Full Length Research Paper
ABSTRACT
Male involvement in antenatal care helps to have safe delivery, especially in developing countries. The problem has been insufficiently studied in Ethiopia. Therefore, this study assessed male attendance and associated factors at their partners’ antenatal visits among antenatal care attendees in Bale Zone health facilities. Cross sectional study was conducted from May to June, 2017 among 609 pregnant mothers. Simple random sampling was used to select participants. Interviewer administered questionnaire was used to collect data. Data was entered into Epi-data version 3.1 and analyzed using statistical package for social sciences (SPSS version 21). Variables with p-values <0.05 were considered to declare statistical significance in multivariable logistic regression analysis. Male attendance at their partners’ antenatal visits was 41.4%. Having primary level of education (AOR=2.15, CI=1.12, 4.11), age ≥ 35 years (AOR=0.3, CI=0.1, 0.87), being farmer (AOR=0.23, CI=0.11, 0.51), having previous antenatal care visit (AOR=0.49, CI=0.26, 0.92) were factors associated with male partner involvement. Male attendance at their partners’ antenatal visits was low. Hence, health providers and other stakeholders shall create awareness and implement strategies to boost male partners’ involvement in antenatal care visit.
Key words: Antenatal visits, Bale-Zone.
INTRODUCTION
Antenatal care (ANC) is the pillars of safe motherhood and an essential elements of safe delivery (Kariuki and Seruwagi, 2016). The need for male involvement in reproductive health was one of the fore-front agenda during the International Conference on Population and Development (UNFPA, 1999). Male involvement is highly desirable in maternal health (Lowe, 2017). Because male attendance during ANC is an important strategies to reduce preventable maternal problems during pregnancy (Jennings et al., 2014). But, accessing maternal health care services seems females’ predominant responsibility and men often do not have access to participate in maternal health care services (Lowe, 2017; Kenneth et al., 2016; Bhatta, 2013). Many men do not believe that pregnancy requires their responsibility as compared to other competing social responsibilities (Jennings et al., 2014).
Although, there is reduction in maternal death and increased skilled birth attendants coverage, mothers still face unacceptable risks of death related to pregnancy, labor, and delivery (WHO, 2016). More than 50% of the global maternal deaths are due to pregnancy related complication (Kissoon et al., 2015). The World Health Organization (WHO) estimates that 303,000 women died during pregnancy and childbirth in 2015 and 99% of these maternal deaths occurred in developing countries (Kariuki and Seruwagi, 2016). An estimated 353 maternal deaths per 100,000 mothers occurred in Ethiopia where 85% of births took place at home. Evidence shows that ANC services in most developing countries to be under-utilized, median coverage rate of at least one ANC visit at 88% and four or more ANC visits at 55% (1,7,9). In Ethiopia, 57% of women attended at least one ANC visit, and 32% attended the recommended four visits (MOH, 2014).
Male participation in sexual and reproductive health is central component in empowering women (UNFPA, 1999), and different strategies have been tried to increase male attendance, mass media advertisements, incentives to women who attend ANC with their male partners, invitations to male partners to attend ANC (Osoti et al., 2014). For example in Malawi and Tanzania, providing invitation cards during pregnancy enhances male partner involvement by 50% (Nyondo et al., 2015; Jefferys et al., 2015).
Nevertheless, in most developing countries where patriarchist is dominant, it is uncommon to see male attendance during ANC(4). Men do not involve in antenatal and postnatal care, family planning and being encouraged (Sokoya et al., 2014; Mullick et al., 2005; Mullany et al., 2006; Kaye et al., 2014). This is true throughout sub-Saharan Africa, where pregnancy and childbirth is considered to be the responsibility of the woman (Kariuki and Seruwagi, 2016). In addition, to men reluctance to engage in maternal health service, health care providers like nurses have negative attitudes towards men (Ladur and Colvin, 2015).
Male attendance during ANC is important to find solutions to the main factors of maternal death: delay in decision-making to refer the mother to health facility; lack of transport in case of obstetric complications; and delay in receiving treatment within the health care facility (Kariuki and Seruwagi, 2016; Jennings et al., 2014; Ampt et al., 2015). In addition, it helps to reduce postpartum depression, improved utilization of maternal health services (Yargawa and Leonardi-bee, 2015), increases women willingness to recognize danger sign of pregnancy, attends the delivery, shortens labor, reduced need for oxytocin, anesthesia, and instrumental deliveries and reduces chance of cesarean section by 50% (Olayemi et al., 2009; Alva, 2012), increase antenatal care appointments and delivery services (Sokoya et al., 2014; Modarres, 2005). Male attendance also increases uptake of the uptake of maternal antiretroviral therapy among HIV-seropositive pregnant women (Takah et al., 2017).
Though male participation in maternal care is increasing, their attendance in providing general support is often limited (Meier, 2015), and their involvement dutring ANC varied from country to country. In developed countries, around 95% male attended at their partners ANC, but it is low in developing countries like Ethiopia (Asefa, 2014; Ganle and Dery, 2015; Vermeulen et al., 2016).
In Nepal, male partner helps the teens to attend ANC, but the women herself among adult women (Upadhyay et al., 2014). Another studies in Nepal, Malawi and Democratic republic of Congo (DRC) indicated women who received education with husbands and partner notification had more chance to have maternal care services (Mphonda et al., 2014; Mullany et al., 2006; Gill et al., 2017; Kululanga et al., 2011).
In rural and peri-urban area in Uganda, 42 to 66% of mothers have been accompanied by husbands during antenatal care (Tweheyo et al., 2010; Kakaire et al., 2011) In Nigeria, around 48% of women did not think it was their husbands' place to attend antenatal clinic, 73% of husbands accompanied their wives to the hospital for their last delivery (Olayemi et al., 2009), 82.4% had desire to accompany during ANC clinic visits; 14.2% male partners attended previous delivery and 84.8% of the women were satisfied with the experience (Abiodun et al., 2015). Another study in Northern Nigeria, showed 62% of men believed that their presence was not needed (Zubairu et al., 2010).
In Johannesburg, South Africa, 92% of mothers preferred their husbands attendance at ANC and 14% reported that their husbands attended during the current pregnancy (Yende et al., 2016). In rural Rwanda, the level of men ANC attendance was 29.4%, while 22.3% women were accompanied to the labor ward (Richard, 2016). A study conducted in Ghana indicated that 35, 44, and 20% of men accompanied their partners to antenatal care, delivery, and postnatal care services, respectively (Craymah et al., 2017).
In Kenya, 72% of mothers felt that their male spouses should at least set aside while 54% indicated that they wanted their male partners to be accompanying them (Nanjala and Wamalwa, 2012). Another study in Kenya showed 63% of women consented to male participation, but male accompany during ANC is only 26.2% (Aluisio et al., 2016). In Burkina Faso, to make use of maternal care, they need consent of a member of the family particularly, the partner (Somé et al., 2013).
In Ethiopia, male attendance during ANC ranged from 20 to 60% (Asefa, 2014; Haile and Brahn, 2014) and husband’s approval has a greater effect on maternal care utilization especially for women under the age of 20 years (Biratu and Lindstrom, 2006). This might be due to the traditional view that men are autonomous and have great control over social, economic and their partners.
Maternal age and parity less than four (Abiodun et al., 2015), residence, educational status, last delivery in health facility (Olayemi et al., 2009; Asefa, 2014; Abiodun et al., 2015; Tweheyo et al., 2010), male partner attended prenatal health education (Kariuki and Seruwagi, 2016; Mullany et al., 2006; Wai et al., 2015), long waiting time at the health unit, lack of transport, walking distance ≥ 1 h to health facility, fear of being tested for HIV, being polygamous, having a concurrent task or job demand, non-invitation by the wife, poor communication between men and female are factors associated with low male attendance during ANC (Tweheyo et al., 2010; Byamugisha et al., 2011).
Higher maternal education level and formal occupation of spouse are associated with male partner involvement (MPI) (Richard, 2016). In Ethiopian, occupation of women being a rural resident, age difference between a wife and their spouse (Asefa, 2014), and lower husband educational level (Addisalem, 2014) contributed for low male involvement while employed mother, living together and previous history of couple counselling increase the chance of male involvement during ANC (Haile and Brahn, 2014; Addisalem, 2014).
Male attendance in maternal health is often ignored by health programs in developing countries. In Ethiopia, few researches were conducted regarding male partners’ attendance during ANC. Therefore, this study aimed to assess the level of male attendance and associated factors at their partners’ antenatal visits among antenatal care attendees in Bale Zone, South East, Ethiopia. Hence, findings of the study would help to inform policy makers to design appropriate programs that enhance males’ involvement in antenatal care and act on gaps identified. Furthermore, findings would be used as a resource to other researchers on these issues.
Operational definitions
Male partner
Is an individual with whom the pregnant woman was in intimate sexual relationship and was responsible for her pregnancy whether they were legally married or not.
Male partner involvement
Husband’s attendance at the time of antenatal checkup and husband’s participation in birth preparedness measured based on the women’s reports. The variable was coded as “Yes” if the woman attended ANC and her spouse accompanied her; “No“ if the woman attended ANC but her spouse did not accompany her.
MATERIALS AND METHODS
Study design, period and setting
Institutional based cross-sectional study was conducted among 609 pregnant women who were attending antenatal care in selected health facilities of Bale zone from May to June, 2017.
Sample size, technique and procedures
Single proportion formula was used to calculate the sample size by assuming Z α/2 = 1.96 (standard score value for 95% confidence level of two sides normal distribution), p = 59.9%, d (tolerated margin of error) = 5%, non-response rate = 10%, and design effect = 1.5. Using simple random sampling technique, 20% (16 health centers) of health centers (HC) and all hospitals (4 hospitals) were selected based on the proposed sample fraction guideline for assessing the operation of District Health systems developed by WHO regional office for Africa (Sambo et al., 2003). The sample size was determined by proportionate allocation formula based on their average monthly intake of antenatal services provided by each health facilities.
Study variables
The main outcome variable was prevalence of male partners’ attendance during the current ANC while the independent variables were demographic information (age, marital status, level of education, occupation residence, religion, living status, number of live children, years living with husband, type of marriage (marriage, cohabiting, divorce, and/or separated), family size, age at first marriage, obstetrics characteristics (gravida, parity, intention of pregnancy and ANC follow up) and perception of women towards paternal involvement.
Data collection tools and procedures
The data was collected using pre-tested structured interviewer administered questionnaire. The questionnaire was designed by the researchers after reviewing literatures. All questionnaires were prepared in English language, and then translated to Afan Oromo and Amharic (local language) which were used for data collection and re-translated back to English to check for any inconsistencies. To keep quality of data, pretest was conducted; half day training was given to data collectors and supervisors and completed questionnaires were reviewed to check for its consistency and completeness.
Ethical approval
Ethical review committee of College of Medicine and Health Sciences, Madda Walabu University approved the study. Permission to conduct the study was obtained from Bale Zone administrative office and written informed consent was taken from each participant.
Data analysis
The completed questionnaires were checked for completeness, edited sorted and entered into Epi-Data version 3.1, and exported to version 21 of Statistical Package for the Social Sciences (SPSS) for analysis. The assumption of logistic regressions was checked. Then, binary logistic regression analysis was done to see the independent effect of predictors on the dependent variables and predictors with P-valve ≤ 0.25 were entered in the multivariable logistic regression analysis model to identify final predictors of male involvement during ANC after controlling other independent variables. Odds ratio and 95% CI were calculated and P≤0.05 was considered statistically significant. Finally, the result was described in text form and summarized and presented in tables and graphs.
RESULTS
Socio-demographic characteristics of the study participants
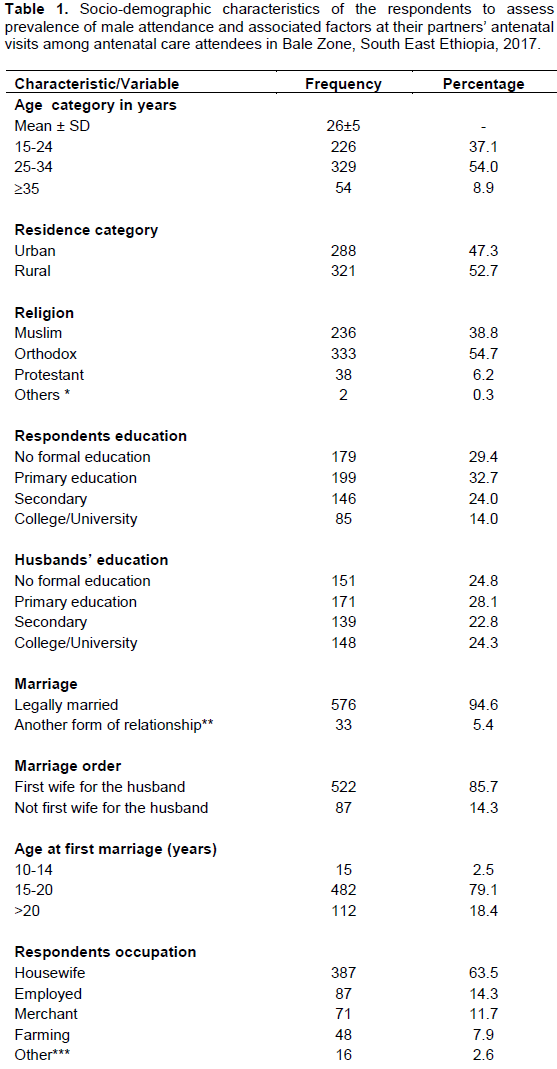
All (609) study participants were interviewed that gave a response rate of 100%. The age of the participants ranged from 15 to 40 years (mean: 26±5 years). Three hundred and twenty one (52.7%) and 576 (94.6%) were from the rural area and legally married, respectively. Almost 200 (32.7%) of the participants had attended primary level of education. In terms of occupation, 387 (63.5%) were house wives, while 297 (48.8%) of their husband were farmers. Around 480 (79.1%) and 270 (44.7%) of the study participants were married in the age group of 15 to 20 years and have lived with their partners less than five years, respectively. To access health facility, 248 (40.7%) of the respondents traveled more than 30 min (Table 1).
Pregnant women’s expectation from their male partners in antenatal care involvement
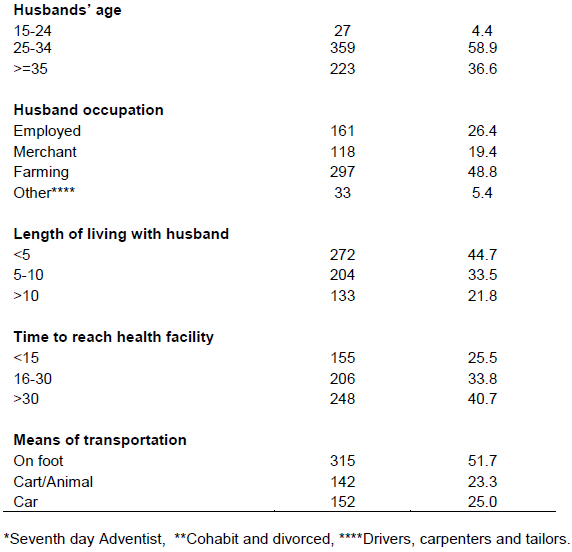
The majority, 515 (84.6%) of the respondents responded “yes” to the question “should male attend ANC visit?” with their pregnant partner. Five hundred thirty-six (88.0%) of the respondents reported that male partners should be educated about pregnancy with their partner; of this 79.5% mentioned, a male whose wife is pregnant should be educated how to support the pregnant mother. Majority respondents agreed, there must be legitimate enforcement for a male to attained ANC visit (82.1%), and 90.5% on HIV testing at ANC visit (Table 2). Among 252 husbands came with their pregnant partners, only 36.0% were informed about the presence of HIV counseling and testing (Table 2). The vast majority of respondents (94.9%) liked someone with them during labor. Two hundred and eighty (48.4%) of the respondents, among those who needed someone during delivery (their husband); followed by those who needed their mother 43.4%. Five hundred and four (82.8%) respondents had believed that they had good communication about ANC/pregnancy with their husband (Table 2).
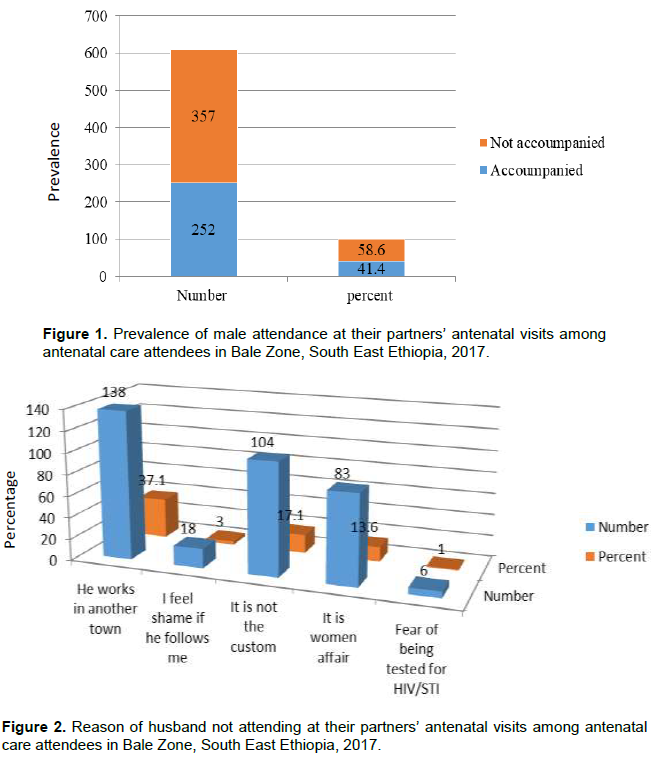
Prevalence of male attendance at their partners’ antenatal visits
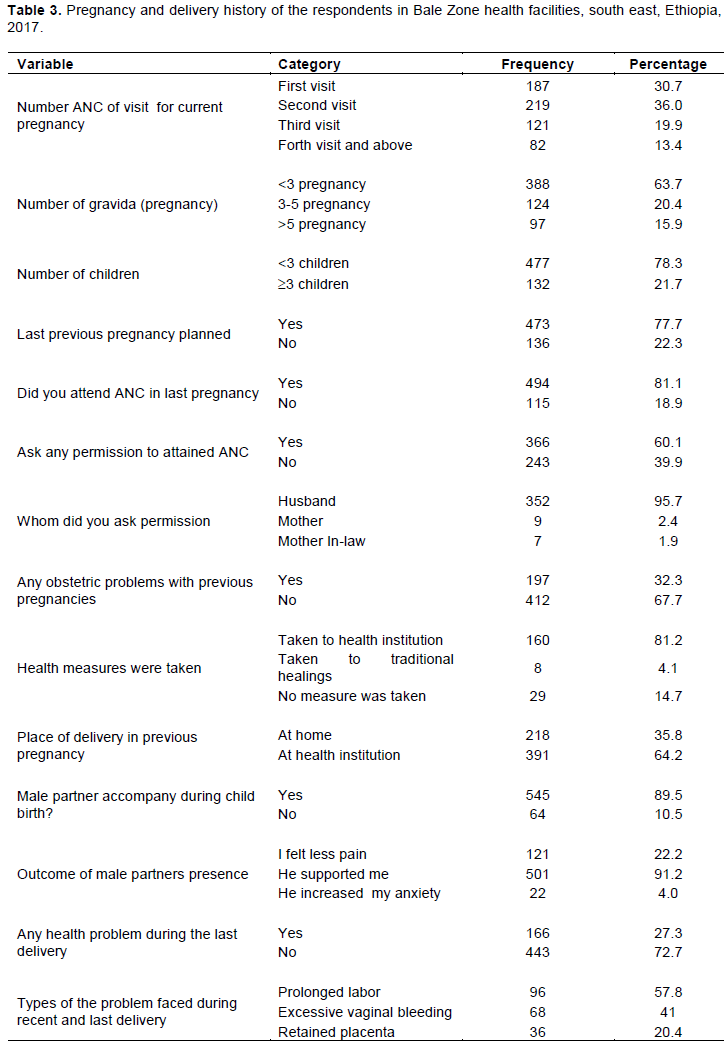
In this study, the prevalence of male partner involvement was 253 (41.4%). More than half of the respondents 357 (58.6%) were not accompanied by their partner during ANC (Figure 1). Reasons for not accompanied by their male partner were husband working in another town 138 (37.1%), not the custom 104 (17.1%) and it is women affair 83 (13.6%) (Figure 2).
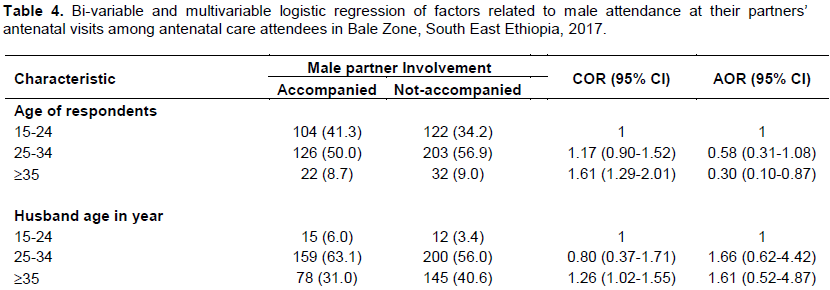
Pregnancy and delivery history of the respondent
Around 219 (36%) of mothers attended their second visit in the current pregnancy. Their gravidity ranges from 2 to 12 pregnancies and 388 (63.7%) had <3 pregnancies. Around 480 (78.3%) of the respondents had ≤3 children. Almost 78% of recent last pregnancy was planned and 19% of them had no ANC follow up history. Among 352 (95.7%) respondents asked permission from their husband. Two hundred eighteen (35.8%) gave past birth at home before the current pregnancy and 27.3% faced delivery related problems, prolonged labor 57.8%, and excessive vaginal bleeding 41.0% (Table 3). During labor and delivery, 578 (94.9%) want company, 280 (48.4%) prefer the male partner with 501 (91.2%) who reported their partner supported them and 121 (22.2%) felt less pain as a result of being accompanied by male partner (Table 3). One hundred and ninety-seven (32.3%) of the respondents faced different pregnancy related problems of which a severe headache, that accounts for 47.7%, was the leading problem followed by blurred vision and vaginal bleeding, 36.5 and 34.5%, respectively (Figure 3).

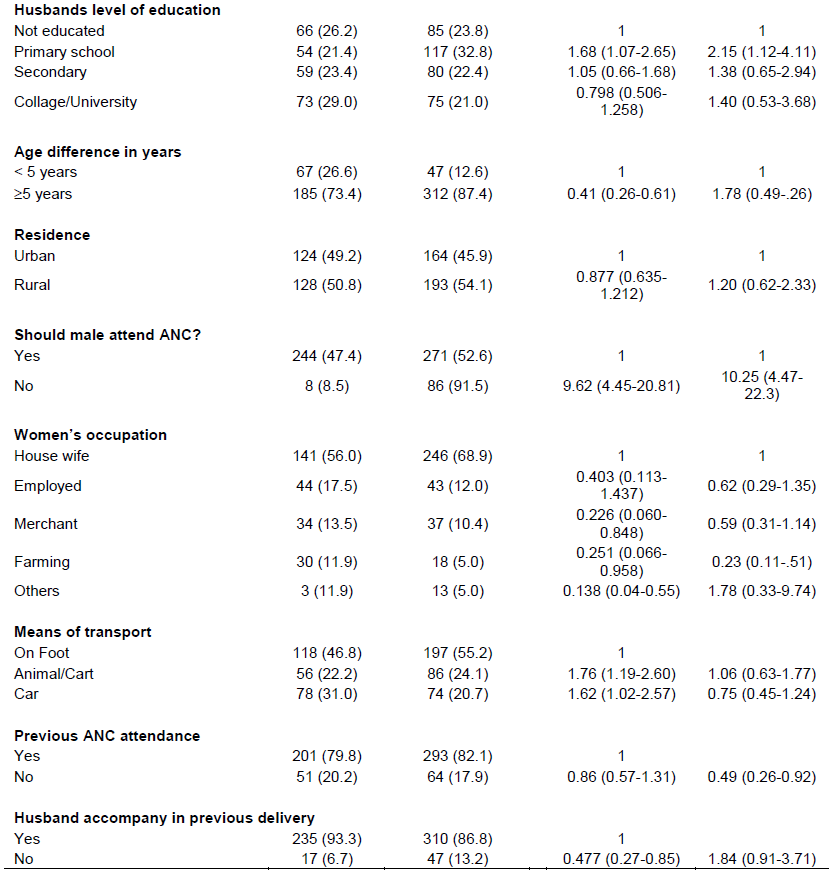
Factors associated with male partner involvement
In the bivariate analysis, participant age ≥35 years, husband age ≥35 years, level of education, occupation, age difference, having good communication, believing male should attend ANC, husband accompanied in recent delivery, means of transport had association with male partners attendance during their ANC visits. The odds of women age ≥ 35 years were 0.3 times less likely to have their partner attendance during ANC as compared to those in the age group of 15 to 24 years (AOR: 0.3, 95% CI: 0.1, 0.87). The odds of having husband with primary level of education were 2.15 times more likely to have male attendance during ANC (AOR: 2.15, 95% CI: 1.12, 4.11). The odds of having age difference ≥ 5 years between a wife and husband were 1.78 times more likely to have male partners attendance during ANC (AOR: 1.78, 95% CI: 0.49, 0.26). The odds of being farmers were 0.23 more likely not to attend ANC (AOR: 0.23, 95 CI: 0.11, 0.51). The odds of having previous ANC attendance was 0.49 times more likely to have male attendance (AOR: 0.49, 95% CI: 0.26, 0.92).
Women who think the male should attend ANC were11.04 times (AOR: 11.04, 95% CI: 4.82, 25.31) more likely to more than male attendance during ANC. The odds of having good communication with their male partner were 2.97 times more likely to have their male attendance during ANC visits (AOR: 2.83, 95% CI: 1.45, 5.52) (Table 4).
DISCUSSION
This study generated information regarding male attendance and associated factors at their partners’ antenatal visits among antenatal care attendees. Accordingly, the prevalence of male attendance at their partners’ ANC visit was low (41.4%) which means fewer number of women reported that their partners attended during their ANC follow up. This finding is higher than studies conducted in Harari (19.7%), Tigray (24.7%), and Fentaly, Ethiopia (30.5%), and Wakiso, Uganda (6%) (Asefa, 2014; Kariuki and Seruwagi, 2016; Gebrehiwot et al., 2012). Since, ANC is government concern in the world; husbands might get information regarding their responsibility during ANC. The finding is lower than study findings in Inda and Gulu districts, Uganda, Ambo and Addis Ababa, Ethiopia (Tweheyo et al., 2010; Addisalem, 2014; Dereje, 2016; Abhishek, 2009). This difference might be due to the difference in time and residence of the participants.
The participants reported husband working in another town (37.1%), not a custom (17.1%) and its women’s affair (13.6%) were reasons of non-accompany. The findings are similarly to a study conducted in Harari where respondents stated that their partners were occupied with routine jobs (54.6%), males consider the ANC as the sole responsibility of the wife/women 13.6% (Asefa, 2014) and in Nigeria where husbands were working in another town (41.5%) and not a custom (9.2%) (Abiodun et al., 2015).
In this study, majority (95.7%) of the respondents asked their husband to have ANC. This finding is likely similar to a finding in Burkina Faso where pregnant mothers asked their male partners to consent to visiting health facility (Somé et al., 2013). This might be due to male are dominant in deciding the family issues in sub-Saharan Africa.
Most of the respondents reported that they want their male partners’ participation during ANC. They stated that male partners’ education regarding how to support the pregnant women, problems during pregnancy and sexual relation during pregnancy is necessary. These findings are almost similar to a study in Harari, Cameroon and Nigeria where women wanted their partner’s involvement in ANC and male partners need to be educated on the care of pregnant women (Asefa, 2014; Abiodun et al., 2015; Nkuoh et al., 2013).
Being from rural residences, increased age difference (≥5 years) between women and their male partner increases the likelihood of non-attendance during ANC. The finding is supported by study conducted in Harari, Ethiopia (Asefa, 2014), and Fentaly district, Ethiopia where pregnant mothers living in urban were more likely to have male attendance.
Male partner who have educational level of primary and above are more likely to involve in their partners ANC visits. This finding is supported by studies conducted in India, Uganda and Nigeria where increased educational level was associated with more attendance in maternal care (Zubairu et al., 2010; Kariuki and Seruwagi, 2016).
But, maternal educational level has no association with male partner involvement during ANC which supports a study finding in Kinshasa (Gill et al., 2017). This might be explained by male partners with some basic level of education of better understanding of the complications associated with unskilled delivery. Education also enables men to discard the negative attitudes and cultural beliefs.
The study has limitations since it relied on mothers self-reporting of their male partners’ attendance during ANC which may be under- or over-reported. In addition, cross-sectional data was used and therefore causality and direction of results cannot be determined; longitudinal analysis may provide additional insight into male partner attendance during ANC and investigate all factors that may be associated with male partner involvement in ANC in future studies.
Implications for practice
As earlier shown and mentioned by different literatures understanding level and factors of male attendance during their partners’ ANC visits are important to fill gaps and set strategies to boat male participation in maternal health services. The result of the current study reflects the usefulness of promoting male partners participation during ANC and reducing factors that hinder them in the studied health care settings. As male attendances during ANC increases, women will be supported to have full ANC visits so that pregnancy related maternal morbidity and mortality can be reduced.
CONCLUSIONS
Despite the fact that male partners’ attendance in the maternal ANC service is increasing, it remains low in Ethiopia. Furthermore, being older, farmer, age difference of more than five years, previous ANC attendance, and husband attendance in previous delivery increase the likelihood of male partners non-attendance at their partners ANC visit. Health providers and other stakeholders need to focus on educating men on their shared responsibility in ANC. Educating women with their partners when they come to ANC could improve male attendance in future ANC visit.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the study participants who gave their unlimited information.
REFERENCES
|
Abhishek S, Ram (2009). Men's involvement during pregnancy and childbirth: Evidence from rural Ahmadnagar, India. Population Review 48(1). |
|
|
Abiodun S, Adeniran A, Aboyeji P, Adegboyega A, Fawole OR, Balogun KT, Adesina PIA (2015). Male Partner's Role during Pregnancy, Labour and Delivery: Expectations of Pregnant women in Nigeria. ijnInternational Journal of Health Sciences 9(3):305. |
|
|
Addisalem DA (2014). Assessment of Husband Involvement during Pregnancy and Child Birth in AkakiKaliti Sub-city, Addis Ababa, Ethiopia (Doctoral dissertation, Addis Ababa University). |
|
|
Aluisio AR, Bosire R, Betz B, Gatuguta A, Kiarie JN, Nduati R (2016). Male partner participation in antenatal clinic services is associated with improved HIV-free survival among infants in nairobi, kenya: a prospective cohort study. Journal of Acquired Immune Deficiency Syndromes 73(2):169. |
|
|
Alva S (2012). Gender Attitudes and Male Involvement in Maternal Health Care in Rwanda. In: Annual meetings of the Population Association of America, San Francisco pp. 2-5. |
|
|
Ampt F, Mon MM, Than KK, Khin MM, Agius PA, Morgan C (2015). Correlates of male involvement in maternal and newborn health: a cross-sectional study of men in a peri-urban region of Myanmar. BMC Pregnancy and Childbirth 15(1):122. |
|
|
Asefa F (2014). Male Partners Involvement in Maternal ANC Care: The View of Women Attending ANC in Hararipublic Health Institutions, Eastern Ethiopia. Science Journal of Public Health 2(3):182-188. |
|
|
Bhatta DN (2013). Involvement of males in antenatal care, Birth preparedness, Exclusive breast feeding and immunizations for children in Kathmandu, Nepal. BMC Pregnancy and Childbirth 13(1):14. |
|
|
Biratu BT, Lindstrom DP (2006). The influence of husbands ' approval on women's use of prenatal care: Results from Yirgalem and Jimma towns, south west Ethiopia. Ethiopian Journal of Health Development 20(2):84-92. |
|
|
Byamugisha R, Strøm AN, Ndeezi G, Karamagi CAS, Tylleskär T, Tumwine JK (2011). Male partner antenatal attendance and HIV testing in eastern Uganda: A randomized facility-based intervention trial. Journal of the International AIDS Society 14(1):43. |
|
|
Craymah JP, Oppong RK, Tuoyire DA (2017). Male Involvement in Maternal Health Care at Anomabo, Central Region, Ghana. International Journal of Reproductive Medicine. |
|
|
Dereje BD, Gizachew AB (2016). Involvement of male in antenatal care, birth preparedness and complication readiness and associated factors in Ambo Town, Ethiopia. |
|
|
Ganle JK, Dery I (2015). "What men don"t know can hurt women's health': a qualitative study of the barriers to and opportunities for men's involvement in maternal healthcare in Ghana. Reproductive Health 12(1):93. |
|
|
Gill MM, Ditekemena J, Loando A, Ilunga V, Temmerman M, Fwamba F (2017). "The co-authors of pregnancy": leveraging men's sense of responsibility and other factors for male involvement in antenatal services in Kinshasa, DRC. BMC Pregnancy and Childbirth 17(1):409. |
|
|
Gebrehiwot H, Gebregziabher W, Gidey G (2012). Assessment of husbands' participation on birth preparedness and complication readiness in Enderta Woreda, Tigray Region, Ethiopia. J Women's Heal Care 3(140):2167-0420. |
|
|
Haile F, Brahn Y (2014). Male partner involvements in PMTCT: a cross sectional study. BMC Pregnancy and Childbirth 14(1):65. |
|
|
Jefferys LF, Nchimbi P, Mbezi P, Sewangi J, Theuring S (2015). Official invitation letters to promote male partner attendance and couple voluntary HIV counselling and testing in antenatal care: An implementation study in Mbeya Region, Tanzania. Reproductive Health 12(1):95. |
|
|
Jennings L, Na M, Cherewick M, Hindin M, Mullany B, Ahmed S (2014). Women's empowerment and male involvement in antenatal care: analyses of Demographic and Health Surveys (DHS) in selected African countries. BMC pregnancy and Childbirth 14(1):297. |
|
|
Kakaire O, Kaye DK, Osinde MO (2011). Male involvement in birth preparedness and complication readiness for emergency obstetric referrals in rural Uganda. Reproductive Health 8(1):12. |
|
|
Kariuki K, Seruwagi G (2016). Determinants of male partner involvement in antenatal care in Wakiso District, Uganda. British Journal of Medicine and Medical Research 7:18. |
|
|
Kaye DK, Kakaire O, Nakimuli A, Osinde MO, Mbalinda SN, Kakande N (2014). Male involvement during pregnancy and childbirth: Men's perceptions, practices and experiences during the care for women who developed childbirth complications in Mulago Hospital, Uganda. BMC Pregnancy and Childbirth 14(1):54. |
|
|
Kenneth N, Sonto M. Maputle HS (2016). Male partners' views of involvement in maternal healthcare services at Makhado Municipality clinics, Limpopo Province, South Africa. African Journal of Primary Health Care & Family Medicine 8(2):1-5. |
|
|
Kissoon N, Dugani S, Bhutta ZA (2015). 3 Maternal and child health: Gains, but a long journey ahead. Canadian Medical Association Journal 187(16):E471-E472. |
|
|
Kululanga LI, Sundby J, Malata A, Chirwa E (2011). Striving to promote male involvement in maternal health care in rural and urban settings in Malawi - a qualitative study. Reproductive Health 8(1):36. |
|
|
Ladur AN, Colvin CJ, Stinson K (2015). Perceptions of community members and healthcare workers on male involvement in prevention of mother-to-child transmission services in Khayelitsha, Cape Town, South Africa. PLoS One 10(7):e0133239. |
|
|
Lowe M (2017). Social and cultural barriers to husbands' involvement in maternal health in rural Gambia. The Pan African Medical Journal 27. |
|
|
Meier ME, Avillaneda L (2015). A Literature Review of Paternal Involvement in Prenatal Care. Journal of Family Strengths 15(1):10. |
|
|
Modarres NV (2005). Couple's attitudes to the husband's presence in the delivery room during childbirth. Eastern Mediterranean Health Journal 11(4):828-834. |
|
|
Ministry of Health (MOH) (2014). Ethiopia Mini Demographic and Health Survey 2014. Cental statistical agency 2014. |
|
|
Mphonda SM, Rosenberg NE, Kamanga E, Mofolo I, Boa E, Mwale M (2014). Assessment of Peer-Based and Structural Strategies for Increasing Male Participation in an Antenatal Setting in Lilongwe, Malawi. African Journal of Reproductive Health 18(2):97-104. |
|
|
Mullany BC, Becker S, Hindin MJ (2006). The impact of including husbands in antenatal health education services on maternal health practices in urban Nepal: Results from a randomized controlled trial. Health Education Research 22(2):166-176. |
|
|
Mullany BC, Becker S, Hindin MJ (2006). The impact of including husbands in antenatal health education services on maternal health practices in urban Nepal : Results from a randomized controlled trial. Health Education Research 22(2):166-176. |
|
|
Mullick S, Kunene B, Wanjiru M (2005). Involving Men in Maternity Care: Health Service Delivery Issues. Agenda Special Focus 6:124-35. |
|
|
Nanjala M, Wamalwa D (2012). Determinants of Male Partner Involvement in Promoting Deliveries by Skilled Attendants in Busia, Kenya. Global Journal of Health Science 4(2):60. |
|
|
Nkuoh GN, Meyer DJ, Nshom EM (2013). Women's attitudes toward their partners' involvement in antenatal care and prevention of motherâ€toâ€child transmission of HIV in Cameroon, Africa. Journal of Midwifery and Women's Health 58(1):83-91. |
|
|
Nyondo AL, Choko AT, Chimwaza AF (2015). Invitation Cards during Pregnancy Enhance Male Partner Involvement in Prevention of Mother to Child Transmission (PMTCT) of Human Immunodeficiency Virus (HIV) in Blantyre, Malawi : A Randomized Controlled Open Label Trial. PLoS One 10(3):e0119273. |
|
|
Olayemi O, Bello FA, Aimakhu CO, Obajimi GO AA (2009). Male participation in pregnancy and delivery in Nigeria: A survey of antenatal attendees. Journal of Biosocial Science 41(4):493-503. |
|
|
Osoti A, Han H, Kinuthia J, Farquhar C (2014). Role of male partners in the prevention of mother-to-child HIV transmission. Research and Reports in Neonatology 4:131-138. |
|
|
Richard K, Malande OO (2016). Involvement for obstetric emergencies in rural Rwanda. The Pan African Medical Journal 25 p. |
|
|
Sambo L, Chatora R, Goosen E (2003). Tools for assessing the operationality of district health systems . World Health Organization, Regional Office for Africa. |
|
|
Sokoya M, Farotimi A, Ojewole F (2014). Women's perception of husbands' support during pregnancy, labour and delivery. IOSR Journal of Nursing and Health Science 3(1):45-50. |
|
|
Somé DT, Sombié I, Meda N (2013). How decision for seeking maternal care is made--a qualitative study in two rural medical districts of Burkina Faso. Reproductive Health 10(1):8. |
|
|
Takah NF, Kennedy ITR, Johnman C (2017). The impact of approaches in improving male partner involvement in the prevention of mother-to-child transmission of HIV on the uptake of maternal antiretroviral therapy among HIV-seropositive pregnant women in sub-Saharan Africa: a systematic review and m. BMJ Open 7(11):e018207. |
|
|
Tweheyo R, Konde-lule J, Tumwesigye NM, Sekandi JN (2010). Male partner attendance of skilled antenatal care in peri-urban Gulu district, Northern Uganda. BMC Pregnancy and Childbirth 10(1):53. |
|
|
Tweheyo R, Konde-Lule J, Tumwesigye NM, Sekandi JN (2010). Male partner attendance of skilled antenatal care in peri-urban Gulu district, Northern Uganda. BMC Pregnancy and Childbirth 10(1):53. |
|
|
UNFPA (1999). 5 Programme of Action of the International Conference on Population and Development: 20th Anniversary Edition. |
|
|
Upadhyay P, Liabsuetrakul T, Shrestha AB, Pradhan N (2014). Influence of family members on utilization of maternal health care services among teen and adult pregnant women in Kathmandu, Nepal : a cross sectional study. Reproductive Health 11(1):92. |
|
|
Vermeulen E, Solnes Miltenburg A, Barras J, Maselle N, van Elteren M, van Roosmalen J (2016). Opportunities for male involvement during pregnancy in Magu district, rural Tanzania. BMC Pregnancy and Childbirth 16(1):66. |
|
|
Wai KM, Shibanuma A, Oo NN, Fillman TJ, Saw YM, Jimba M (2015). Are husbands involving in their spouses' utilization of maternal care services?: A cross-sectional study in Yangon, Myanmar. PloS One 10(12):e0144135. |
|
|
World Health Organization (WHO) (2016). Time to respond: A report on the global implementation of maternal death surveillance and response. |
|
|
Yargawa J, Leonardi-bee J (2015). Male involvement and maternal health outcomes : systematic review and meta-analysis. Journal of Epidemiol Community Health jech-2014. |
|
|
Yende N, Rie A Van, West NS, Bassett J, Schwartz SR (2017). Acceptability and preferences among men and women for male involvement in antenatal care. Hindawi Journal of Pregnancy 8 p |
|
|
Zubairu I, Abubakar IS, Galadanci HS, Aliyu MH (2010). Birth preparedness, complication readiness and fathers' participation in maternity care in a northern Nigerian community. African Journal of Reproductive Health 14(1). |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


