Full Length Research Paper
ABSTRACT
Postpartum hemorrhage (PPH) is the leading cause of maternal morbidity and mortality world-wide. Although declining globally, maternal mortality is on the rise in the United States. Since uterine balloon tamponade (UBT) has been shown to be safe as well as highly effective in arresting PPH and halting shock progression, this study sought to clarify the practice and perceptions of UBT use among midwives and family physicians in the United States. A cross-sectional 12-item survey on the practice, experiences and perceptions of uterine balloon tamponade utilization for PPH management was conducted among midwives and family physicians that perform deliveries in the United States. The survey settings were one family medicine and two midwifery national conferences in the United States. One hundred and ninety-seven midwives (164; 83.2%) and family physicians (33; 16.8%) completed the surveys. The 197 providers had previously cared for a mean of 6.0 (SD= 18.8) uncontrolled PPH cases each, over the course of their career till date. Eighty (40.6%) of the 197 respondents had been involved with at least one hemorrhaging woman in which a UBT was placed, but only 13 (7.9%) of the 164 midwives and 6 (18.2%) of the 33 family physicians had ever placed a UBT device themselves. One hundred and thirty-one (73.6%) of 178 providers desired training on use of UBT. Midwives and family physicians in the United States care for women with uncontrolled PPH, however, infrequently place a UBT device. Most midwives and family physicians would like training on uterine balloon tamponade.
Key words: Uterine balloon tamponade, post-partum hemorrhage, maternal hemorrhage, emergency obstetric care.
INTRODUCTION
Postpartum hemorrhage (PPH) is the leading cause of maternal morbidity and mortality worldwide. It is estimated that PPH is responsible for 130,000 deaths and 2.6 million injured women across the globe annually (AbouZahr, 2003; World Health Organization, 2012; MacDorman et al., 2013). While many low and middle-income countries have made considerable strides to reduce their maternal mortality ratios (MMR) over the past two decades, the MMR in the United States has worsened by 136% over the past 20 years (World Health Organization, 2014). The incidence of PPH in the United States has increased by over 30% since 2004 and today it is estimated to occur in 2.9% of deliveries (Bateman et al., 2010). It is notable that one in ten women with PPH will fail first line therapies and are thus classified as having uncontrolled PPH (Ononge et al., 2016).
The most common cause of PPH is uterine atony. First-line treatment options for PPH from uterine atony include uterine massage, uterus and bladder emptying and uterotonic agents such as oxytocin, ergometrine, misoprostol and prostaglandin F2a (PGF2a) (World Health Organization, 2012). When first-line interventions are unsuccessful, PPH is called “uncontrolled”. Inter-ventions that target uncontrolled PPH from atonic uterus include aortic compression, intravenous tranexamic acid (Collaborators, 2017), uterine balloon tamponade, uterine artery embolization, and fluid, blood and blood product resuscitation once hemorrhage control has been gained (World Health Organization, 2012). Surgical approaches to uncontrolled postpartum hemorrhage include internal iliac artery ligation, uterine compression sutures and emergency hysterectomy (El Senoun et al., 2011).
Over the past seven years, the authors have studied the impact of uterine balloon tamponade in resource-limited settings by studying efficacy, safety, cost-effectiveness, barriers and facilitators to optimal use, as well as models for scale (Natarajan et al., 2016; Burke et al., 2016). During this time, UBT use for uncontrolled PPH has been endorsed by the WHO, the International Federation of Obstetrics and Gynecology, the American College of Obstetrics and Gynecology, the Royal College of Obstetrics and Gynecology and the International Confederation of Midwives, among others, as the best evidence clinical intervention (World Health Organization, 2012; Doumouchtsis et al., 2007; Tindell et al., 2013; Lalonde et al., 2006; Mavrides et al., 2016).
The authors’ work has shown that if applied in a timely fashion, uterine balloon tamponade arrests hemorrhage, halts shock progression (Burke et al., 2017), averts nearly all deaths and emergency hysterectomies (Pendleton et al., 2016; Burke et al., 2017), is “safe” and “highly cost-effective” (Mvundura et al., 2017), and can be placed successfully by any cadre, including illiterate front-line health workers (Natarajan et al., 2016). Deploying a UBT device involves placing a balloon within the uterine cavity and inflating it until hemorrhage ceases. A variety of uterine balloon devices are available, including the Sengstaken-Blakemore tube, Bakri balloon, Rusch balloon, Ebb (Belfort-Didley), and the condom catheter balloon (Pendleton et al., 2016; Dildy et al., 2014).
The authors believe that lessons learned in low- and middle-income countries may inform opportunities for improving health outcomes in highly resourced settings, such as the United States and elsewhere (Tindell et al., 2013; Pendleton et al., 2016; Burke et al., 2016). The purpose of this study was to clarify the practice and perceptions of UBT use in the United States among midwives and family physicians.
MATERIALS AND METHODS
Ethical approval was obtained from the Partners Human Research Committee (Massachusetts General Hospital, Boston, MA, USA). A cross-sectional 12-item survey on the practice, experiences, and perceptions of uterine balloon tamponade utilization for PPH management was developed by the authors through an iterative process. Uncontrolled PPH was defined as hemorrhage unresponsive to a first dose of treatment uterotonics. Appropriate utilization of uterine balloon tamponade was defined as uterine placement of a UBT in each case of uncontrolled post-partum hemorrhage. Respondent credentials, location and years spent in practice, number of deliveries attended per month, number of uncontrolled PPH cases cared for and experience with uterine balloon tamponade were recorded.
Setting
The survey instrument was administered among midwives and family physicians in the United States at three national conferences: the American College of Nurse Midwives 60th Annual Meeting and Exhibition (Washington, DC, June 27, 2015); the American Academy of Family Physicians Family Medicine Experience (Denver, CO, September 29, 2015); and the Midwives Alliance of North America Annual Convention (Albuquerque, NM, October 15, 2015).
Study population
Conference regulations did not allow solicitation beyond the authors’ exhibitor booth; therefore, the study participants were among those that voluntarily approached the booth. Providers were queried as to whether they provided obstetric delivery care. If the response was positive, the provider was invited to participate in the study and complete a survey. Oral consent was obtained and all surveys remained anonymous.
Inclusion and exclusion criteria
All providers that approached the authors’ exhibitor booth were potential study participants. Exclusion criteria included health cadres other than midwives or family physicians, providers who did not practice obstetrics, students, providers who had less than one year of clinical experience and providers who primarily practiced outside United States.
Data analysis
Each of the 12 questions was analyzed individually. If no answer was provided to a question, the individual data point was removed from both the numerator and the denominator. The registry was built using Microsoft Excel 2007 (Seattle, Washington, USA) and critically examined using standard descriptive analysis in Stata 13 (College station, Texas, USA).
RESULTS
Respondent characteristics
One hundred and ninety-seven providers met the inclusion criteria and completed the surveys. One hundred and sixty-four (83.3%) were midwives and 33 (16.7%), family physicians. The mean years of clinical practice of the 197 providers was 15.6 years (range: 1 to 45). One hundred and fifteen (70.1%) of the 164 midwives provided details of their training. Sixty (52.2%) of the 115 midwives were certified nurse midwives (CNM), 25 (21.7%) were certified professional midwives (CPM), and 18 (15.7%) were dual CPM and lay midwife (LM) certified. Among the 33 family physicians, five (15.2%) had pursued additional fellowship training in obstetric care and three (9.1%) were certified Advanced Life Support in Obstetrics (ALSO) providers. Of the 193 providers that described their practice location(s), 110 (57.0%) performed deliveries exclusively in hospitals, 63 (32.6%) in non-hospital settings (independent birthing centers and private homes) and 12 (6.2%) in both.
Experience with postpartum hemorrhage
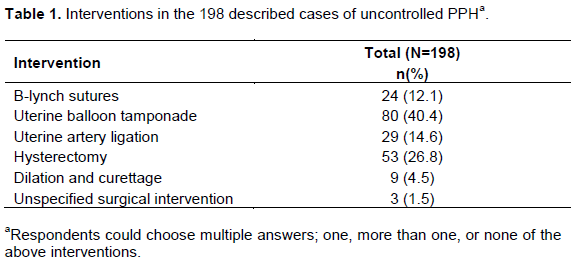
One hundred and eighty-two (92.4%) of the 197 providers estimated the number of uncontrolled PPH cases they had cared for over the course of their career. The mean number of uncontrolled PPH cases per provider over the course of their career was 6.0 (SD= 18.8). In response to a request for a narrative on each of the provider’s two most recent cases of uncontrolled PPH, 182 providers described a total of 198 women hemorrhaging un-controllably (Table 1). Respondents provided information on one, two or no cases. A UBT device was placed in 80 (40.4%) of the 198 women with uncontrolled PPH. Seventy-six (38.4%) of the 198 cases of uncontrolled PPH directly underwent surgical intervention without an attempt at a UBT device placement.
Nineteen (9.6%) of the 197 respondents had placed at least one UBT device at some point in their career. The 19 included 13 (7.9%) of the 164 midwives and 6 (18.2%) of the 33 family physicians. Two midwives reported having improvised a UBT device with a condom and Foley catheter.
Seventy-one of 110 (64.5%) respondents reported that the Bakri balloon was the most common uterine balloon at their facility. The next most common uterine balloon devices reported were the Foley catheter (8.2%) and the condom catheter (1.8%), followed by the Sengsten-Blakemore tube (0.9%), the Ebb balloon (0.9%) and the Rusch balloon (0.9%). One hundred and thirty-one (73.6%) of the 178 providers who responded that they had never placed a UBT device, wished to become trained on it in the future.
DISCUSSION
The 197 midwives and family physicians that participated in the survey collectively cared for almost 1,200 women with uncontrolled postpartum hemorrhage over the course of their careers. Although, UBT is widely endorsed by leading maternal health and obstetric physician organizations, only 9.6% of the surveyed providers had ever placed at least one. The surveyed providers reported that, in their experience, 38.4% of hemorrhaging women proceeded directly to emergency surgery with no UBT placement attempts. Most (73.5%) of the surveyed providers expressed a desire to become trained on UBT use.
Although, uterine balloon tamponade has been shown to be highly effective in the hands of all levels of healthcare providers (Tindell et al., 2013), very few had ever placed a UBT among this cohort of midwife and family physician obstetric providers despite considerable experience with women suffering from uncontrolled PPH. While this study was not designed to uncover barriers to appropriate use of uterine balloon tamponade, lack of knowledge and training were likely contributors to suboptimal use. Since many of the interviewed providers performed deliveries outside the hospitals and since it is well known that early UBT placement leads to improved outcomes (Burke et al., 2017), it appears that there may be considerable untapped opportunity for strengthening the policies and clinical pathways for the emergency care of uncontrolled PPH.
During the course of the authors’ research, it was inspiring to observe the near elimination of PPH deaths and emergency hysterectomies in major medical centers across several low-income countries, yet it is surprising and unsettling to learn about the significant number (38.4%) of hemorrhaging women reported by this cohort of providers, who were taken directly to emergency surgery without attempting uterine balloon placement. Previous research by the authors has clearly demon-strated that uterine balloon tamponade can both avert hysterectomies and other surgical interventions as well as arrest hemorrhage and shock progression (Pendleton et al., 2016; Burke et al., 2017). It appears there may have been numerous missed opportunities to avert emergency surgical intervention among those surveyed in this study.
The main limitations of this study were: being restricted to surveying only providers that were attracted to, and chose to visit the authors’ exhibitor booth. Despite the sample size of 197 obstetric midwife and family practice providers, the surveyed providers collectively had considerable experience with uncontrolled PPH. While providers that were attracted to the booth related to the topic on PPH were more likely to be more knowledgeable on PPH, the findings demonstrated a striking lack of awareness and training on uterine balloon tamponade.
CONCLUSION
There may be considerable opportunity to improve appropriate use of uterine balloon tamponade across multiple levels of obstetric delivery providers in the United States.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
This research was supported by the Ujenzi Charitable Trust.
REFERENCES
|
AbouZahr C (2003). Global burden of maternal death and disability. Br. Med. Bull. 67(1):1-11. |
|
|
Bateman BT, Berman MF, Riley LE, Leffert LR (2010). The epidemiology of postpartum hemorrhage in a large, nationwide sample of deliveries. Anesthesia Analg. 110(5):1368-1373. |
|
|
Burke, TF, Ahn R, Nelson BD, Hines R, Kamara J, Oguttu M, Dulo L, Achieng E, B Achieng, Natarajan A, Maua J, Kargbo SAS, Altawil Z, Tester K, de Redon E, Niang M, Abdalla K, Eckardt MJ (2016). A postpartum haemorrhage package with condom uterine balloon tamponade: a prospective multiâ€centre case series in Kenya, Sierra Leone, Senegal, and Nepal. BJOG 123(9):1532-1540. |
|
|
Burke TF, Danso-Bamfo S, Guha M, Oguttu M, Tarimo V, Nelson BD (2017). Shock progression and survival after use of a condom uterine balloon tamponade package in women with uncontrolled postpartum hemorrhage. Int. J. Gynecol. Obstet. doi: 10.1002/ijgo.12251 |
|
|
Collaborators WT (2017). Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet 389(10084):2105-2116. |
|
|
Dildy GA, Belfort MA, Adair CD, Destefano K, Robinson D, Lam G, Strong TH, Polon C, Massaro R, Bukkapatnam J, Van Hook JW (2014). Initial experience with a dual-balloon catheter for the management of postpartum hemorrhage. Am. J. Obstet. Gynecol. 210(2)136-e1. |
|
|
Doumouchtsis SK, Papageorghiou AT, Arulkumaran S (2007). Systematic review of conservative management of postpartum hemorrhage: what to do when medical treatment fails. Obstet. Gynecol. Surv. 62(8):540-547. |
|
|
El Senoun GA, Singh M, Mousa HA, Alfirevic Z (2011). Update on the new modalities on the prevention and management of postpartum haemorrhage. Fetal Matern. Med. Rev. 22(4):247-264. |
|
|
Lalonde A, Daviss BA, Acosta A, Herschderfer K (2006). Postpartum hemorrhage today: ICM/FIGO initiative 2004-2006. Int. J. Gynecol. Obstet. 94(3):243-253. |
|
|
Likis FE, Sathe NA, Morgans AK, Hartmann KE, Young JL, Carlson-Bremer D, Schorn M, Surawicz T, Andrews J (2015). Management of Postpartum Hemorrhage. Comparative Effectiveness Review No. 151. Agency for Healthcare Research and Quality. PMID: 26020092 |
|
|
MacDorman MF, Declerq E, Matthews TJ (2013). Recent trends in out-of- hospital births in the United States. J. Midwifery Womens Health 58(5):494-501. |
|
|
Mavrides E, Allard S, Chandraharan E, Collins P, Green L, Hunt BJ, Riris S, Thomson AJ (2016). Prevention and management of postpartum haemorrhage. BJOG 124:e106-e149. |
|
|
Mvundura M, Kokonya D, Abuâ€Haydar E, Okoth E, Herrick T, Mukabi J, Carlson L, Oguttu M, Burke, T (2017). Costâ€effectiveness of condom uterine balloon tamponade to control severe postpartum hemorrhage in Kenya. Int. J. Gynecol. Obstet. 137(2):185-191. |
|
|
Natarajan A, Alaska Pendleton A, Nelson BD, Ahn R, Oguttu M, Dulo L, Eckardt MJ, Burke TF (2016). Provider experiences with improvised uterine balloon tamponade for the management of uncontrolled postpartum hemorrhage in Kenya. Int. J. Gynecol. Obstet. 135(2):210-213. |
|
|
Ononge S, Mirembe F, Wandabwa J, Campbell OM (2016). Incidence and risk factors for postpartum hemorrhage in Uganda. Reprod. Health 13(1):38. |
|
|
Pendleton AA, Natarajan A, Ahn R, Nelson BD, Eckardt MJ, Burke TF (2016). A qualitative assessment of the impact of a uterine balloon tamponade package on decisions regarding the role of emergency hysterectomy in women with uncontrolled postpartum haemorrhage in Kenya and Senegal. BMJ Open. 6(1):p.e010083. |
|
|
Pendleton AA, Natarajan A, Ahn R, Nelson BD, Eckardt MJ, Burke TF (2016). Emergency hysterectomy for uncontrolled postpartum hemorrhage may be averted through uterine balloon tamponade in Kenya and Senegal. Int. J. Gynecol. Obstet. 133(1):124-124. |
|
|
Tindell K, Garfinkel R, Abuâ€Haydar E, Ahn R, Burke TF, Conn K, Eckardt M (2013). Uterine balloon tamponade for the treatment of postpartum hemorrhage in resource-poor settings: a systematic review. BJOG 120(1):5-14. |
|
|
World Health Organization (WHO) (2014). Trends in maternal mortality 1990 to 2013: estimates by WHO, UNICEF, UNFPA, The World Bank and the United Nations Population Division. ISBN 978 92 4 150722 6 |
|
|
World Health Organization (WHO) (2012). WHO recommendations for the prevention and treatment or postpartum haemorrhage: evidence base. Geneva: World Health Organization. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


