and behavior-based conflict. Time-based conflict may occur when time devoted to one role (work role) makes it difficult to participate in another role (family role). A strain-based conflict arises, when experience in one role (work role) spills over into another role (family role) and interferes with participation in the family role (Akhigbe and Koleoso, 2016). This may be influenced by the strain factors such as stress, fatigue, tension, and anxiety. Behavior-based conflict as one of the source of conflict occurs when specific behaviors required in one role are incompatible with behavior expectation in another role (Akhigbe and Koleoso, 2016).
In as much as work-family conflict could arise from these broad sources, specifically, the determinants of work-family conflict could be work-related factors of which in this study, job characteristic is considered. Job characteristics of nurses include: task variety, job autonomy, job schedule, average number of patient served per shift, and workload (Michel et al., 2011). Cho et al. (2006), defined workload as the relationship between the work demands that are placed on an employee given a specified amount of time and resources. Autonomy also was seen as the amount of job-related independence, initiative, and freedom, either permitted or required in daily work activities” (Finn, 2001), these are the component of nurse’s job characteristics.
Nursing is considered a profession which, despite being a fulfilling and satisfying job (Duffield et al., 2009), can be impaired due to, inability to handle responsibilities arising from both domains. In order to increase productivity at work several strategies was devised to curtail the incidence of work-family conflict among nurses. Among such strategy is the presence of co-workers supports to accommodate seasonal fluctuations, annual, maternity, study, and sick leave, ensuring that work stress is reduced (Mordi et al., 2013; Deery, 2008). Despite all these strategies, research still has it that nurses experience a high level of burnout and poor level of job satisfaction which is seen to be the outcome of work-family conflict (Khamisa et al., 2015). This raises the question; what is the level of work-family conflict among nurses in the teaching hospitals and which job characteristics has influence on work-family conflict? This becomes imperative to establish effective strategies that will have a greater influence on work-family conflict among nurses. Therefore, the aim of this study was to investigate job characteristics and its influence on work-family conflict among nurses in the teaching hospitals in Anambra State, Nigeria.
MATERIALS AND METHODS
Study setting, design and participants
Descriptive survey design was adopted for this study. It is a research design with its main objective, as the portrayal of characteristics of a person, phenomenon, situation, population or group, or the frequency with which certain phenomenon occur (Polit and Beck, 2010). The study was conducted in two teaching hospitals in Anambra State: Nnamdi Azikiwe University Teaching Hospital (NAUTH), Nnewi and Chukwuemeka Odumegwu Ojukwu University Teaching Hospital (COOUTH), Amaku from September 1 to November, 2018. The two tertiary health institutes consist of various departments with health workers manning each unit. It also covered several numbers of clinics and wards. The units were further divided into eight job units for each teaching hospital, it entails: CSSD, Emergency unit, Surgical unit, Medical unit, Clinic, Nursing admin/CEU, ICU/SCBU, Maternity/Gynecological unit. The participants of the study were registered nurses of all cadres, both males and females, working in the two health institutes for at least one month, emotional and physical stability, and willingness to participate in the study (Nursing services, COOUTH and NAUTH, 2017-2018).
Sample size determination and sampling procedure
The total population of nurses working in the teaching hospitals is 565 (Nursing services, COOUTH and NAUTH, 2017-2018). In COOUTH, there are 170 nurses and 395 nurses in NAUTH. This comprises nurses in all the cadres and in different wards. A sample size of 257 (inclusive of 10% attrition rate) of nurses working in the teaching hospitals in Anambra State was obtained using the Taro Yamani’s (Yamane, 1973) formula for known population, of which COOUTH was 77 nurses and NAUTH was 180 nurses. To select a representative sample size for each unit from each sampling, a proportionate sampling was utilized using a formulae (ns = Ns × n / N) (Amogu, 2001, unpublished).
Data source and procedures
The instrument for data collection was a questionnaire adopted to fit into research objectives. The questionnaire was derived from work-family conflict questionnaire by Carlson et al. (2000) for measuring work family conflict. It consists of 8 items. Work design questionnaire for job characteristics by Morgeson and Humphery (2006) was used to investigate the job characteristics of nurses. The questionnaire consists of 30 items, divided into three sections. Section A contained the demographic data, which is characterized by questions 1-11. Section B, dealt with job characteristics which covered items 12-22 (working hours; item 12, average number of patient served per shift; item 13, work schedules; item14, work load; items 15-17, task variety; items 18-19, and Job autonomy; items 20-22). Section C covered work-family conflict; items 23-30. Collection of data was done by the researchers, from individuals that met the inclusion criteria. Filling of the questionnaire was based on convenience in the various units of the teaching hospitals by the nurses. Response from each questionnaire was reviewed and checked for completeness by the principal investigator. Data collection lasted for two months when a sample size of 257 was reached though only 210 were valid, as this were the nurses that completed their questions. The return rate was 82% of the stimulated sample size of 257 nurses from the two teaching hospitals.
Data processing and analysis
The collected data were analysed using both descriptive and inferential statistics. This analysis was done with the aid of Statistical Package for Social Science (SPSS) version 23 and Microsoft Excel 2007. Results were presented in tables. The descriptive statistics-frequency, percentage, mean and standard deviation were used to summarise the items of the questionnaire. Specifically, the mean and standard deviation were used for the Likert scale items. The Kruskal-Wallis and Spearman Correlation were the inferential statistics used. Job characteristics that was considered in this study include, working hours per day, task variety, work schedule, job autonomy, average number of patients served per shift and organizational support/co-workers support.
For the computed variables used in the inferential statistics such as work-family conflict (WFC) score. Negatively structured items were reversed before this summation. For WFC specifically, the WFC score was also categorised into a binary (high or low) data. A nurse was classified to have high WFC if score is above an expected average of 24 and classified to have low WFC if otherwise. The expected average is obtained by summing the item averages of 3 (that is, mean/midpoint for 5 point scale) for the 8 items. Statistical significance was made at p value<0.05 in this study.
Data quality control
The instrument used for data collection was a standardized instrument that has its standardized value for reliability of instrument, work-family conflict instrument had a Cronbach alpha statistics value of 0.89, and work design questionnaire showed a high internal consistency value of 0.87.
Data quality was assured by carrying out the careful design of data extraction instrument, appropriate data collection by researchers. Intensive supervision was done by principal investigator during the whole period of data collection. Reliability of instrument and its validation was done before data collection. Daily, the data were strictly revised for completeness, consistency, accuracy and clarity by the investigators. Data obtained was held in high level of confidentiality. In addition, the data were thoroughly and carefully entered into the computer using Microsoft Excel 2007.
Ethical statement
Ethical approval was obtained from Nnamdi Azikiwe University Teaching Hospital Ethics committee. Following the approval, a letter was written through the Head of Department (HOD) Nursing Science, Nnamdi Azikiwe University, Nnewi to NAUTH Research committee. Attached to the letters was the research proposal. Permission was obtained from unit heads. The purpose of the study was explained to the respondents and an oral informed consent was obtained from the respondents before the administration of the questionnaire. The confidentiality of information was maintained by not recording their names in the instrument for data collection.
RESULTS
Socio-demographic characteristics
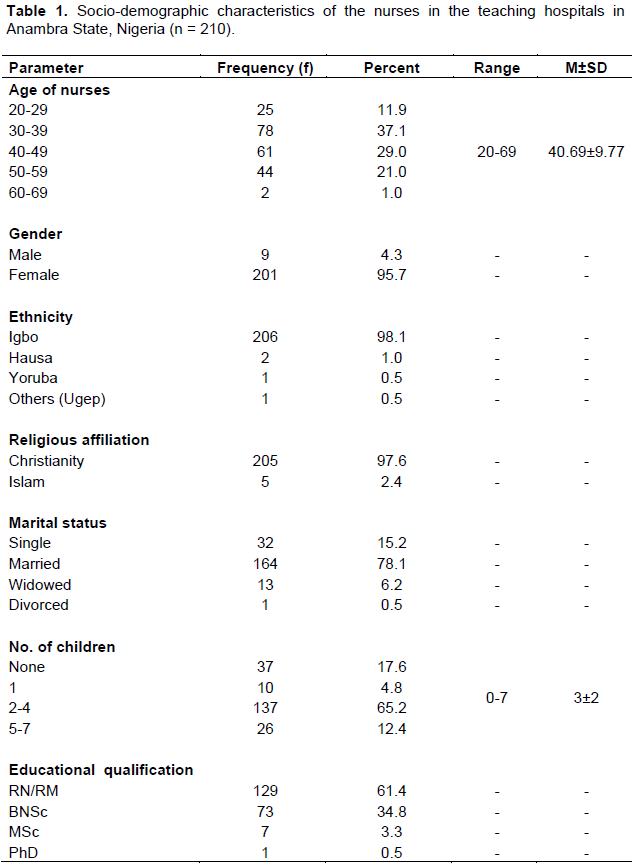
Two hundred and ten (210) nurses working in different unit irrespective of their cadre were analysed. They were aged between 20 and 69 years with mean and standard deviation of 40.69±9.77 years and modal age group of 30 to 39 years (37.1%). The nurses were predominantly females (95.7%), Igbo by ethnicity (98.1%) and Christianity (97.6%) by religion. Majority were married (78.1%); the number of their children ranged from 0 to 7 with mean and standard deviation of 3±2 children, and majority with 2 to 4 children (65.2%). For majority of the nurses had RN/RM qualification (61.4%) followed by those with BNSc. (34.8%) (Table 1).
Job characteristics of nurses
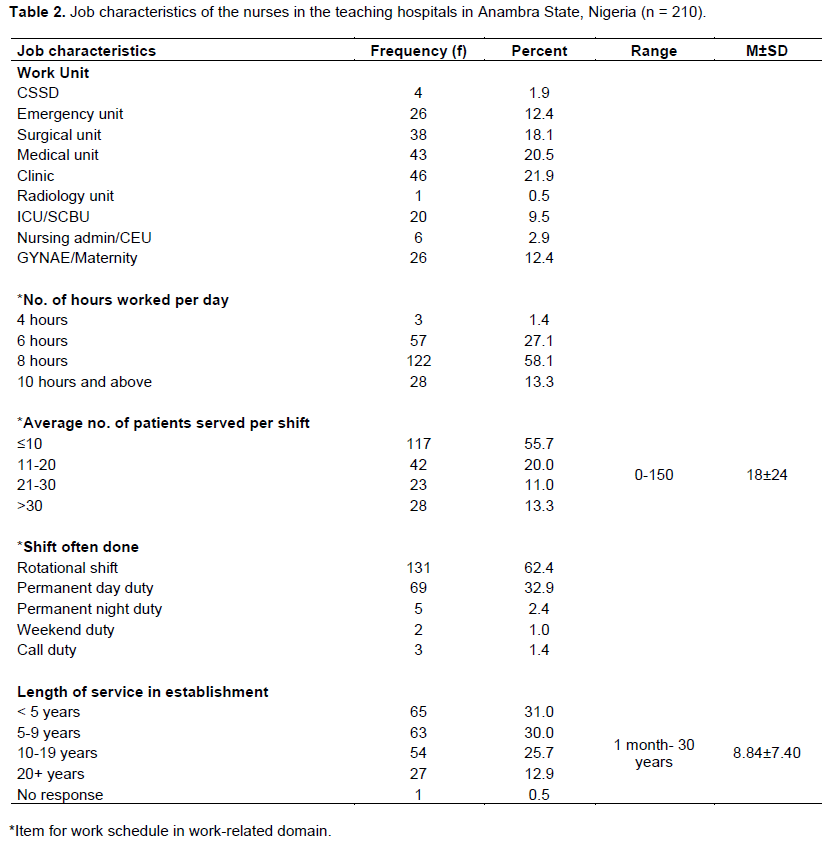
For the job characteristics, nurses professional rank was distributed across Nursing Officer II (31.0%), Nursing Officer I (21.9%) and Chief Nursing Officer (19.5%). The job units of the nurses were thus distributed: clinic (21.9%), medical unit (20.5%), surgical unit (18.1%), emergency unit (12.4%), Gynae/maternity (12.4%), ICU/SCBU (9.5%), nursing administration/CEU (2.9%), CSSD (1.9%), and radiology unit (0.5%). Majority of the nurses worked 8 h per day (58.1%). The average number of patients served per shift ranged from 0 to 150 with mean and standard deviation of 18±24 and majority serving 10 or less (55.7%). The shift often done was majorly rotational (62.4%) followed by permanent day (32.9%). The nurses’ length of service ranged from 1 month to 30 years with mean and standard deviation of 8.84±7.40; majority have served below 10 years (61.0%) (Table 2).
Level of work-family conflict among nurses
The two most common forms of the conflict amongst them were such that: ‘after work, they come home too tired to do some of the things they would like to do’ (3.91±1.10) and ‘due to work-related duties, they frequently have to make changes to their personal plans’ (3.80±1.05). Other forms of the conflict experienced though slightly above average were: ‘their work schedule often interferes with their family life’ (3.42±1.28); on the job they have so much work to do that it takes away their personal interests’ (3.31±1.19); their work takes up time that they would like to spend with their family’ (3.10±1.24); and the amount of time their job takes up makes it difficult to fulfil family responsibilities’ (3.01±1.27) (Table 3).
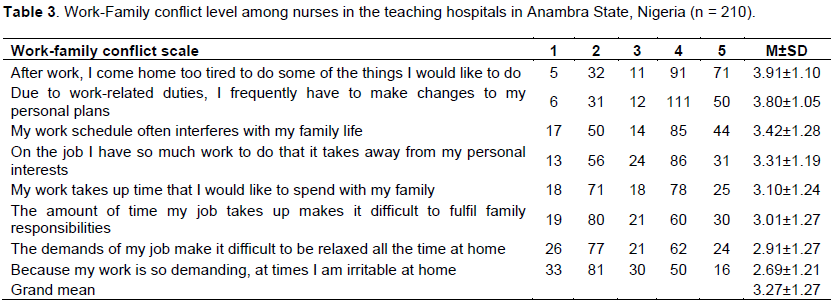
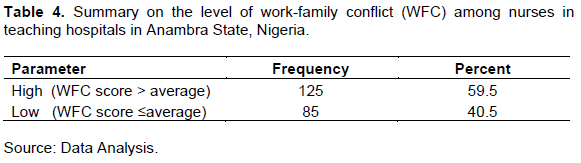
In general, work-family conflict was somewhat above average (3.27±1.27) (Table 4). Majority of the nurses have experienced the conflict (59.5%); hence the conflict was somewhat high.
Job characteristics as a determinant of work-family conflict
The considered domains include, working hours and average number of patients served per shift workload, task variety and job autonomy. Working hours per day, task variety and job autonomy were non-determinants of work-family conflict as no significant relationship existed between them (Table 5).
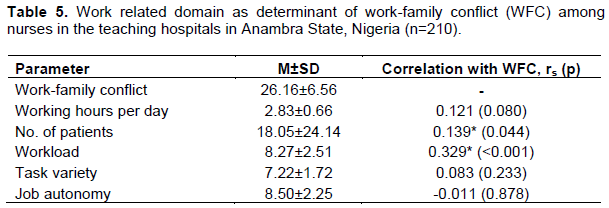
Specifically, for average number of patients served per shift, nurses that served more patients were predisposed more to work-family conflict; and likewise those that had more workload. Shift often done was non determinant of work-family conflict as no significant difference existed between work-schedule (c2 (2) = 1.707, p = 0.426) (Table 6).
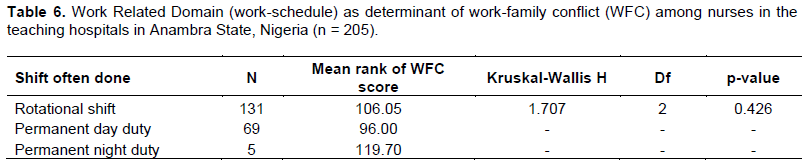
In other words, no work-schedule group was predisposed more than the other. Hence, the conflict level was the same for the different schedule (irrespective of the seemly difference in the mean rank): permanent night (119.70), rotational shift (106.05) and permanent day (96.00).
DISCUSSION
This study was designed to determine the influence of job characteristics on work-family conflict among nurses. In general, the findings showed high level of work-family conflict among nurses in the teaching hospitals in Anambra State with a grand mean score of 3.27 in Table 3.
Working hours per day, task variety, work schedule and job autonomy had no influence on work-family conflict, whereas average number of patients served per shift and workload indicated its influence on work-family conflict.
This indicates that work interference with family roles or responsibilities is high among nurses. This could be as a result of the fact that most respondents reported that after work they return home too tired to do things they could love to do. A mean value of 3.8 was associated with respondents who make changes in their personal plans so as to meet up with their duties at work. This reason is in line with work done by Ozor et al. (2016), which states that work-family conflict increases as there is a reduction in personal accomplishment and emotional exhaustion. Individuals who are certainly not able to satisfy their personal plans (which may be quite different from that of their job) may be prone to work-family conflict. Tiredness from job is also seen as a restriction, since other duties allocated to a particular time will be shifted or not done at all. This may affect the nurse in question. Societal factors could also be the reason for the high level of work-family conflict, as majority of the respondents are females (95.7%), and in the eastern part of Nigeria, there is an understanding that women are the builders of their home; hence, the home comes first before their jobs. This brings about a societal expectation, whereby the woman struggles to meet up with the expectation in her home and the organizational expectations. It has also been seen that the expectations at home are different from the expectations at work.
As regards to job characteristics, Sabil et al. (2016) on identifying work-family conflict among Nurses in Sarawak General Hospital, Malaysia, stated that one of the factors contributing to work family conflict among nurses is workload. This could be seen in majority of the respondents (86) indicating with a mean value of 3.31, that in their job they have so much to do that it takes away their personal interest. It was also seen that the personal interest of the nurse may be ignored as majority of the respondent also stated that they do not have much influence on their job as to change what has been planned. Nurses’ jobs are said to be tasking as they are major stakeholders in the medical profession. This is said to be so as the total number of patient to be cared for per shift is not determined by the number of patient available at the resumption of duty. There could be new admissions, emergencies, and increased number of patients that is unbooked in the clinic. The professional nurse cannot state the exact number of patients who are expected in the hospital, in a particular day. As this uncertainty may bring about increased workload, as patient must be attended to, especially the critical ill patient in order to promote health. This may bring about stress as they are stretched beyond their capacity, which is a product of work-family conflict.
This current finding is in line with work done by Mansour and Tremblay (2016), which states that increased workload, leads to work stress through work-family conflict.
Furthermore, from the socio-demographic characteristics, 55.7% of the respondent served ≤10 patients which is not in line with the standardized number of nurse-patient ratio, which is 1:4 depending on the state of the patient. Critically-ill patients may require 1 nurse:1 patient, this is not seen to be applicable in the teaching hospitals, which is the standard of Nursing and Midwifery Council of Nigeria. Inability to meet up with this standard has been related to shortage in workforce. Shortage in the number of nurses will help to increase workload. Few nurses who are assigned to manage numerous patients will be subjected to over labour. This could be a strong contributor to work-family conflict as nurses over labour to care for the number of patient assigned to them. This also affects the quality of care rendered. This could also guide the fact that work overload increases work-family conflict.
For the non-determining factors, working hours could be seen to have no significant relationship with work-family conflict, because it was seen from the result that majority of the respondents worked for 8 h (58.1%), which is considered to be the shortest number of hours a professional nurse could work. Irrespective of the fact that there are other factors that could lead to work-family conflict, the number of working hours is not a contributing factors, as this is the least number of hours an individual can work in a hospital setting. Rather, there could be other factors which can bring about the presence of work-family conflict.
For task variety, it could be as a result of the presence of most respondent (142) indicating that they do come up with new ideas under personality domain. Individuals who seem to come up with new ideas may not find it difficult in the midst of various tasks, as they are also curious to know the outcome of every particular task. Moreover, nursing profession is filled with numerous task, to be done on a patient and are being carried out scientifically, knowing the rationale for every action and the theory that guides the practice. All these training, are been inculcated during the period of learning for the nurse in prospect. It is assumed that the professional nurse is acquainted with this task, though not easy, yet not strange to the nurse. This may make task variety not significantly related to work-family conflict. This result disagrees with work done by Michel et al. (2011) on the antecedents of work-family conflict: a meta-analytic review, which states that task variety as a component of work characteristics is an antecedent of work-family conflict. The researcher findings could be narrowed down to the profession or individuals involved which could be one of the reasons for the variation. Finally, for job schedule and job autonomy, most of the respondents (77) have influence on the decision that pertains to their work schedule not the job itself. Provisions could have been made in the hospital for this so that individuals who have some functions to attend can easily identify the date and necessary adjustment could be made within the period of drafting out the roaster. Period of off-duty can still be of benefit to the nurse without having or generating conflict. Recent finding is not in line with work done by Zito et al. (2013), on job demand and work-family conflict in a health care staff in Northern Italy: the role of shift works, this state that work-shift influences work family conflict, work-family conflict is higher in shift work than their colleagues without shift work and on-call. The reason for the contradiction could be because majority of nurses in Nigeria do shift work, and when there is a change in schedule either by position or responsibility it comes with slight increase in remuneration, so it rarely makes any difference. The limitation of this study was based on willingness of nurses to fill the questionnaire due to increased workload, therefore those with incomplete information were excluded from the study.
CONCLUSION
The major findings of the study were that in general, the level of work-family conflict was high among nurses working in the teaching hospitals in Anambra State. Among the job characteristics, working hours, task variety, job schedule and job autonomy were non-determinant of work-family; no significant relationship existed between them, whereas average number of patients served per shift and workload were of greater influence on work-family conflict with positive relationship among nurses.
RECOMMENDATIONS
Nurse managers/head of nursing services should establish policies that will guide and enhance work-life balance, allowing individual to work at their pace and are still paid based on their request. Nurse managers and administrators should work together with the Nursing and Midwifery Council of Nigeria (NMCN) to see that the implementation of the recommended ratio of nurse to patient is achieved first, in all tertiary institution, which will set the pace for others to follow. Finally, incorporate seminars, symposium on work-family conflict as part of the orientation of new staff, exposing the causes, effect and how to handle work-family conflict. This will make the professional nurse alert so as to stand against the incidence or causes of work-family conflict, having been fully informed. This will reduce the incidence of increased workload, thereby reducing work-family conflict. Further study could be done on other factors that could influence work-family conflict.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Akhigbe K, Koleoso O (2016). The role of age, job experience, educational attainment, and length of marriage in work-family conflict of married nurses. African Journal for the Psychological Study of Social Issues 16(2):56-68. |
|
|
Akintayo D (2010). Work-Family Conflict and Organization Commitment among Industrial Workers in Nigeria. Journal of Psychology and Counseling 2(1):1-8. |
|
|
Carlson D, Kacmar K, Williams L (2000). Construction and initial validation of a multidimensional measure of work-family conflict. Journal of Vocational Behavior 56:249-276. |
|
|
Cho J, Laschinger H, Wong C (2006). Workplace Empowerment, Work Engagement and Organizational Commitment of New Graduate Nurses. Nursing Leadership-Academy of Canadian Executive Nurses 19 (3):4. |
|
|
Deery M (2008). Talent management, work-life balance and retention strategies. International Journal of Contemporary Hospitality Management 20(7):23-28. |
|
|
Duffield C, Roche M, O'Brien-Pallas L, Catling-Paull C, King M (2009). Staff Satisfaction and Retention and the Role of the Nursing Unit Manager. Collegian 16:11-17. |
|
|
Fang Y (2017). Burnout and work-family conflict among nurses during the preparation for reevaluation of a Grade A tertiary hospital in China. Chinese Nursing Research 4(1):51-55. |
|
|
Finn C (2001). Autonomy: An important component for nurses' job satisfaction. International Journal of Nursing Studies 38(3):349-357. |
|
|
Greenhaus J, Beutell N (1985).Sources of conflict between work and family roles. Academy of Management Review 10:76-88. |
|
|
Harrington B, Ladge J (2009). Present dynamic and future direction for organizational. Organizational Dynamics 338(2):148-157. |
|
|
Karimi Q, Jomehri F, Asadzade H, Sohrabi F (2012). Consequences of Conflict between Work and Family among Iranian Female Teachers. Journal of Basic and Applied Scientific Research 2(2):1869-1875. |
|
|
Khamisa N, Oldenburg B, Llic D (2015). Work related stress, burnout, job satisfaction and general health of nurses in South Africa. International Journal of Environmental Research and Public Health 12(1):652-666 |
|
|
Lembrechts L, Dekocker V, Zanoni P, Pulignano V (2015). A study of the determinants of work-to family conflict among hospital nurses in Belgium. Journal of Nursing Management 23(7):898-909. |
|
|
Mansour S, Tremblay D (2016). Workload, generic and work-family specific social supports and job stress: mediating roles of work-family and family-work conflict. International Journal of Contemporary Hospitality Management. ISSN: 0959-6119 |
|
|
Makola L, Mashegoane S, Dubusho (2015). Work-family and Family-work conflict among African nurses caring for patient with AIDS. Journal of the Democratic Nursing Organization of South-Africa 38(1):1436. |
|
|
Michel S, Kotrba M, Mitchelson K, Clark A, Baltes B (2011). Antecedents of work-family conflict: a meta-analytic review. Journal of Organizational Behavior 32(5):689-725. |
|
|
Morgeson FP, Humphery SE (2006). The work design questionnaire (WDQ): Developing and validating a comprehensive measure for assessing job design and the nature of work. Journal of Applied Psychology 91(6):1321-1339. |
|
|
Mordi C, Mmieh F, Ojo S (2013). An exploratory study of manager's perspective of work-life balance in Nigeria: A case analysis of the Nigerian banking sector. Thunderbird International Business Review, 55(1):56-75. |
|
|
Ogbogu C (2013). Work-Family role conflict among academic women in Nigerian Public Universities. WEI International Academic Conference Proceedings. |
|
|
Ozor T, Mgbenkemdi E, Omeje O (2016). Work-Family Conflict as Correlate of Burnout Among Married Female Nurses. Gojamss Journal 12. |
|
|
Polit Beck (2010). Essentials of Nursing Research: Appraising evidence for Nursing Practice. USA: Lippincott-Raven Publishers (seventh edition). |
|
|
Sabil F, Abu H, Ali J, Lizzan N (2016). Identifying Work-Family Conflict Among Nurses: A Qualitative Study. The European Proceedings of Social/Behavioural Sciences. |
|
|
Ugoani JN (2013). Emotional intelligence and balancing WFC among dual career parents in Nigeria. Management and Administrative Science 2(5):575-582. |
|
|
Yamane T (1973). Statistics and introductory analysis. New York: Harpers & Roy. |
|
|
Zito M, Colombo L, Mura G (2013) Job demand and work-family conflict in a health care staff: The role of work shifts. Giornale Italiano di Medicina de lLavoroed Ergonomia Journal 35(3):168-175. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


