Full Length Research Paper

ABSTRACT
Antenatal care (ANC) has been recommended as a service that can reduce both maternal and newborn mortalities. However, even in areas recording high ANC attendance, there are unevenly high levels of maternal and new born mortalities. Evidence of a weak relationship between ANC use and maternal and newborn survival has motivated recent calls to focus on content and quality of care provided rather than mere ANC attendance. This was a descriptive cross sectional study which was designed to evaluate the quality of antenatal care services in two health facilities in Lusaka and two in Mumbwa districts of Zambia. The health facilities were selected purposively based on poor maternal outcomes such as high maternal mortality ratio. Women attending antenatal clinics were selected using simple random sampling. Data was collected using a client exist interview schedule designed by World Health Organization for assessing quality of antenatal care. Data was analyzed using Statistical Package for Social Scientist (SPSS) version 24.0. The study revealed a lot of variations in the care provided at the four sites. None of the women had all the blood tests for haemoglobin, grouping and X-match, HIV and syphilis conducted from three out of the four health facilities, while at the fourth, only 30% of women had all the blood tests conducted. Furthermore, less than 20% of women had a full head to toe examination. While less than 10% of women from each of the facility reported that the health providers met the requirements for provision of privacy. Despite not meeting the minimum standards of care, only less than 5% of women categorized the care as poor. All the four health facilities recorded low quality of care on all domains of antenatal care. Therefore, if antenatal care has to achieve its intended purpose of reducing adverse maternal and new born outcomes, then quality of care delivered during pregnancy should be the focus as opposed mere attendance.
Key words: Quality, antenatal care services, evaluation.
INTRODUCTION
Every day, approximately 800 women die from preventable causes related to pregnancy and childbirth (WHO, 2017). To this effect, Antenatal Care (ANC) has been recommended as one means to reduce both maternal and newborn mortalities (WHO, 2005). ANC services enable early identification of pregnancy related risks and complications and ensure access to services including health education, vaccinations, diagnostic tests and treatments (Gross et al., 2011). Additionally, WHO (2016) states that antenatal care does not only serve as a platform for health promotion, prevention, screening, and diagnosis of diseases but also as an opportunity to provide pregnant women with the social and psychological support necessary for healthy motherhood. However, even in areas recording high ANC attendance, there are unevenly high levels of maternal and new born mortalities (Kyei et al., 2012). For example in Zambia, more than 9 in 10 (96%) mothers received antenatal care from a skilled provider for their most recent pregnancy, while the maternal mortality ratio is still standing at 398/100,000, while neonatal and infant mortality stands at 24 deaths/1,000 and 45/1,000, respectively.
Evidence of a weak relationship between ANC use and maternal and newborn survival has motivated recent calls to focus on content and quality of care provided rather than mere ANC attendance (WHO, 2015). Similarly, Kyei et al. (2012) and Nwaeze et al. (2013) asserted the need to focus on resources and strategies to be tailored towards improving the quality of care provided in order to optimize the results other than focusing on mere ANC attendance. This is in view of the evidence that effectiveness of ANC relies on the quality of care provided during each visit (Ejigu et al., 2013).
Quality health care delivered during pregnancy and childbirth has been shown to prevent most of the adverse outcomes of pregnancy, and antenatal care provides an important platform to achieve a reduction in pregnancy-related mortality and morbidity (Tunçalp et al., 2017). The essence of ANC therefore is to prepare women for birth and parenthood and prevent problems for pregnant women, mothers and babies through early detection, alleviation and/or management of health problems that affect mothers and babies during pregnancy (Lincetto et al., 2010).
In addition to focusing on quality of ANC services with regard to structures, processes and outcomes, it should be realized that pregnant women have the rights to participate in decisions involving their well-being and what may or may not be done to their bodies (Wheatley et al., 2008; Sword et al., 2012; Shabila et al., 2014). Understanding women’s perspectives of antenatal care services is particularly important for enhancing effectiveness of healthcare delivery as it ensures that strategies for improving care are inclusive of the end user views.
Furthermore, Wheatley et al. (2008) and Sword et al. (2012) assert that understanding women’s perspectives and experiences of ANC can result in provision of ANC services which are responsive to women’s needs and expectations.
Despite the documented evidence of the significance of quality of ANC services in comparison to mere attendance, a numbers of studies conducted in African countries have reported less desirable quality of ANC services. For example, Fagbamigbe and Idemudia (2015) in a study conducted to assess quality of ANC services in Nigeria found that less than 5% of ANC users in Nigeria received desirable quality of ANC services with about one tenth receiving minimum acceptable quality. In the same study, it was revealed that although most attendees made four visits, it was very striking that about 1% did not receive any of the ten ANC components considered in that study. This study revealed further that the commonest component of ANC offered in Nigeria are measurement of blood pressure and distribution of iron supplement as they were offered to nearly all the attendees while other important components of ANC such as health education on PMTCT, IPT and urine testing were reported to be low.
Similarly, a study conducted in Zambia by Kyei et al. (2012), revealed inadequacies with regard to services provided during ANC. For example, while folate/iron supplementation, tetanus vaccination and IPT of malaria were provided by the vast majority of ANC facilities, detection and prevention of mother-to-child transmission of HIV was only available at a third of ANC facilities. Most screening tests were not commonly available: only 16% of ANC facilities provided haemoglobin testing which is helpful in diagnosing anemia, and only half provided syphilis testing. Urine protein testing, which is important for detecting hypertensive complications of pregnancy such as pre-eclampsia, was performed by less than a quarter of ANC facilities. With this background, the present study sought to evaluate the quality of antenatal care services from the pregnant women’s perspectives in selected healthcare centres of Mumbwa (mainly rural) and Lusaka (mainly urban) districts of Zambia.
MATERIALS AND METHODS
A descriptive cross sectional multi-site study design was used to evaluate the quality of antenatal, intranatal and postnatal care services in two health centres in Lusaka district and two 1st Level hospitals in Mumbwa district of Zambia. The Lusaka based sites constituted the urban setting, while the Mumbwa district sites constituted rural sites. The study involved evaluating the structures, processes, outcomes and provider’s perspectives of services in the antepartum, intrapartum and postpartum areas in the selected heath facilities. However, the focus of this article is the quality of antenatal care services in the selected health centres, while other aspects of the study have been reported elsewhere.
The health facilities which were included were purposively selected based on poor maternal outcomes such as high MMR. On the other hand, pregnant women were selected using simple random sampling. All women within the reproductive age groups of 15 to 49 years who were seeking antenatal care services at the selected health centres during the study period constituted the study population.
Data were collected using a client exist interview schedule designed by World Health Organization for assessing quality of antenatal care. The tool obtained data under three main categories of demographic characteristics, quality and content of services available at the ANC clinic and client’s perceived quality of ANC services. Data was then entered and analyzed using Statistical Package for Social Scientist (SPSS) version 24.0. Descriptive statistics were computed for the demographic data to understand the demographic characteristics of the study participants. Furthermore, attributes of quality were computed as percentages in order to compare with the WHO recommended minimum quality of care which is set at 80%.
RESULTS
A total of 172 pregnant women attending antenatal care were interviewed; 124 from the two urban health centres and 44 from the two rural health centres. The demographic characteristics are shown in Table 1. The WHO recommended minimum package for ANC includes history obtained from the pregnant woman, physical examination, observations and laboratory tests, drugs and immunizations provided. Others are information on the importance of ANC, nutrition during pregnancy, birth preparedness, danger signs in pregnancy, prevention of HIV in general and prevention of mother to child transmission (PMTCT) in particular (USAID/Population Council, 2006). This study therefore evaluated the quality of ANC and perceived satisfaction with care received at the four health facilities against each component of the WHO ANC package. Quality of care was evaluated with regard to the percentage of women receiving each component of care. Results are presented in Tables 2 to 6.



DISCUSSION
Quality health care delivered during pregnancy and childbirth has been shown to prevent most of the adverse outcomes of pregnancy, and that antenatal care provides an important platform to achieve a reduction in pregnancy-related mortality and morbidity (Tancalp et al., 2017). However, it has been argued that mere ANC attendance does not always accrue to reduction in pregnancy related mortality and morbidity as it has been observed that even in areas recording high ANC attendance, there are unevenly high levels of maternal and new born mortalities (Kyei et al., 2012). This discrepancy has heightened the call to focus on quality and not simply the quantity of ANC.
In Zambia, a typical ANC visit should involve history taking, physical examination, conducting of essential tests including haemoglobin, HIV, syphilis, counselling on risk factors, danger signs and how to handle them, counselling on birth preparation and prevention of Mother to Child Transmission (PMTCT). Other activities include administration of tetanus toxoid vaccine, supply of Fansidar (Sulfadoxine Pyrimethamine) and other essential supplements and prophylaxis medication. Despite this prescribed standard package of care, there were a lot of variations in the care provided at the four sites where the study was undertaken. According to Osungbade et al. (2008), history of current pregnancy is essential at any visit as it provides an opportunity to obtain information that may influence maternal and child health outcomes. However, this was not the case in the current study, for example, the two urban health facilities, less than half of the women had all the different components of history taken (past medical, surgical, family history, and present obstetrics history). While for the two rural health centres, more than 50% of the women had all the different components of the history taken, with the most frequently asked question being on past medical history (Table 2).
World Health Organization advocates that only examinations and tests serving an immediate purpose and proven to be beneficial should be performed during antenatal visits (WHO, 2001). These examinations should include, at a minimum, measurement of blood pressure, testing of urine for bacteriuria and proteinuria, and blood tests to detect syphilis and severe anaemia (WHO, 2003).
With regard to the different types of observations carried out, the present findings revealed that all health facilities recorded at least 50% of all women having their blood pressure, weight and height measured (Table 2). This is against the recommendation by WHO that all women should have their blood pressure checked, and urine and blood tested. Considering that not all the women had their basic observations done, taking for example blood pressure, this implies that those with elevated blood pressure and at risk of pre eclampsia were missed resulting into potential for increased morbidity and mortality.
While it is recommended that all pregnant women should have a complete head to toe examination at all visits for early detection of conditions such as anaemia, renal dysfunction, hypertensive disorders and assessment for fatal growth and viability, the present study showed that less than 20% of women accessing ANC at the four health centres had a full head to toe examination (Table 2). On the other hand, blood laboratory test such as haemoglobin, grouping and X-match, HIV and syphilis were not conducted on all women.
The present findings revealed that none of the women had all the tests conducted from three out of the 4 centres assessed, while the fourth centre, only 30% of women interviewed had all the blood tests done. Other tests such as urine protein testing, which is important for detecting complications for hypertensive disorders such as pre-eclampsia were similarly not performed on all women. This finding is similar to the findings by Kyei et al. (2012) in a similar national wide study conducted five years before the current study in which it was indicated that urine testing was performed by less than a quarter of ANC facilities assessed. Findings of this study therefore are an indication that not much changes have occurred with regard to quality of ANC in the last five years in the country.
Provision of drugs and other immunization are an important package of ANC. In Zambia, it is recommended that all pregnant women should receive preventive medicines to prevent certain conditions. These are Tetanus Toxoid immunization to prevent tetanus, iron/folate supplementation to prevent iron deficiency anaemia thus contributing to the prevention of severe anaemia and complications like pre-term birth, congenital anormalies and intrauterine growth restriction. Others are intermittent preventive treatment (IPT) with Fansidar and albendazole and mebendazole for treatment for hookworm infestation. Despite the significance of these preventive medicines, there were variations in the provision of these essential drugs. For example, while in one urban centre more than 77% of women received all the preventive medicines, in the other urban centre only 30% received all. This finding agrees with the findings reported in a study conducted in Namibia and Kenya by Do et al. (2017) where despite the iron and folic supplements being available in the facilitates which were assessed in Kenya, they were provided to only a few.
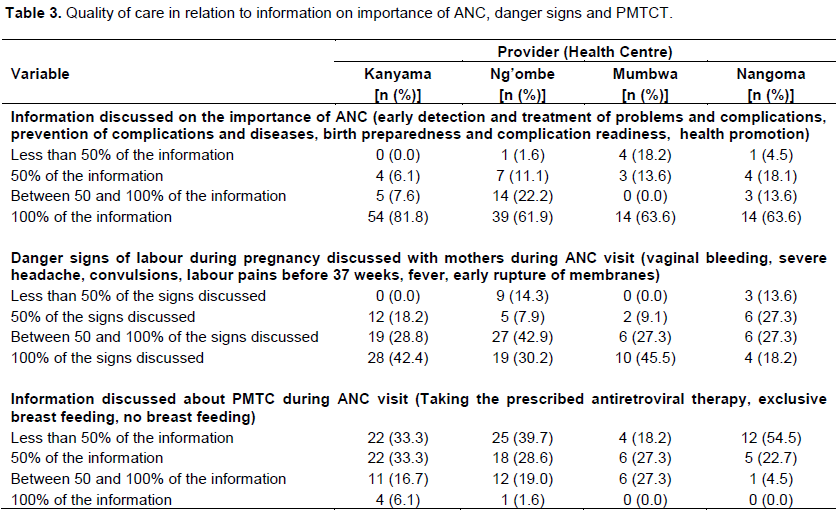
Pregnant women need to be taught about the importance of ANC, danger signs during pregnancy and PMTCT (Table 3). Regarding the importance of ANC, the information should include early detection and treatment of problems and complications, prevention of complications and diseases, while danger signs during pregnancy should include vaginal bleeding, severe headache, convulsions, labour pains before 37 weeks, fever, and early rupture of membranes. On the other hand, information on PMTCT should include taking the prescribed antiretroviral therapy, exclusive breast feeding and not breast feeding at all if someone makes such a choice.
Findings of the current study revealed that at least 60% of all pregnant women across the four facilities had received all information on the importance of ANC, meanwhile only less that 50% of women interviewed had received all information pertaining to danger signs in pregnancy, with one rural health centre recording only 18% of women receiving all the information. This situation can have negative effect if those who are missed happen to experience some danger signs which they may not have information about and it could result in delay in seeking care. The findings of the present study are similar to those reported from Kenya by the Kenya National Bureau of Statistics (2010) where less than half of the pregnant women reported to have been informed of signs of pregnancy complications. PMTCT was the lowest in terms of information given. None of the women interviewed from the two rural facilities had all the information on PMTCT, while the two urban facilities record less than 10% of women receiving all information on PMTCT. Meanwhile information on HIV is highly desired by pregnant women as reported in a study conducted by Katowa-Mukwato et al. (2017), that one of the health information need of pregnant teenagers was knowing and dealing with HIV and clarifying myths and misconception of both pregnancy and HIV and a desire to have nurses teach pregnant teenagers separately from older women especially on issues of PMTCT.
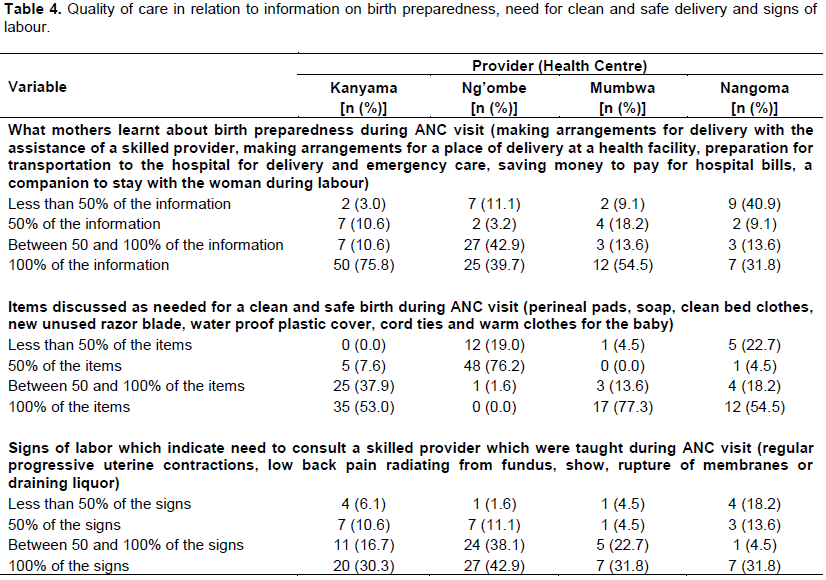
Findings of the current study reviewed a lot of variations in relation to information on birth preparedness, need for clean and safe delivery and signs of labour (Table 4). On information regarding birth preparedness, which include making arrangements for delivery with the assistance of a skilled provider, arrangements for a place of delivery at a health facility, preparation for transportation to the hospital for delivery and emergency care, saving money to pay for hospital bills, and having a companion to stay with the woman during labour. One urban facility recorded 75.8% of women receiving all the information while the other one only 39.7% received all the information. Similarly, 54.5% of the women from one rural facility indicated having received all information on birth preparedness compared to only 31.8 from the other rural facility who received all the information. Regarding items discussed as needed for clean and safe delivery, three out of the four facilities included in the study had more than 50% of women stating that they received all the information to this effect. The study reviewed disappointing results in that less than 50% of women from the four health facilities had all the information on signs of labour taught to them. These results agree with those of Kanyangarara et al. (2017) in a study of quality of ANC services across sub-Saharan Africa, who reported low coverage of barely all components of ANC components including information on signs of labour. Similar findings have been reported by Saad-Haddad et al. (2016) and Victora et al. (2015).
The scenario of inadequate information provision by midwives spans the whole continuum of maternity care from ANC, to labour and delivery and postnatal as reported by Muleya et al. (2018), Bhavnani and Newburn (2010) and Almeida and Silva (2008). These studies reported poor information giving by care providers including midwives despite all women irrespective of parity desiring information about their health, the health of their infants, danger signs, and postnatal checkup and how to behave as mothers. The inadequate information created anxieties among mothers and constituted a negative experience of care.
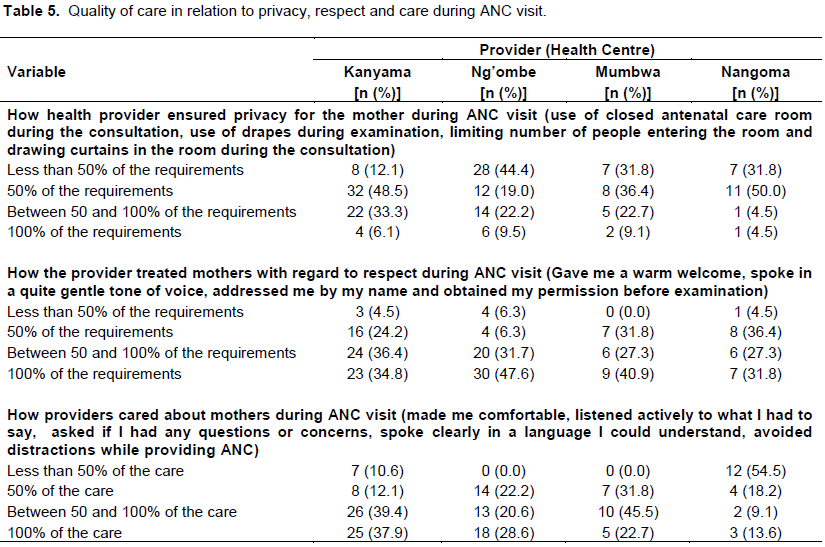
The final category of quality assessed was on respectful care, that is provision of privacy, respect and general concern and care during ANC (Table 5). This category was the poorly scored. For example, under privacy less than 10% of women from each of the facility reported that the health providers meet these requirements; closed antenatal care room during the consultation, use of drapes during examination, limiting number of people entering the room, and drawing curtains in the room during the consultation. With regard to respect that should be given including a warm welcome, speaking in a quite gentle tone of voice, addressed client by name, obtaining permission before examination, and less than 50% of women from all the health centres reported to have been accorded all the attributes of respect. This could impact negatively on quality of ANC and level of satisfaction with care. Do et al. (2017) reported that the client’s ability to discuss concerns with providers, provider’s explanation of problems and treatment, quality of the examination and women’s ability to share information is related to the level of privacy and associated with satisfaction with care.
Regarding provision of comfort, active listening, asking, allowing women to ask questions or clarifying concerns, speaking in a language that a lay person can understand and avoiding distractions while providing care, less than 50% of the women from all the four health facilities reported their care meeting all the desirable attributes. Despite not meeting the minimum standards of care, when asked about the overall satisfaction about care, surprisingly only less than 5% of women categorised the care as poor with most women generally reporting satisfactory care. This finding is contrary to that reported by Do et al. (2017) who reported low levels of satisfaction with ANC services in public facilities both in Kenya and Namibia.
CONCLUSION
All the four health facilities recorded low quality of care on all domains of Antenatal Care as outlined by WHO: History obtained during ANC, observations of vital signs, antenatal examination, laboratory blood investigations, provision of drugs and immunization, and education on nutrition, prevention of HIV, identifying danger signs and provision of respectful care. Therefore, if antenatal care has to achieve its intended purpose of reducing adverse maternal and new born outcomes, then quality of care delivered during pregnancy should be the focus as opposed mere attendance.
LIMITATION
The study reports quality of ANC from the pregnant mothers’ perspectives. Although this is one of the parameters for evaluating quality of ANC services according to World Health Organization, observation of care provided would have been conducted.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the financial support provided by the Norwegian Agency for Development (NORAD) through the NORHED QZA-0848 QZA-MW-13/00032 Grant.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Almeida MS, Silva IA (2008). Women's needs in immediate puerperium in a public maternity in Salvador, Bahia, Brazil. Revista da Escola de Enfermagem da USP 42(2):347-354. |
|
|
Bhavnani V, Newburn M (2010). Left to your own devices: The Postnatal experiences of 1260 first time mothers. The National Childbirth Trust: London. |
|
|
Do M, Wang W, Hembling J, Ametepi P (2017). Quality of antenatal care and client satisfaction in Kenya and Namibia. International Journal for Quality in Health Care 29(2):183-193. |
|
|
Ejigu T, Woldie M, Kifle Y (2013). Quality of antenatal care services at public facilities of Bahir-Dar special zone, Northern Ethiopia. Health Service Research 13:443: |
|
|
Fagbamigbe AF, Idemudia FS (2015). Assessment of quality of antenatal care services in Nigeria: evidence from a population-based survey. Reproductive Health 12(1):88 |
|
|
Gross K, Schellenberg JA, Kessy F, Pfeiffer C, Obrist B (2011). Antenatal care in practice: an exploratory study in antenatal care clinics in the Kilombero Valley, South-Eastern Tanzania. BMC Pregnancy and Childbirth 11(1):36 |
|
|
Kanyangara M, Munos KM, Walker N (2017). Quality of antenatal care service provision in health facilities across Sub-Saharan Africa: Evidence from Nationally representative health facility assessment. Journal of Global Health 7(2). |
|
|
Katowa-Mukwato P, Maimbolwa M, Mwape L, Muleya CM (2017). Experiences, needs and coping strategies of pregnant and parenting teenagers. Journal of Research in Nursing and Midwifery 6(4):056-067. DOI: http:/dx.doi.org/10.14303/JRNM.2017.110 |
|
|
Kenya National Bureau of Statistics (KNBS) (2010). ICF Macro. Kenya Demographic and Health Survey 2008-09. Calverton, MD: KNBS and ICF Macro, 2010. |
|
|
Kyei NNA, Chansa C, Gabrysch S (2012). Quality of antenatal care in Zambia: A national assessment. BMC Pregnancy and Childbirth 12(1):151. |
|
|
Lincetto O, Mothebesoane-anoh S, Gomez P, Munjanja S (2010). Antenatal care: Opportunities for Africa's Newborns. New York: World Health Organization. |
|
|
Muleya CM, Mwape L, Katowa-Mukwato P, Maimbolwa M (2018). Postnatal care within six hours following delivery at two selected general hospitals of Zambia-mothers' experiences. Open Journal of Nursing 8:355-371. |
|
|
Nwaeze IL, Enabor OO, Oluwasola TA, Aimakhu CO (2013). Perception and satisfaction with quality of antenatal care services among pregnant women at the university college hospital, Ibadan, Nigeria. Annals of Ibadan postgraduate medicine 11(1):22-28. |
|
|
Osungbade K, Oginni S, Olumide A (2008). Content of antenatal care services in secondary health care facilities in Nigeria: implication for quality of maternal health care. International Journal for Quality in Health Care 20(5):346-351. |
|
|
Saad-Haddad G, Dejong J, Clara M, Méndez R, Vaz L, Amouzou A (2016). Patterns and determinants of antenatal care utilization: Analysis of national survey data in seven countdown countries. Journal of Global Health 6(1). |
|
|
Shabila NP, Ahmed HM, Yasin MY (2014). Women's views and experiences of antenatal care in Iraq: A Q methodology study. BMC Pregnancy and Childbirth 14(1):43. |
|
|
Sword W, Heaman MI, Brooks S, Tough S, Janssen PA, Young D, Kingston D, Helewa ME, Akhtar-Danesh N, Hutton E (2012). Women's and care providers' perspectives of quality prenatal care: a qualitative descriptive study. BMC Pregnancy Childbirth 12(1):29. |
|
|
Tunçalp Ö, Pena-Rosas JP, Lawrie T (2017). WHO recommendations on antenatal care for a positive pregnancy experience-going beyond survival. British Journal of Obstetrics and Gynaecology 124: 860-862. |
|
|
USAID/Population Council (2006). Acceptability and sustainability of the WHO focused antenatal care package in Kenya, Washington DC: USAID. |
|
|
Victora CG, Requejo JH, Barros AJD, Berman P, Bhutta Z, Boerma T (2015). Countdown to 2015: A decade of tracking progress for maternal, new born, and child survival. The 2015 Report. |
|
|
Wheatley RR, Kelley MA, Peacock N, Delgado J (2008). Women's narratives on quality in prenatal care: A multicultural perspective. Qualitative Health Research 18(11):1586-1598. |
|
|
World Health Organization (WHO) (2005). The World health report: make every mother and child count. Geneva: World Health Organization: |
|
|
World Health Organization (WHO) (2016). WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: World Health Organization. |
|
|
World Health Organization (WHO) (2017). Maternal mortality: Global Health Observatory (GHO) data. |
|
|
World Health Organization (2001). WHO Antenatal Care Randomized Trial: Manual for the implementation of the new model. WHO/RHR/01.30. Geneva: WHO. |
|
|
World Health Organization (2003). Antenatal care in developing countries: Promises, achievements and missed opportunities. Geneva: Switzerland. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


