Earlier studies conducted in Africa have generally generated evidence that women in low income countries have a high physical workload that is sustained during pregnancy. This high physical workload was believed to contribute to the high incidence of low birth weight. However, there are only few published studies on physical activity among pregnant women in low-income countries, and most have been based on questionnaires. This research aims to explore the status of physical activity and factors influencing physical activity in pregnant women in Africa. Pubmed, Scopus and Cinahl databases were searched with no date restrictions using the Mesh terms “pregnancy”, “physical activity”, “exercise” and “Africa”. Articles were independently screened by 2 reviewers. A meta-analysis could not be done due to the heterogeneity of the articles hence a narrative synthesis of evidence was done instead. The results revealed a total of 5 articles from Africa. The major form of physical activity reported was household activities which fall below the recommended intensity during pregnancy. Physical activity tended to decrease as pregnancy progressed. The study thus, low levels of physical activity in pregnancy are prevalent in developing countries as well as in developed countries. However existing published data are too few to generalize to the whole of the African continent household activities.
Earlier studies conducted in Africa have generally generated evidence that women in low-income countries have a high physical workload that is sustained during pregnancy (Benefice and Cames, 1999; Roberts et al., 1982; Spurr et al., 1996; Lawrence and Whitehead, 1988). This high physical workload was believed to contribute to the high incidence of low birth weight (Rao et al., 2003). However, there are only a few published studies on physical activity among pregnant women in low-income countries, and most have based on questionnaires (Hjorth et al., 2012).
There is ample and consistent evidence that promoting physical activity in women of reproductive age may be a promising approach for the prevention of excessive weight gain, gestational diabetes mellitus and subsequent affected by gestational diabetes mellitus (Ferraro et al., 2011). At least 30 min of moderate activity or 8000 steps/day equivalent to approximately 7.5 MET-h/wk are recommended for beneficial results (McParllin et al., 2010).
In a meta-analysis conducted by Dugas et al. (2011) it was suggested that women from developing countries perform similar amounts of physical activity as women from developed countries when assessed by doubled labelled water raising questions about actual physical workload. However, these data provide no insight into the patterns of physical activity. Thus, there is a need for more studies with objective methods for assessing physical activity among pregnant women in low-income countries. The objective of this literature review, therefore, is to assess the patterns of physical activity in pregnant women in Africa.
Historically, pregnancy was regarded as a state of confinement. More recently, however, research has demonstrated many potential health benefits of aerobic and strength-conditioning exercise in pregnancy and the postpartum period. It is now considered safe, and even advisable, for otherwise healthy pregnant women to initiate or continue an active lifestyle during pregnancy. Many anatomical and physiological changes take place during pregnancy and while there is no evidence to suggest that exercise in pregnancy is associated with any maternal of fetal adverse outcomes, it is prudent to adjust exercise regimes where necessary to avoid potential harm. Contact sports as well as sports associated with a risk of falling should be avoided. Brisk walking, stationery cycling, and swimming are examples of aerobics exercises that are recommended in pregnancy.
It is advisable for all pregnant women wishing to pursue exercise in pregnancy to be screened for contra-indications and risk factors, for subsequent recommendations to be made on an individual basis. It is useful to classify pregnant women into sedentary, recreational and competitive athlete, as this will help guide the intensity of exercise. All women should be aware of warning symptoms that may develop during physical activity, and advised to stop the exercise and seek medical advice should they occur. Exercise forms only one component of a healthy lifestyle. A nutritious diet, adequate hydration, and abstinence from smoking, alcohol and illicit drugs are crucial in maintaining optimal health during pregnancy (Horak and Osman, 2012).
Lack of exercise during pregnancy might result in loss of muscular and cardiovascular fitness, excessive maternal weight gain with a raised risk of GDM, varicose veins, dyspnea, lower back pain and poor psychological adjustment (Royal College of Obstetricians and gynecologists - RCOG, 2006). An initial approach to becoming more physically active could be to encourage women to incorporate unstructured physical activity into daily living, both before and during pregnancy. Giving women an appropriate exercise prescription can encourage them to participate in physical activity (Colberg et al., 2013).
Measuring physical activity
Measurement of physical activity in Africa has its own challenge. Most of the questionnaires that have been developed are appropriate for the developed world and might not apply in the resource limited setting in Africa (Wareham et al, 2000). Though the instruments used have high reliability, issues of validity remain a problem. This is because physical activity is multidimensional encom-passing such concepts as energy expenditure and aerobic fitness. Selection of a measurement method that can be used as the comparison or gold standard is very difficult. However the most objective method for measuring physical activity in individuals, the doubly labelled water technique, is extremely expensive. It has only been used in a few studies even in the developed world (Schuit et al., 1997). The method of heart rate monitoring and movement sensing has been said to be the next best objective method (Sobngwi et al., 2001). However the method makes the field work much harder though it can produce reliable results. The method, therefore has potential to be used as a validation method and as an epidemiological tool in its own right (Wareham et al., 2000).
Guidelines for physical activity in pregnancy
A number of guidelines have been developed for physical activity in pregnant women. There are guidelines from the American College of Obstetricians and Gynecologists (ACOG, 2002), the society of exercise physiology. In support of these guidelines the South Africa Sports Medicine Association came up with a position statement on Exercise in pregnancy (Barsky et al., 2012).
Recommendations for physical activity in pregnancy
Women with no medical or obstetric complications should be encouraged to participate in aerobic and strength-conditioning training at moderate intensity on most or all days of the week. The goal should be to maintain good fitness level throughout the pregnancy. Activities such as jogging and hiking that minimize risk of loss of balance and fetal trauma should be encouraged.
However high risk activities such as contact and collision sports, vigorous racquet games, gymnastics and horseback riding among others should be avoided. Women should be advised that exercise does not increase the incidence of adverse pregnancy and neonatal outcomes neither do moderate exercise during lactation affect the quantity or composition of breast milk or infant growth.
Exercise intensity in pregnancy
Determination of optimal intensity of exercise for pregnant women is a controversial element of the exercise regimen with much attention being paid to limiting the heart rate to restrict adverse effects. The rate of perceived exertion is an alternative to heart rate for monitoring exercise. The Borg scale measures the rate of exertion and a score of between 12 to 14 on a 6 to 20 scale indicates somewhat hard work out (SOGP/CSEP, 2003).
Recent research has determined that, compared with less vigorous activities, exercise intensity that reaches at least 60% of the heart rate reserve during pregnancy while gradually increasing physical-activity energy expen-diture is beneficial. To achieve the minimum expenditure of 16 metabolic equivalent task h/wk, one could walk at 2 miles/h for 6.4 h/wk (2.5 metabolic equivalent task-hours, light intensity) or, preferably, exercise on stationary bicycle for 2.7 h/wk (6 to 7 metabolic equivalent task-hours, vigorous intensity). To achieve the target expenditure of 28 metabolic equivalent task-hours per week. One could walk at 2.0 miles/h for 11.2 h/wk (2.5 metabolic equivalent task-hours, light intensity) or, preferably, exercise on stationary bicycle for 4.7 h/wk (6 to 7 metabolic equivalent task-hours, vigorous intensity). More vigorous the exercise requires less total exercise time to achieve metabolic equivalent task hours. Light muscle strengthening performed during the second and third trimesters of pregnancy has minimal effect on new-born body size and overall health.
A prior protocol was written before undertaking the review and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was used to guide reporting (Moher et al., 2009).
Inclusion and exclusion criteria
Quantitative and qualitative studies that looked at physical activity in pregnancy in Africa were included without restrictions on date. Only articles published in English were included. Editorials, letters and commentaries were excluded from the review.
Electronic searches
A comprehensive search of Pubmed, Cinahl and Scopus data bases was conducted using appropriate MeSH terms combined by Boolean commands “AND” and “OR”. Key words in the search strategy included (physical activity OR exercise) AND pregnancy AND Africa. Reference lists of included studies were screened for relevance and hand searching of relevant reports was done. Searches were done from January 2015 to March 2015.
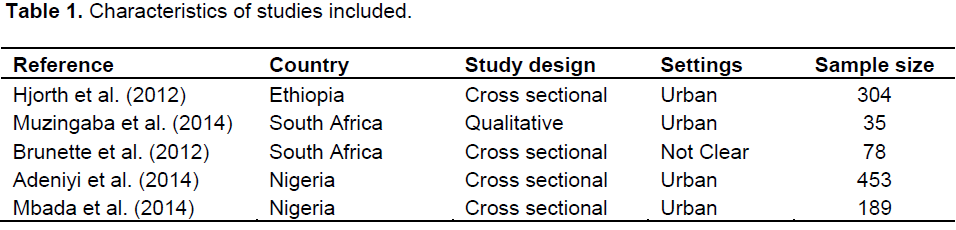
References were managed manually for all the citations retrieved. Two reviewers screened titles and abstracts independently using the exclusions and inclusion criteria. Relevant articles were selected and their full texts were sought. These were then screened by both reviewers for eligibility. Discordance about inclusion of an article was discussed together. A data extraction form was developed incorporating study design, country, sample size and relevant outcomes.
Physical activity status
Nigeria
In a cross sectional survey done by Mbada et al. (2014), to assess knowledge and attitude of Nigerian pregnant women towards antenatal exercise findings revealed that 37% respondents had knowledge of pelvic floor exercise, muscle strengthening exercise 51.3%, back care exercise 51.3% and relaxation and breathing exercise 59.8% as types of antenatal exercise in pregnancy. These findings underscore the importance of education to promote other forms of exercise that can be done without cost in these resources limited setting to promote wellbeing. According to the South African Sports medicine position statement on exercise in pregnancy, exercises such as jogging/ running, hiking, low impact aerobics and dancing are some of the safe exercises that can be done in pregnancy (Barsky et al., 2012). Most of the respondents agreed that exercise in pregnancy would lead to reduction in the risk of back pain (75%), prevention of excess weight gain (69.1%) and increased ability to cope with labour and delivery. Though this is quite true, there are a lot of benefits of exercise that, if made known to pregnant women, will help to promote a good attitude towards exercise in pregnancy and willingness to engage in exercise. Benefits such as prevention or control of gestational diabetes and eclampsia and a general feeling of well-being need to be emphasized. On contraindi-cations of exercise, swelling of lower extremities (31.8%), extreme weight gain or loss (30.7%) and back pain (28.5%) were mentioned. There are quite a number of contraindications to exercise in pregnancy such as restrictive lung disease, incompetent cervix and preterm labour (Barsky et al., 2012). Knowledge of contraindi-cations is very vital to promote safety of the mother and fetus during pregnancy.
In terms of attitude to exercise, only 16% had a negative attitude towards exercise in pregnancy. This gives health care providers an opportunity to utilize exercise as an adjunctive therapy to many health conditions, including gestational diabetes. However safety issues need to be observed to ensure that optimum benefits are reaped from the exercise.
In a survey conducted by Adeniyi et al. (2014) to assess physical activity and energy expenditure in Ibadan pregnant women, about half [222(49.0%)], of the participants were classified as sedentary based on their performance on the Pregnancy Physical Activity Questionnaire (PPAQ). Those who presented a moderate physical activity level were 46 (10.2%) while 40.8% presented within light physical activity level. None of the women could be classified as having vigorous physical activity level. Women expended energy in all the physical activity domains including household, occupational and sports activities though the highest amount of energy in this study was expended on household activities.
South Africa
Brunette et al. (2012) conducts an epidemiological study of physical activity patterns and weight gain in physically active and sedentary pregnant women in Tshwane, South Africa. Of the 78 women who participated, 30.8, 53.9 and 16.7% were classified as relatively inactive, active and very active respectively. In terms of weight gain, 45.5% gained weight within the recommended range, 28.6% gained weight that was below the recommended range while 26.0% gained weight above the recommended range. There was no association, however between the trimester and the level of physical activity. However it has been found in literature that physical activity declines as the pregnancy progresses. These findings could however be due to the small study sample and the cross sectional nature of the design. Physical activity in this study effectively controlled weight gain during pregnancy.
Another study was carried out in South Africa by Muzigaba et al. (2014), to explore the perceived role and influencers of physical activity among pregnant women from low socioeconomic status communities. In terms of physical activity, about 44% reported that they were currently not physically active and of the 56% who reported engaging in physical activity, 44% did light physical activity and 12% did moderate physical activity. All participants were generally aware of physical activity in pregnancy and recognized the importance of being healthy during pregnancy. They mentioned, together with physical activity, good nutrition, safe sex and avoidance of alcohol and tobacco products as healthy lifestyle behaviours.
Ethiopia
Hjorth et al. (2012) conducted a study in Ethiopia to objectively assess level and intensity of movement sensing method was used to measure physical activity. This is the second most objective method of measuring physical activity after the doubly labelled water method. Pregnant women spent a median of 1100 min/day (< 1.5 MET) (76.4%) in sedentary activities namely, eating, sitting, walking, sleeping, resting in bed and cooking. They also spent 303 min/day (1.5 to 3 MET) (21.0%) in light intensity activity and 40 min/day (>3 MET) (2.8%) in moderate to vigorous intensity activity. This falls far below other recommendations made. To achieve the minimum expenditure of 16 metabolic equivalent task h/wk, one could walk at 2 miles/h for 6.4 h/wk (2.5 metabolic equivalent task-hours, light intensity) or preferably, exercise on stationery bicycle for 4.7 h/wk (6 to 7 metabolic equivalent task-hours, vigorous intensity) (Zavorsky and Longo, 2011). In conclusion, physical activity in this study was estimated to be low and the participants would on average physical activity in this study was estimated to be low and the participants would on average be classified as sedentary to light active.
Measurement of physical activity
Only one of the studies done in Africa included in this review employed objective tools in measuring physical activity (Hjorth et al., 2012). Few studies have employed objective methods to record physical activity (Bernstern et al., 2014). The accuracy obtained from use of objective measurement tools is indispensable for establishing valid dose response relationships between physical activity and sedentary behavior on one hand and outcomes for health and disease on the other (Bernstern et al., 2014). Self-reports are used typically in large epidemiological investigations but they lack precision both due to recall error and social desirability bias (Gaston and Cramp, 2011).
Types of physical activity and intensity
Household activities consistently emerged as the major form of physical activity engaged in by pregnant women (Hjorth et al., 2012; Adeniyi et al., 2014). Pregnant women may feel safer and comfortable doing household activities that are outdoor activities (Adeniyi et al., 2014). This is consistent with a study conducted in South Africa whose findings revealed that some women did not feel safe in their neighbourhoods (Muzigaba et al., 2014). Low income pregnant women might not afford outsourcing housekeeping services (Adeniyi et al., 2014). However, household activities may not be adequate to achieve recommended physical activity level (Adeniyi et al., 2014). Aerobic exercise is recommended to maintain cardiovascular fitness and help prevent chronic diseases (Nascimento et al., 2012). Large muscle groups should be involved in exercise such as when walking or jogging, stationery bicycle, treadmill, swimming, water aerobics, aerobic dance or low impact aerobics (RCOG, 2006). Whatever choice of activity a woman makes, it necessary to find a modality of exercise which they stick to over time while avoiding exercises that increase risk of falling and abdominal traumas (RCOG, 2006).
It is very important for pregnant women to be able to measure the intensity of exercise if they are to benefit from it. Ratings of perception exertion can be used to assure an ideal intensity of exertion using a scale rating from 6 to 20 with an ideal target zone for pregnant women of 12 to 14 (somewhat hard) (Artal et al., 2003). However in low income settings these resources might not be available and the “talk test” can be done to confirm that intensity of exercise is adequate and women are not overexerting. The “talk test” enables exercising at comfortable intensity that allows one to keep up a conversation (RCOG, 2006).
Level of physical activity
The level of physical activity reported in the studies from Africa was low (Adeniyi et al., 2014; Hjorth et al., 2012). However women in low income countries are generally considered to have a high physical workload that is sustained throughout pregnancy. There are a few published studies on physical activity among pregnant women in low income countries and most are based on questionnaires. In a meta-analysis of doubly labelled water studies conducted by Dugas et al. (2011) to assess energy expenditure in adults living in developing compared with industrialized countries findings revealed that women from developing countries have similar physical activity levels to those from developed countries. It could therefore be a misconception that women from developing countries have high levels of physical activity considering that physical activity in the studies was measured using the most objective method. Low levels of physical activity have also been reported in the developed world. A study conducted in the United States reported that only 15% of women engaged in physical activity at the recommended level (Evenson et al., 2004). In another study done on health Irish pregnant women only 21.55 women met the current recommendations for exercise in pregnancy (Walsh et al., 2011).
Physical activity tended to decrease as pregnancy progressed in the African studies reviewed (Hjorth et al., 2012, Adeniyi et al., 2014). The risk of being sedentary increase with advancing pregnancy probably because most women are careful to avoid injuries to themselves and the unborn baby and that there is a general distortion of body frame with a backward sway that makes it difficult to perform physical activity (Adeniyi et al., 2014). Even studies conducted in developed countries have reported a declining physical activity level with advancing pregnancy (Guelinckx et al., 2010; Hayes et al., 2012). These findings might mean that low levels of physical activity are prevalent in both developing countries and there is need to promote physical activity even in developing countries.
Factors influencing physical activity
Attitude and knowledge
Only one study by Mbada et al. (2014) looked at knowledge and attitude towards physical activity in pregnancy. Findings revealed that participants had some knowledge about types of exercise and some benefits and contraindications to antenatal exercise. 47.6% had below average knowledge, 5.82% had average know-ledge while 46.6% had good knowledge of antenatal exercises. Almost half of the participants had below average knowledge. This in itself might be a barrier to performance of physical activity during pregnancy.
It also might result in women engaging in activities that increase risk of harm both to the pregnant woman and the unborn baby. It is necessary therefore, to give proper education concerning physical activity in pregnant considering its numerous benefits among which are prevention and control of gestational diabetes. Though 47.6% had below average knowledge of physical activity in pregnancy in this study, only 15.8% had a negative attitude towards physical activity in pregnancy. These findings might underscore the influence of lack of knowledge on exercise in pregnancy because even some of those that had a positive attitude towards exercise in pregnancy.
Although recommended level of physical activity is beneficial, it may not be perceived as appropriate or feasible. Maintaining or increasing physical activity in pregnancy is difficult even in the absence of medical or obstetric complications. Though there is little information on activity levels in pregnancy (McParlin et al., 2010), studies have consistently identified social isolation, safety concerns and cultural norms as barriers to physical activity among an ethnic group of pregnant women (Chasan-Taber, 2012).
In the study conducted by Muzigaba et al. (2014),participants indicated that physical pain, large body size due to pregnancy and lack of energy were barriers to engaging in physical activity during pregnancy. Un-availability of physical activity based facilities at community level and lack of time to exercise due to family work responsibilities were major environmental barrier to physical activity during pregnancy. Similar findings from low income countries in the developed world have been reported in literature. In a study conducted by Groth and Morrison-Beedy (2013) to assess the views of low income, pregnant African American women on physical activity and diet, part of the findings revealed that fatigue was a major barrier to being physically active.
Though the women expressed that being physically active is important during pregnancy, they were not intrinsically motivated to do so. There was also fear that physical activity might be harmful to the baby or the pregnancy if they become too physically active. Strategies to overcome known exercise barriers including fatigue, concern with pregnancy complications, lack of time, lack of social support and weather may need to be in-corporated into weight control interventions in pregnancy (Evenson et al., 2009).
Some women thought that their financial position was an impediment since physical activity requires access to a gymnasium while some were concerned about safety issues in the neighbourhood. Almost all participants in this study reported not being aware of what types of physical activity to do and how much is required. This could also be a barrier to physical activity in pregnancy (Muzigaba et al., 2014). These findings are consistent with findings of a study that reported lack of awareness of importance of exercise. In a study conducted by Kieffer et al. (2002), women believed diabetes was primarily related to heredity and diet but not physical activity during pregnancy or in the post-partum period.
Late booking
Most of the participants in the study reviewed were in either the second or third trimester of pregnancy. This might reflect on a problem of late booking. Physical exercise particularly before pregnancy and in the early stages of pregnancy has been shown to be beneficial in preventing and controlling gestational diabetes mellitus. It is therefore necessary to encourage early booking of pregnancy in order to realize more benefits from physical activity as pregnant women do get contact with health care professionals early that will give appropriate health education.
Based on the findings of this review, the following recommendations were made:
i) Guidelines of physical activity in pregnancy such as the South African guidelines should be used to foster physical activity in pregnant women. A study done in South Africa reported that women were willing to follow a set of guidelines with supervision (Muzigaba et al., 2014). If physical activity is integrated in a routine antenatal care pregnant women are likely to adopt it as a necessity rather than as an option in pregnancy.
ii) Health education on physical activity in pregnancy should be an integral part of antenatal care.
iii) Objective measures of physical activity such as doubly labelled water tests and heart rate monitoring and movement sensing should be utilized in order to come up with generalizable results. Self- reports of physical activity have a weakness of recall and social desirability bias.
iv) Pregnant women should be encouraged to form exercise groups in their communities so they provide moral support for each other. This might also take care of neighborhood safety concerns as raised in a study that was done in South Africa (Muzigaba et al., 2014)
v) Pregnant women should be encouraged to book early for antenatal care in order to reap optimal benefits from physical activity. According to RCOG (2006), women should adhere to a certain modality of effective exercise if it will be beneficial to them. Early booking gives this opportunity of starting early in pregnancy and adhering for a long time.