Full Length Research Paper

ABSTRACT
Men are the major decision makers in the home; thus, this study was designed to assess the knowledge and practice of married men towards safe motherhood in Ibadan North Local Government Area, Oyo State, Nigeria. A descriptive cross-sectional study was adopted using a multi-stage and proportionate sampling technique to recruit three hundred and ten married men. A semi-structured questionnaire used to solicit information on socio-demographic characteristics, knowledge and practice of safe motherhood among respondents. Knowledge were measured on 35-point and knowledge scores of ≤11, 12-23, ≥24 were rated poor, fair and good respectively. Descriptive statistics and Chi-square test were conducted at 5% level of significance. Respondents’ age was 43.7±7.9 years, 85.5% were Yoruba and 54.5% were Muslims, 47.1% of the respondents had secondary education. A good number of the respondents (64.2%) had safe motherhood awareness but the knowledge of safe motherhood was poor (74.8%). About one-third (33.1%) understood safe motherhood as taking care of women throughout pregnancy. The overall mean knowledge score was 8.97±3.48. Level of education and occupation were statistically significant with respondents' knowledge of safe motherhood. There is need to enlighten married men about safe motherhood and involvement in maternal health.
Key words: Married men, safe motherhood, maternal health, safe motherhood knowledge, practice.
INTRODUCTION
The lifetime risk of maternal mortality of women in sub- Saharan Africa is 1 in 39 live births, which is the highest when compared to other world regions (Tilahun et al., 2013). The World Health Organization (WHO) estimated in 2012 that 287,000 maternal deaths occurred in 2010; sub-Sahara Africa (56%) and Southern Asia (29%) accounted for the global burden of maternal deaths (World Health Organization, UNFPA and World Bank, 2012). Most developed countries have made considerable progress in addressing maternal mortality, but it appears that countries with high maternal mortality burdens like Nigeria have made little progress in improving maternal health outcomes despite emphasis by the Millennium Development Goals (MDGs) (Okereke et al., 2013). Nigeria accounts for 1 in 6 maternal deaths globally. Approximately 50,000 Nigerian women die each year from largely preventable pregnancy-related complications (Erim et al., 2012). Certain avoidable factors (biomedical, reproductive, health service factors, socioeconomic and cultural factors) increase the risks of severe complications or maternal death (Somé et al., 2013).
A majority of the deaths related to pregnancy and childbirth can be prevented if the women receive adequate and timely medical care at the crucial moments, evidence suggests that providing expectant mothers with adequate maternal care, birth supervision by skilled attendants, and access to emergency obstetric care in pregnancy and delivery can save lives (Oyeyemi and Wynn, 2012). He further stated that complications that can potentially lead to death exist in about 9-15% of pregnancies, 75% of maternal deaths are as a result of direct causes from severe haemorrhage (bleeding), maternal sepsis (infection), obstructed labour, high blood pressure with fits in pregnancy (eclampsia) and unsafe abortion (Oyeyemi and Wynn, 2012).
Most cultures, especially in Africa, regard all issues related to pregnancy or childbirth as a female domain; therefore, men are often not expected to be involved in any health seeking behaviour during pregnancy (Kwambai et al., 2013). Safe motherhood has been conceptualized as a means of ensuring women's accessibility to needed care through antenatal programme in order to facilitate their safety and optimal health throughout pregnancy and childbirth (Igbokwe and Adama, 2011). Safe motherhood is a means of saving the lives of women and improving the health of millions of others (Jatau, 2014).
In a study conducted in rural Tanzania, involvement men in antenatal care service are identified as important in maternal health. Maternal mortality has decreased worldwide in the last ten years; however, in the Sub-Saharan countries it is still high. The World Health Organization (WHO) estimates that, currently, 287,000 women a year die of preventable complications related to pregnancy and childbirth; the majority of these (99%) occur in developing countries and, out of those, 51% occur in the Sub-Saharan region (August et al., 2015).
Safe motherhood is aimed at preventing maternal and prenatal mortality and morbidity. It also enhances the quality and safety of women's life through the adaptation of combination of health and non-health strategies (Jatau, 2014). The importance of safe motherhood to the overall development of a country or a nation cannot be over-emphasized and it has to be acknowledged at the highest levels. Therefore, this study is aimed at assessing the knowledge, attitude and perception of married men on issues related to safe motherhood and by implication, this will help in understanding men’s disposition and serve as a guide in designing targeted programs and in the long run contributing to the reduction of the country's maternal mortality and the realization of MDGs-5. The broad objective of this study is to investigate the knowledge, attitude and perception of married men towards Safe Motherhood Initiatives in Ibadan North Local Government Area of Oyo state, Nigeria.
MATERIALS AND METHODS
The study was a cross-sectional descriptive study. The study accessed the knowledge, attitude and perception of married men towards safe motherhood. The study was carried out in Ibadan North Local Government Area, Ibadan North Local Government is situated in Ibadan metropolis which was carved out of the defunct Ibadan Municipal Government by the Federal Military Government of Nigeria on 27th September 1991. The local government is bounded by Akinyele Local Government in the North, in the east, it is bounded by Ibadan North East and Lagelu Local Government, it’s bounded by Ido Local Government, Ibadan South West and Ibadan South-East Local Government in the West.
Three hundred and ten married men using a five-stage multi-stage sampling technique to select respondents for the study. A semi-structured interviewer administered questionnaire which comprised open and closed ended questions was used to collect data from respondents. Four research assistants were recruited for the study and were trained a day prior to commencement of data collection to ensure that they have good understanding of the instrument. They were trained on the objectives and importance of the study, sampling process, how to get respondent's informed consent, detailed review of the questions to ensure familiarity and interviewing techniques.
Instrument for data collection
A semi-structured interviewer administered questionnaire which comprised open and closed ended questions was used to collect data from respondents. Related information from literatures guided the development of the research instrument.
Procedure for data collection
Four research assistants were recruited for the study since interviewer administered questionnaire was used for the study. They were trained a day prior to commencement of data collection to ensure that they have good understanding of the instrument. They were trained on the objectives and importance of the study, sampling process, how to get respondent's informed consent, detailed review of the questions to ensure familiarity and interviewing techniques. Data collection commenced on 7th September 2015 and ended 6th October; it lasted for approximately 4 weeks. Approval to interview respondents was gotten from the head of each community after explaining to them the purpose and benefits of the research. Thereafter informed consent was sought from the participants before being recruited into the study and the questionnaires were administered to them in seclusion to give room for privacy. Respondents were selected from every third house, in houses where there were more than one household, balloting was done to select a household where the respondent was picked.
Ethical consideration
Ethical approval was obtained from the ethical committee of Oyo State Ministry of Health Ethical Review Committee prior to the commencement of the study. At the community level, community leaders granted permission to conduct the study. The respondents gave verbal consent prior to being interviewed. Respondents were assured of confidentiality of information as there was no form of identifier on the questionnaire.
Data management and analysis
All questionnaires were reviewed after completion for accuracy and serial number were written on each for easy identification and recall. Coding guide was then developed to facilitate the entry of the responses into the computer. The responses were then entered into the computer after coding using the SPSS software. Data analysis were carried out using descriptive statistics and inferential at 5.0% level of significant.
RESULTS
The ages of respondent ranged from 25 to 64 years with a mean age of 43.7±7.9 years. Almost half (45.8%) fell between the 35 to 44 years age group. More than half of the respondents (54.5%) were Muslims and majority of the respondents were Yoruba (85.8%). The highest educational qualification of almost half of the respondents (47.1%) was secondary education, (38.1%) acquired tertiary education, 11.9% completed primary education while 2.9% did not acquire any formal education. A greater percentage of the respondents (43.9%) have spent between 10 to 19 years in their marriage (Table 1). On respondents occupation, (35.2%) were traders, (29.3%) were civil servants followed by artisans (23.9%). More than half of the respondents (51.6%) make a joint decision with their wives about where they seek maternity care while (38.4%) of the respondents make the sole decision about where the wife seeks maternity care, (8.7%) of the respondents wives decides where she wants to deliver and family decides for the remaining (1.3%). Majority of the respondents (87.4%) has just one wife while (12.6%) are polygamous with (89.7%) having two wives and 10.3% married to three wives.

Knowledge about safe motherhood
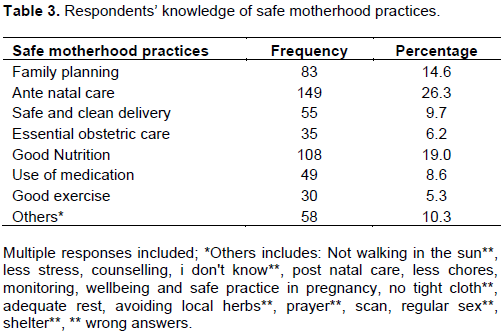
Majority of the respondents 199(64.2%) have heard about safe motherhood. According to the respondents, safe motherhood was understood as taking care of a pregnant woman throughout pregnancy by 33.1% of respondents, going to the hospital for antenatal checkups (17.6%), less stress for a woman (17.1%), good nutrition (11.0%), less chores (8.8%). Other responses (12.4%) include taking prescribed drugs, adequate rest after delivery, exercise, lot of sex, no violence, exclusive breastfeeding, safe delivery, financial assistance, family planning (Table 2). The two highest source of information of the respondents are Media (37.7%), Hospital (21.9%) among others. Concerning safe motherhood practices, (26.3%) mentioned Ante natal care, 19% mentioned nutrition, 4.6% mentioned family planning (Table 3).

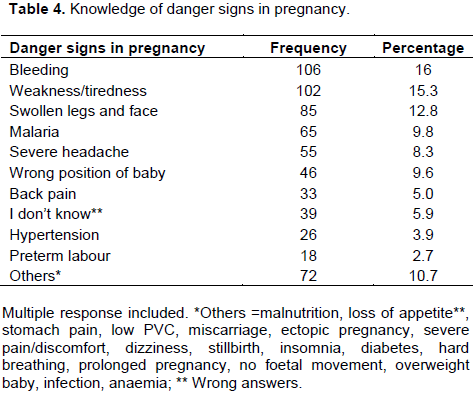
Majority of the respondents (91.0%) were sure that their wives take their medications regularly during pregnancy and most of the respondents' wife (96.8%) seeks care in the hospital during pregnancy. Majority (86.1%) of the respondents reported correctly that problems related to pregnancy and childbirth can endanger the life of a woman. On the danger signs in pregnancy, 16.0% of respondents mentioned bleeding, 15.3% said weakness and tiredness, 12.8% mentioned swollen legs and faces, 9.8% mentioned malaria, other responses are represented on the Table 4 while about one-third (61.9%) of respondents affirmed that a woman can die from any of the problems.
On danger signs during labour, 21.9% reported severe bleeding, 10.6% mentioned severe headache, 9.9% said prolonged labour while 16.1% admitted they do not know the danger signs in labour, others are represented on Table 5. Test of associations indicated that there is relationship between respondent's level of education (c2=13.35; p-value=0.04) and occupation (c2=15.4; p-value=0.000) and knowledge about safe motherhood.

Knowledge of safe motherhood was calculated for each respondent using a 35-point knowledge scale assessing understanding of safe motherhood, knowledge of safe motherhood practices, and knowledge of danger signs in pregnancy and labour, knowledge about whether a woman can die from the pregnancy and labour related dangers. Each correct answer was scored 1 and incorrect answers were scored 0, then each respondent's score was summed up to give the total knowledge score for each respondent. The scores were categorised into poor, fair and good knowledge. A score above 24 was categorised as good knowledge score, while a score from 12-23 was categorised as fair and scores below 12 was categorised as poor. Most of the men (74.8%) had poor knowledge of safe motherhood (Table 6).

DISCUSSION
The ages of respondents ranged from 25-64 years, greater number of the study participants were within the range of 35-44 years, those within the 45-54 age bracket were the next most numerous. The mean age of 43.6±7.9 found in this study was observed to slightly vary from an earlier study carried out in Northern Uganda conducted by (Jatau, 2014). The implication of this mean age is that majority of the men are still in their reproductive ages and they are agile enough to participate in safe motherhood. It is therefore necessary to enlighten men of this age group on the importance of participation in safe motherhood.
More than three quarter of the respondents were from the Yoruba ethnic group as revealed from the study, this is expected since the study is carried out in Ibadan North, a local government in the South-western part of Nigeria. The proportion of the respondents who practised Islam is higher compared to those who practiced Christianity and traditional religion which was similar to a research conducted in Osogbo (Adelekan et al., 2014) where more than three quarter of the respondents were Muslims. The educational status of men in the community can be considered to be less than average since less than half of them had at least secondary education. Respondent's with secondary education were the highest followed by tertiary education, this can be attributed to the fact that the study was carried out in a community setting where all categories of people can be found. A higher percentage of the respondents were self employed, this is expected since most people in the local government are in the private sector.
Knowledge of the respondents about safe motherhood
Safe motherhood means different things to different people, respondents understood safe motherhood as different things; taking care of pregnant woman throughout pregnancy, going to the hospital for antenatal check-up, less stress and chores during pregnancy, good nutrition. The finding from this study shows that there is poor knowledge of safe motherhood initiative/ practices while some of the respondents understood it as taking prescribed drugs, exercise, adequate rest after delivery and lot of sex. Few of the respondents recognised antenatal care as a safe motherhood practice, fewer said nutrition while even fewer recognized family planning, safe and clean delivery and essential obstetric care as safe motherhood practices. Majority of the respondents agreed that problems related to pregnancy and childbirth can endanger the life of a woman. Despite the high level of awareness, only few of the respondents could identify the danger sign in pregnancy and danger signs during labour.
However, on birth preparedness, few of the respondents were able to identify items needed to put in place before delivery that is, birth kits as cotton wool, gloves, spirit and sanitary pads. This agrees with a study among similar respondents in Tanzania. Respondent's overall mean knowledge score about safe motherhood was 8.97±3.48 out of a 35 point knowledge scale which accessed understanding of safe motherhood, knowledge of safe motherhood practices, knowledge of danger signs in pregnancy and labour and materials needed for birth preparedness (Butawa et al., 2010). This implies a poor knowledge of safe motherhood, however to ensure effective and increased participation, men should possess relevant knowledge of safe motherhood. This finding (high awareness, poor knowledge) is consistent with several similar studies; among men and women of reproductive age in Zaria, Kaduna state (Butawa et al., 2010), Nigeria; among men in Ungogo, a community in Northern Nigeria (Iliyasu et al., 2010); in a study carried out in Osun state among men of reproductive age (Adenike et al., 2013). The respondents' major source of information on safe motherhood is the media, followed by the hospital.
From this study, there is significant relationship between respondent's level of education and knowledge of safe motherhood. This agrees with the findings from the study conducted in Kaduna, Nigeria where more than 50% of men and 43% of women gave answers that fell into the category of “poor‟ knowledge (Iliyasu et al., 2010). Men’s knowledge was considerably worse than women’s. Respondents with tertiary education showed more knowledge of safe motherhood; this is expected because of the training and exposure in the tertiary institution. Those with secondary and primary education showed lesser knowledge; this could be as a result of school curriculum at that level is been limited to.
Implication for health promotion and education
The findings from this study provide important information on the knowledge, attitude and perception of married men towards safe motherhood initiatives. The study revealed poor knowledge among married men in Ibadan North Local Government which indicates the need to strenghten existing health education programs. Men need to be enlightened on the issue of safe motherhood and the importance inherent in it. The health promotion strategies that could be useful to improve levels of knowledge of married men towards safe motherhood initiatives are through training and public enlightenment.
CONCLUSION
This study highlights the need for men in Ibadan North Local Government to have more knowledge about safe motherhood and involvement in safe motherhood practices as their knowledge about the issue has been found to be deficient. It is obvious that a huge knowledge gap exist that needs to be filled in terms of understanding of the concept of safe motherhood, knowledge about safe motherhood practices, knowledge about obstetric danger signs (danger signs during pregnancy and during labour). Married men should be knowledgeable about issues relating to maternal health such as safe motherhood so that they can have a happy and healthy family because when women in the households are incapacitated, the whole household would be affected since women have an enormous impact on their families's welfare.
RECOMMENDATIONS
It was recommended that men should be educated about safe motherhood and the importance of male participation in safe motherhood starting from an early age. There is need for increased media advocacy to promote maternal health and enlighten the public on safe motherhood and the importance of male involvement in safe motherhood.
LIMITATIONS
This study faced certain limitations which should be acknowledege. It was difficult to verify some of the information given by the respondents. Their responses may also have been influenced by socio cultural beliefs about role of men in taking care of their wife(ies) and children right from conception stage.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The authors are grateful to the research assistants and the participants for their support, cooperation and assistance during the conduct of the study.
REFERENCES
|
Adelekan AL, Edoni ER, Olaleye OS (2014). Married Men Perceptions and Barriers to Participation in the Prevention of Mother-to-Child HIV Transmission Care in Osogbo. Journal of Sexually Transmitted disease Nigeria. |
|
|
Adenike O, Esther A, Adefisoye A, Adeleye A, Olanrewaju OS (2013). Perception, attitude and involvement of men in maternal health care in a Nigerian community.Journal of Public Health and Epidemiology 5(6):262-270. |
|
|
August F, Pembe AB, Mpembeni R, Axemo P, Darj E (2015). Men's Knowledge of Obstetric Danger Signs, Birth Preparedness and Complication Readiness in Rural Tanzania. PLoS One 10(5):e0125978. |
|
|
Butawa NN, Tukur B, Idris H, Adir F, Taylor KD (2010). Knowledge and Perceptions of Maternal Health in Kaduna. African Journal of Reproductive Health 14(3):71-76. |
|
|
Erim DO, Resch SC Goldie SJ (2012). Assessing health and economic outcomes of interventions to reduce pregnancy-related mortality in Nigeria. BMC Public Health. |
|
|
Igbokwe CC, Adama GN (2011). Knowledge and practice of safe motherhood. Journal of Research in Education and Society 2(1):221-229. |
|
|
Iliyasu Z, Abubakar IS, Galadanci HS. Aliyu MH (2010). Birth preparedness, complication readiness and fathers' participation in maternity care in a northern Nigerian community. African Journal of Reproductive Health 14(1):21-32. |
|
|
Jatau AA (2014). Maternal Health Problems and Strategies for Promoting Safe Motherhood Amongst Pregnant Married Women in Kanke LGA, Plateau State, Nigeria. Mediterranean Journal of Social Sciences 5(17). |
|
|
Kwambai TK, Dellicour S, Desai M, Ameh CA, Person B, Achieng F, Terkuile FO (2013). Perspectives of men on antenatal and delivery care service utilisation in rural western Kenya: a qualitative study. BMC Pregnancy and Childbirth 13:134. |
|
|
Okereke E, Aradeon S, Akerele A, Tanko M, Yisa I, Obonyo B (2013). Knowledge of safe motherhood among women in rural communities in northern Nigeria: implications for maternal mortality reduction. Reproductive Health 10(1):57. |
|
|
Oyeyemi SO, Wynn R (2012). Giving cell phones to pregnant women and improving services may increase primary health facility utilization: a case-control study of a Nigerian project. Reproductive Health 11(1):8. |
|
|
Somé DT, Sombié I, Meda N (2013). How decision for seeking maternal care is made-a qualitative study in two rural medical districts of Burkina Faso. Reproductive Health |
|
|
Tilahun T, Coene G, Luchters S, Kassahun W, Leye E, Temmerman M, Degomme O (2013). Family Planning Knowledge, Attitude and Practice among Married Couples in Jimma Zone, Ethiopia. PLoS One 8(4) |
|
|
World Health Organization, UNFPA and World Bank (2012). Trends in maternal mortality: 1990 to 2010. 2012, World Health Organization Geneva. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


