Full Length Research Paper

ABSTRACT
The study was undertaken to explore the influence of cultural practices on birth experiences of first-generation Nigerian women (FGNW) living in London, with the objective of highlighting factors within emic and etic care that may influence birth outcomes for this population. The study entailed an exploratory, descriptive, contextual and qualitative methodology organised in two stages. Focus group discussions and semi-structured interviews were conducted with self-identifying FGNW with retrospective birth experiences, and eight non-Nigerian and four Nigerian midwives providing maternity care for this population. Second part entailed prospective study of FGNW at three intervals during a birth continuum. Combined epistemologies of culture care and trans-cultural theory were adopted. Thematic and ethno-nursing analytical approaches of identifying, analysing and reporting patterns and themes within the data ensued. Findings indicate that culture exerts a significant influence on birth and maternity care experiences of FGNW as care meanings are embedded in cultural values and beliefs, economics of family and other support networks, diaspora environment, culture of expectations, rituals and taboos, kinship of support, and immigration barriers in their negotiation of maternity care. Conflicts were uncovered between FGNW’s cultural and midwives professional care as aspects of FGNW’s cultural practices warrant preservation, negotiation; re-patterning to ensure continuing perinatal health and wellbeing. Culture Care Midwifery Model is espoused as a model to guide midwives in providing culturally congruent care that will meet the care needs of FGNW and optimise their health and wellbeing through birth continuum.
Key words: Birth, culture, culture care, cultural congruence, emic care, ethno-nursing theory, etic care, family, kinship.
Abbreviation: BAME, Black, Asian and Minority Ethnic group; CEMACH, Confidential Enquiry into Maternal Deaths in the UK; CMACE, Confidential Inquiry into Maternal and Child enquiries; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, 4th Edition; Emic care, folk, traditional/cultural care; Etic care, professional care based on biomedical model of care; FGNW, first-generation Nigerian women. FGNW in the context of this study are women born in Nigeria who migrated to the United Kingdom (UK) and are domiciled in London; ‘igbu ewu ukwu’, celebration of fertility by slaughter of goats at the birth of a tenth and subsequent child/ren in Igbo culture; NICE, National Institute for Health and Care Excellence; Omugwo, specified rest period of about a month to three months of the Igbo’s of Eastern Nigeria which is symbolic and similar to the Chinese ritual of ‘doing the month’; ONS, Office of National Statistics; MBRRACE, Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries across the UK (MBRRACE-UK); MREC, National Health Service Multi-Centre Research Ethics Committees; Mw, midwife; Wm, woman.
INTRODUCTION
Factors that contribute to poor birth outcomes for FGNW in London may be linked to aspects of their cultural emic care practices which has so far not been studied and/or documented. Historical policy documents have highlighted poor outcomes in the birth outcomes of Black, Asian and Minority Ethnic (BAME) populations in the UK (Smith et al., 2019; (MBRRACE-UK), 2014; (CMACE), 2011; (CEMACH), 2007, 2004), attention has not been given to their cultural practices in relation to birth, nor has the influence of such cultural practices been the focus of studies. Blunt (2014) and Smith et al (2019) highlight health inequalities faced by BAME women, resulting in fivefold increased mortality rate for black women in childbirth and 121% increased risk of stillbirth among black babies as compared to their White counterparts. This staggering historical statistics roused the researcher’s interest in exploring potential influences that cultural practices may exert on the reported poor birth outcomes of BAME women including FGNW living in the United Kingdom. Therefore as a British-trained midwife from Nigerian background, she has taken on the task of exploring this matter both from the perspectives of FGNW and midwives; in order to uncover the influence that emic and etic care practices may have on the birth experiences/outcomes of FGNW in London. Amongst this Nigerian population, there are wide ranges of socio-cultural processes decreed by tribal and religious dictates that inform choices/decisions about pregnancy, birth and maternity care.
National Health Service (NHS) trusts are required to understand the needs of their population and to provide care that is culturally sensitive to their local populations (Gil-González et al., 2015; CMACE, 2011; CEMACH, 2007/2004). Furthermore, there has been a flurry of directives over the last decade attempting to highlight and strategize measures for addressing the inequitable cultural care provision in the NHS, to ensure policy context and to highlight implications for care delivery such as Smith et al. (2019), MBRRACE (2014), CMACE (2011), Psoinos et al. (2011), CEMACH (2007, 2004) and NSFs (2007).
This tensions has worsened especially around the notion of ‘Health Tourism’ affecting migrant women seeking maternity care in Britain. Maternity staff are expected to meet the care needs of diverse populations but without a specific care model to guide cultural congruent care delivery. This study is therefore timely to make tangible contribution to understanding of some of the cultural practices that influence care uptake of FGNW and care approaches taken by midwives to meet diverse cultural care needs; by examining perspectives of emic versus etic care perspectives of the study cohorts; and to suggest a care model to inform culturally congruent care for FGNW.
FGNW has a unique identity as a transnational ethnic group in London. To this population, ethnicity may be perceived as both cultural and national identity as both are held in even regard by them. Maalouf (2012) in discussing the increasing complexity of identity asserted that each one of us has two heritages: A vertical one that comes to us from our ancestors, our religious community and our popular traditions, and a horizontal one transmitted to us by our contemporaries and by the age we live in. Therefore various aspects of belief systems and vertical and/or horizontal identity upheld by FGNW in regards to their ethnicity may influence their access of maternity care. Conversely, maternity service care responsiveness to such health beliefs based on identity, and associated emic practices, is necessary in order to achieve congruency in maternity care delivery to this population.
To FGNW, cultural expectations, rites and rituals may serve as a guide and a means of support during pregnancy and birth experiences, and may potentially aid their transition to motherhood. Conversely, unrealistic expectations can be overwhelming and possibly detrimental to their health and wellbeing (Katbamna, 2000). Therefore exploring how FGNW’s emic care practices align with midwives’ etic care provision is vital to ensure culturally congruent care that meets the care needs of this population during birth experiences in London. Towards this end, this research study was undertaken with the following specific objectives:
(i) To explore the cultural (emic) care practices of first-generation Nigerian women during their birth experiences in London.
(ii) To explore first-generation Nigerian women’s retrospective expectations of maternity care in London.
(iii) Examine midwives’ perception of first-generation Nigerian women’s requirements for culturally congruent care in their birth experiences in London.
The study addressed the following research questions:
1). What cultural practices are important to first-generation Nigerian women in their birth experiences in London?
2). What do first-generation Nigerian women expect from maternity care providers to make care culturally congruent?
3). How well were the cultural needs of first-generation Nigerian women with retrospective experiences of birth in London met as compared to their prior experiences of birth in their home country?
4). What do midwives perceive to be the specific expectations and cultural needs of first-generation Nigerian women and to what degree did they feel they met these needs?
The study entails an exploratory, descriptive, contextual and qualitative methodology. As qualitative research aim to enhance understanding of individual perspective (Bowling, 2009: 380), the qualitative paradigm taken in this study will enable the researcher to focus on the meaning FGNW attach to their social world of birth in London while adhering to culturally-informed or learned emic care practices and the midwives understanding of this social world of FGNW in contrast with their etic care approaches and perspectives.
Discord between delivery approaches and care-seeking behaviours can have negative impact both to the care giver and care receiver. Therefore, the need for culturally congruent care that meets the care needs of FGNW during childbirth in London is the driving force that prompted the search for a care model that can enable and inform FGNW and midwives to achieve maternity care that is culturally congruent. As a result, the interrelated theories guiding this study are those of Helman (2007) which explores three different cultural strata of culture expression, Leininger (2002) Culture Care Theory and Papadopoulos et al. (2008) Cultural Competent Care model. Leininger (2002) theory will guide the exploration of the influence of culture on emic care practices of FGNW around pregnancy both in their home country and in London. Papadopoulos et al. (2008) Cultural Competent Care model will guide the exploration of the midwives cultural awareness, cultural knowledge, cultural competence and sensitivity in meeting the cultural care needs of FGNW. In this way, the combined models will be useful in uncovering new knowledge on the influence of emic and etic care approaches on achieving maternity care that is culturally congruent for FGNW as well as to unveil midwives level of cultural competence in meeting the needs of this population.
Defined narrowly, “epistemology is the study of knowledge and justified belief” (Steup, 2014: 1). If knowledge is justified true belief (Steup, 2014: 2), midwives need to have cultural knowledge to understand what FGNW believe about their cultural practices and how what they belief influences their care approaches and care expectations. Similarly, FGNW need to comprehend the philosophy of professional care of midwives in order to accept and access it to meet their maternity care needs. Therefore for knowledge to be justified, there is need to establish what FGNW hold as justified true belief of professional care approaches and the need for accepting and valuing these from midwives, whilst midwives similarly need justified true belief of emic care practices of FGNW in order for both to arrive at a level of understanding that ‘are individually necessary and jointly sufficient for knowledge’ to be gained (Steup, 2014: 2). Exploring the emic birth practices of FGNW and the etic care approaches of midwives offer a powerful and rich source of qualitative data that enhances understanding of emic/etic care approaches.
MATERIALS AND METHODS
The study was planned in two stages. In stage one, an exploratory approach was taken through focus group discussions to obtain views of FGMWs emic care practices from three perspectives: the retrospective perspectives of FGNW with valid experiences of birth in London, and the perspective of Nigerian midwives and non-Nigerian midwives providing maternity care in Local Trusts of the FGNW sample. The rationale for stage 1 of this work was firstly to explore the emic care practices and what FGNW consider relevant in regards to meeting their cultural needs during birth, and also to use focus group with FGNW with retrospective experience of birth as an exploratory step to gain an insight about divergent cultural care practices that informed the prospective study. Similarly, by examining midwives perspectives on FGNW’s emic care practices and the issues this may raise in midwives etic care approaches, a broader understanding of their perception of competency and congruency was ascertained to inform the prospective study.
Stage two of the study entailed obtaining the prospective views of six FGNW women through semi-structured interviews at 3 stages of pregnancy/birth: twenty-four weeks gestation, at six weeks postnatal and at three months postnatal. The purpose was to elicit their prospective emic care practices around pregnancy, birth and postnatal care in order to identify individual and group patterns as well as identify commonalities of cultural practices over the birth continuum. Such exploration enhanced a detailed narrative of women’s experiences, granting an opportunity to understand the wider social context of their birth experiences and to make connection between different areas of their lives as experienced through a continuum of birth. According to Barwell (2009: 49), “a narrative has a tripartite structure with a beginning, a middle and an end”. In this way, interviewing FGNW at the viability of pregnancy (24 weeks gestation), at the middle of birth experience (6 weeks postnatal) and at 3 months post birth gave a structure for capturing their stories of emic care practices at three distinct phases of their childbirth experience. As prospective study is not affected by recall bias (Bowling, 2009), changes in belief and practices of the prospective informants could be picked up at different intervals and analysed to reflect reported changes over time. Such succession in the narration of events does represent events as an intelligible whole (Barwell, 2009).
Semi-structured interviews are a useful data collection tool in qualitative research, as they allow for participants to expand on their individual experiences. By using open-ended questions on the topic guide, informants were given the freedom to bring the distinct understanding that narratives supply to the events they are about (their childbirth practices through a birth continuum). An advantage of this approach is that valuable information can be obtained, providing depth of relevant data (Watson et al., 2008).
Rees (2011) assert that recruiting a manageable sample is favourable in such interview data collection, to facilitate a more in-depth understanding of the researcher’s questions and to provide data-rich information. There were altogether five focus group discussions and eighteen prospective interviews with the recruited sample of 24 informants which provided saturation of categories, patterns and themes that has enriched understanding of how emic care practices of FGNW influence their care access, general health and wellbeing and the congruency of etic maternity care provision of midwives to this population. Saturation of data means that data was collected until redundancy occurred; informants’ shared similar content and the researcher noted recurrence of the same information (Weller and Kinder-Kurlanda, 2016).
Following MREC approval, three NHS Trusts were approached and informed of the researcher’s intention to commence recruitment of the study samples from their catchment area. Following this, all Nigerian women of childbearing age (18 to 50 years), fitting the selection criteria and accessing maternity care at the three NHS Trusts and all midwives working in the same Trusts were granted equal opportunity to participate in the study by individual invitation letters and information leaflets.
Inclusion criteria
The target sample were self-identifying FGNW within childbearing age, with a viable pregnancy and accessing maternity care within three Trusts in South-East London. Midwives were self-identifying Nigerian and non-Nigeria midwifery practitioners interested in the study and working within the three Trusts in South-East London.
Exclusion criteria
These were non-Nigerian women, second and subsequent generation Nigerian women accessing care at the three NHS Trusts, Nigerian women with complicated pregnancies, critically-ill or non-viable pregnancies. No FGNW fitting these categories were encountered during recruitment or at any stage of this study. Mid-wives were only excluded by lack of expressed interest in the study.
Details of focus group interview
The focus group interviews occurred over a total of 9 h in a 3 month period and involved 18 informants, in 5 separate sessions, using 4 venues. The participants were mostly interviewed at convenient locations chosen by them. Six FGNW who took part in the first focus group were women who had retrospective birth experience in London. They took part in the focus group discussion after the researcher gained their full informed written consent. This focus group discussion was interactive and lasted for two hours. The women considered the following topic-guide areas:
1). Explore the cultural practices you adhered to during your childbirth experience in Britain and the presumed benefits and/or constraints of these to your health and wellbeing.
2).What do you consider culturally important for Nigerian women during pregnancy and childbirth?
3). In terms of childbirth practices, what do you consider to be the difference between Nigerian women in Nigeria and FGNW in London?
4).The women were also asked to examine the care they received from midwives in regards to meeting their cultural needs.
5). Topic guide for stage two of the study were also reviewed by this cohort in regards to appropriateness of the tool in addressing pertinent points about pregnancy and childbirth practices of FGNW in the prospective study.
These questions were aimed towards obtaining the retrospective views of the women in regards to what they consider important in their birth experiences, and midwives meeting their cultural needs.
To ascertain the etic perspectives of midwives, 2 separate groups of midwives were recruited from 2 local Trusts within MREC catchment area to ascertain their perception and views of FGNW’s emic care practices around childbirth and the issues that these may cause in providing etic care to this population. The sample constituted of 8 non-Nigerian midwives located in one Trust and 4 Nigerian midwives located in another Trust by mere co-incidence. In this way, a total of 12 midwives consented to take part in the focus group discussion. According to Kumar (2019), in qualitative research the sample size does not have any significant role, and Aveyard (2010) conveyed that a small sample is appropriate in qualitative research to enhance in-depth understanding of phenomena from information-rich informants.
An eleven-point topic guide specifically designed by the researcher to elicit information from the midwives and approved by MREC for this study was used for the focus group discussions with midwives. Polit et al. (2001) affirm that topic guides enable discussants to tell their own story in narrative or conversational form. Use of open-ended questions was instrumental in obtaining specific in-depth information (Bowling, 2009) from midwives on their perspectives on FGNW’s emic care practices and the meanings given to these practices by midwives in regards to providing congruent etic care to FGNW. Data generated from all angles of focus group discussions were to inform the prospective study through comparison of emergent characteristics of emic practices of FGNW as perceived by them and by midwives.
For stage two of this study, 30 FGNW in early stages of pregnancy were approached at booking and invited to take part in the prospective study, which was to take place at twenty-four weeks gestation, six weeks postnatal and three months postnatal. Seven women consented but one withdrew her consent within a day of consenting, for personal reasons not explained to the researcher, leaving six women as the sample population for the prospective study.
During the prospective discussions that took place in the women’s homes, the emphasis was on gathering narratives and understanding of the cultural practices of each participant woman during current pregnancy and childbirth experience in their most convenient environs. Elwood and Martin (2000) argue that location influences information that is communicated in research interviews as well as the power dynamics of the interview. They contend that participants given a choice of the location/venue of research interview feel more empowered in their interaction with the researcher.
Audio recording was used for gathering interview data. Video recording was used as an aide memoir to allow integration of audio, visual interaction and environmental material and to bring significance to events during data gathering. This move proved beneficial as exaggerated gestures inform expression of narratives amongst Nigerians.
Ethical considerations
According to Cluett and Bluff (2006), ethics in research can be considered the degree to which the researcher conforms to moral standards in relation to legal, professional and social accountability. As per robust researcher processes, ethics approval was sought from Multi-Centre Research Ethics Committee (MREC) which has a dual duty of protecting the rights, safety, dignity and well-being of research participants; and facilitating and promoting ethical research ethos that is of potential benefit to participants, science and society. In line with this, approval and official recognition of this study (MREC ref: 08/H0810/66) was gained. Ethical considerations also include confidentiality, informed consent, voluntary participation, and protection of participants against potential physical or emotional harm, observing Data Protection Act (1998), un-coerced participation and/or withdrawal, and keeping to ethical principle of beneficence (balancing benefits, costs and risks of research) and non-maleficence (doing no harm) to the participants (Cluett and Bluff, 2006). This also included arranging debriefing services for participants in regards to any potential psychological issues that may arise from partaking in this study. At the end of the study, the service of the counsellors were not deployed as none of the participants highlighted any emotional/psychological effect from participation in the study.
Data analysis
Through a thematic analytical approach utilising Braun and Clarke (2006) model, informed by Leininger (2002) phases of data analysis and qualitative framework, concepts have been drawn from transcribed data generated through focus group interviews and prospective interviews to formulate categories through which over-arching themes are devised.
The researcher having personally obtained the data via interactive means, some immersion with the data occurred during data gathering and transcription to have familiarity with the depth and breadth of the content. One therefore started transcribing with prior knowledge of the data and with some initial analytic interests or deliberation through memos (self-reflection on the data gathering exercise). Transcribing was an excellent way to get to grips with data breakdown as it aided the creation of meanings to the data generated by interviews. Analysis of the various audio recordings (backed with video recording) of the interviews involved detailed scrutiny of particular fragments to illuminate meaning of participant’s verbal and non-verbal expressions. In this way, analytical approaches aided the deconstruction of assumptions and fostered understanding of the meaning of these experiences for the informants. The researcher adopted a rigorous orthographic verbatim transcript account of all verbal and relevant non-verbal cues/gestures recorded during data gathering and highlighted interesting categories of the data as she transcribed.
Inductive analysis approach entails coding data without trying to fit it into a pre-existing coding frame or one’s analytic preconception, and hence averts the bias of pre-supposition. Semantic approach enabled the researcher to identify themes within the explicit or surface meaning of the data (Braun and Clarke, 2006) without going beyond what the participants have said or what has been written about cultural practices in childbirth. In this regards, Bowling (2014) suggest that verbatim recording and transcription are essential for gathering data to ensure meaning is not distorted or lost. This entailed recording reflective notes about what one was learning from the data (Hussein, 2009), gathered and transcribed as the discussions progressed. This is encouraged by Braun and Clarke (2006) and Leininger and McFarland (2006) as a measure to ensure engagement with the data.
The concepts drawn from each interview represent each informant’s experience, while the categories are the representation of the dominant features of the entire group of informants’ experiences. The collation of these into over-arching themes enhanced the representation of the collective voices of FGNW and midwives about childbirth emic practices and maternity care experiences of FGNW. Themes are derived from analysis and synthesis of both focus group and prospective study data and then confirmed with informants for accurate representation and meaning. Member checking also formed part meaning making of data.
Interpretation is central to qualitative and trans-cultural research studies (Kincheloe and McLaren, 2005; Leininger, 2006a). The adoption of an interpretative stance in examining data renders a sense of the lived experiences of FGNW’s emic childbirth practices and midwives etic perspectives and the influence of these on the birth experiences of FGNW. Discussion and triangulation of study findings with existing knowledge enabled meaningful interpretation by researcher. According to Bowling (2014) researchers use triangulation to increase their in-depth understanding of the phenomenon under investigation by combining multiple methods and theories. Through triangulation, convergence is sought among multiple and different sources of information from which the theoretical framework was formulated and data generated in the formulation of themes or categories.
According to Bryman (2004), different theories help researchers to see problems at hand using multiple lenses. In theoretical triangulation, both related and/or competing theories may be utilised in formulating hypotheses for providing broader and deeper understanding of research problems. Data analysis triangulation, on the other hand, entails using more than two methods of analysing the same set of data for validation purposes (Bryman, 2004; Hussein, 2009). Combinations of Culture Care Theory, transcultural care approaches of Leininger and Papadopoulos and review of existing knowledge formed the triangulation of theory and methods that validates this study. This approach is taken to enrich the research process by enhancing completeness of views rather than confirming findings (Adami and Kiger, 2005). Affirmation of interpretation through member checking aids validity and extrapolation of knowledge from the experiences reported.
RESULTS AND DISCUSSION
The ages of the FGNW ranged from 25 to 34 years with mean age of 30 years. The age range of 25 to 34 years of this population is dissimilar to that reported by Ukwuani and Suchindram (2003) for Nigerian women in Nigeria, where 39.2% of mothers in their study gave birth at younger ages (<25 years) while about 14% gave birth in older ages (35-49 years). According to World Health Organisation survey in 2003, 4.3% of Nigerian women aged between 15-19 years were pregnant with their first child.
The same report indicated that at sub-regional level, a higher proportion of teenage pregnancies were found in women residing in the North East and North West areas of Nigeria (WHO, 2013). The age range in this study depicts the current reproductive trend for non-UK born women in Britain, were the 25 to 34 age group had the largest percentage of births with proportionally fewer births to non-UK born mothers aged less than 25 years in 2011 (ONS, 2009; 2012; Zumpe et al., 2012). This change in reproductive pattern between FGNW in London and their counterparts in Nigerian could indicate acculturation by FGNW in London, in choosing to reproduce in similar age ranges to the women in their domicile country (UK) as opposed to their Nigerian domiciled counterparts.
The status of the informants ranged from unemployed student to medical doctor and lawyer. They were all educated to Higher Education level (Diploma to Bachelor degree). Interestingly, they were all self-identified married women supported by their respective husbands. WHO (2012) in their report on the demographics of Nigeria highlighted that, the proportion of married respondents in North West Nigeria was (94.6%) in the 25 to 34 age group and the proportion of respondents who ever attended school in North West Nigeria was (32.7%). Sadly, the educated figure for Eastern and Southern Nigeria from which the sample of the current study originate were not given in the said WHO report. These reported demographics differ from those of this study, as most were educated, middle class and Christian.
The tribes represented were an even mix of Igbos and Yoruba’s with parity of zero to two children respectively. Although efforts were made to recruit women representing all Nigerian regions living in London, the population of this study were predominantly South-Eastern and Western Nigerians of Igbo and Yoruba tribes in even proportions. Further obstacle to recruiting women from Northern Nigeria emanate from Nigerian migration history. Intrinsically, postcolonial conflicts influence the migration patterns in Nigeria. The Nigerian-Biafran war created massive movement of Nigerians across the world. South-eastern professionals, students, job seekers, women and children were among those who left the country due to political instability and insecurity and mostly settled in parts of the Western world. Nigerian Northerners rarely migrate internationally as they still hold the financial and political power strings of the nation (Cross et al., 2006). This resulted in the lack of representation of Northern Nigerian women in this study.
Over-arching themes
Some of these themes have been merged according to their similarity to arrive at over-arching themes that sum up the perceptions of midwives and FGNW and to answer the research question. Six over-arching themes were drawn as follows (Figure 1):
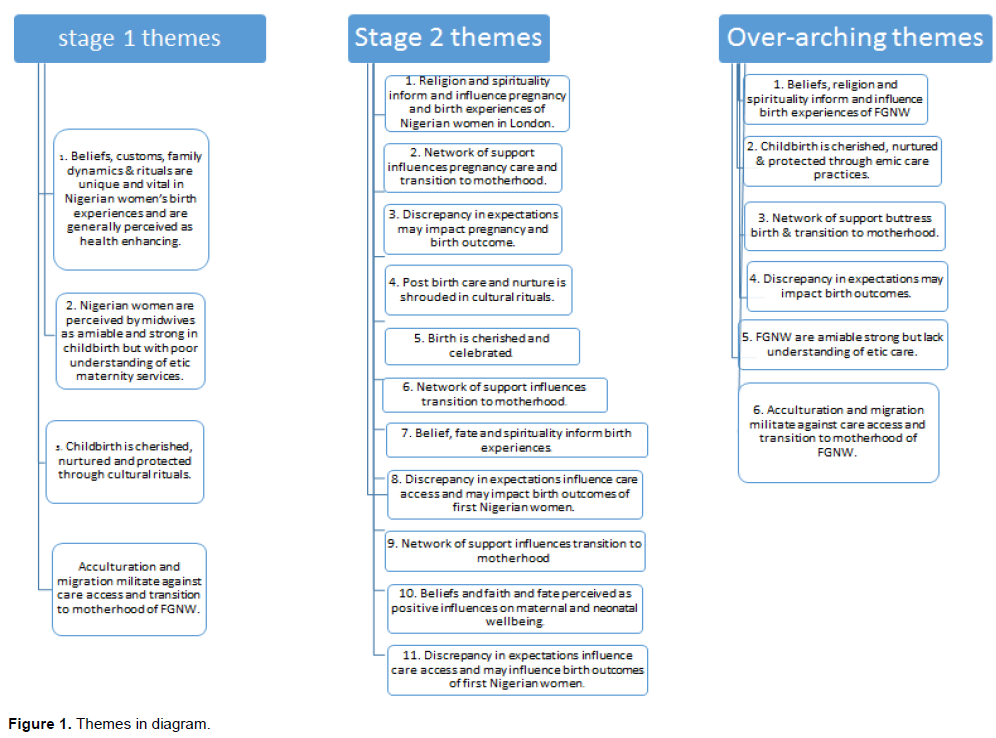
(i) Beliefs, religion and spirituality inform and influence birth experiences of FGNW.
(ii) Amongst FGNW, Childbirth is cherished, nurtured and protected through emic care practices.
(iiii) Network of support buttress birth and transition to motherhood of FGNW giving birth in London.
(iv) Discrepancy in expectations may impact birth experiences and birth outcomes of FGNW in London.
(v) FGNW are amiable and strong but lack understanding of etic care.
(vi) Acculturation and migration militate against care access and transition to motherhood of FGNW in London.
These themes will be critically discussed in triangulation with evidence from contemporary literature to emerge with new knowledge of how culture influences the birth experiences of FGNW in London. Comments by FGNW informants from focus group are denoted as FGN wm 1, 2, etcetera and comments by FGNW prospective informants are labelled as cases: C1, C2 etcetera, while midwife informants are identified as mw1, mw2, and etcetera. NHS Trusts of the midwifery informants are denoted numerically as H1 and H2 etcetera to enhance anonymity.
Theme one: Beliefs, religion and spirituality inform and influence birth experiences of FGNW
From data generated from interviews, it would appear that religious belief in God’s will, are constructs that are believed by FGNW to foster wellbeing. This population of Nigerian women in maintaining spiritual beliefs, customs and rituals appear to uphold these traditional measures to ensure healthy pregnancy and birth. On the matter of belief and faith of FGNW, one Caucasian and one Nigerian midwife commented:
“I find that they are much more faith orientated you know; if God is giving you a child that something is wrong with, then God is giving it to you and it’s His will whether that child lives or dies. The one lady that had the child that had hydrocephalus, she really did not want any invasive test. She was against having (emphasized) a foeticide. …It really hurt her to make those decisions. You know as far as God was concerned; it troubled her immensely. If I tell parents that they’re both sickle cell carriers; they will not go for an invasive test. They will say: no, we will take what we are given; ...and that I think is a marked cultural difference” (H1, mw 4).
Some of these quotes from midwives highlight and affirm FGNW’s adherence to spirituality through belief in God’s intervention in their birth experiences and outcomes. There appear to be a strong acceptance of the will of God in the expression, “what we are given”, and ‘rebuking’ unwarranted potential outcomes which they consider to be outside the will of God for them.
Evidence from literature review and all angles of this study affirm that holding religious beliefs, faith and superstition is integral in the life of most Nigerians at home and abroad. Nadeem et al. (2008) in their study reported that women from minority ethnic groups in Britain were more likely to endorse faith-based solutions to health problems compared to their counterparts from the United States of America. At times, this can be perceived as having a somewhat dichotomous construct of positive and negative spiritual sides (Mitchell and Baker, 2000). A Nigerian researcher Izugbara et al. (2005) assents this later view by asserting that there is also a strong belief in supernatural mystical causes of disease and ill-health amongst some Nigerians. Where, on the one hand, religion and faith aids the acceptance and resolution of certain unpleasant life experiences and aids psychological balance, on the other hand, there seems to be a degree of delusion in respect of faith. The following quotes from midwifery informants go some way to confirm this notion:
“…in labour, you know to give them room because the pastor might come in the middle of it all to pray. So you need to allow for that. There’s gonna be oh! My pastor is on the way and there’s a lot of that, a lot of prayers on the floor, ringing back home, and mother’s praying, father’s praying….” (H2, mw 1).
“Some of them pray on the baby. Muslims, they pray immediately (sic: after birth) before the baby is bathed’ (H2, mw 4).
Such belief is not limited to FGNW. Callister and Khalaf (2010) study of Ecuadorian women’s childbirth experiences found that a strong reliance on God, and spiritual beliefs were vital for transcending the physical pain and challenges associated with giving birth. Most of the women in the study resonated with the idea that childbirth is a time when spirituality was enhanced.
Concomitantly, extracts from Nigerian midwives in this study portray a resounding consensus on FGNW’s need for respecting culture and upholding certain cultural practices that they perceived as enhancing the health and wellbeing of mother and baby. These cultural belief systems tend to resemble those upheld by their counter-parts living in Nigeria and experiencing birth there; which go further to affirm the view that emic care practices related to childbearing and socialisation are among the most difficult to change (Muscardino et al., 2006).
Theme 2: Childbirth is cherished, nurtured and protected through emic care practices
It would appear that amongst FGNW, pregnancy and birth are nurtured through care and attention to healthy nutrition for the pregnant woman and through other emic care approaches geared towards ensuring the wellbeing of both mother and baby. Both midwives and FGMW expressed that a good deal of attention goes into provision of appropriate nutrition for the pregnant mother and providing restorative nutritious therapy for the new mother to ensure that she regains her vitality and physique as fully and as quickly as possible after the strain and stresses of pregnancy and birth. In parallel, there is congruence in FGNW’s desire for healthy nourishment and the midwives promotion of healthy nutrition in pregnancy. Amongst FGNW, this tradition of nourishing a new mother appear to be upheld with a measure of ritualistic significance orchestrated via the Omugwo ceremony (were rest and recuperation is maintained over a given period of about a month to three months with female relatives taking care of the new mother). The following extract from midwives practicing in two different NHS Trusts would seem to confirm FGNW’s endeavour to maintain healthy nutrition during pregnancy and childbirth:
“They eat well (H1, mw 7)....... They don’t take to hospital food because they believe hospital food is not nourishing enough. “They (family) cook vegetable soup, particularly for her, cos they believe the food will produce a lot of haemoglobin to make you fit and to be able to look after your baby” (H2, mw 4).
On the contrary, one of the Nigerian midwifery informants held a divergent view of the nutritional intake of FGNW, highlighting that the diet of FGNW may actually be unbalanced and unhealthy; as demonstrated by her comment below:
“I find that the belief that the Nigerian women have about diet in pregnancy is completely different to what we would advise as professionals. In Nigerian women having high carbohydrate diet is the norm’ (H2, mw 1).
Having high carbohydrate diet by Nigerian women could be as a result of food taboos that abound in traditional instructions to pregnant and recently delivered FGNW. In parts of Nigeria, cultural food proscriptions discourage pregnant women from eating some fruits, vegetables, rice and other high-calorie foods that enrich and nourish the body and avert malnourishment and susceptibility to disease. The general belief is that such foods would negatively affect the childbearing process, as well as affect the health and life of the mother and/or baby. In reality, most of these prescriptions and proscriptions are given in order to sustain the myth surrounding a particular tradition or to emphasise the sacredness of a custom conceived as inviolable (Nwokocha, 2007). Countering such cultural adherence warrants advocacy and robust nutritional advice via effective professional nutrition ad-vice and health promotion to counter ill-informed beliefs.
Theme 3: Network of support appear to buttress birth and transition to motherhood of FGNW in London
Strong network of support enhances the birth experiences of FGNW in London. Some midwifery informants positively evaluated how FGNW are celebrated and nurtured in their birth experiences in London:
“... I think we have a lot to learn from Nigerian women about looking after women that are pregnant and women that ‘have recently delivered…by the idea of actually being looked after which is rather nice” (H1, mw 4).
“So you don’t tend to see a Nigerian woman labouring on her own... It could be a neighbour or a friend that could be there to be with her” (H2, mw 3).
There is also a wonderful Church community that they consider as part of their family as well. So they are supported very much there’ (H1, mw 3).
As established in literature review (Dike, 2013), amongst this Nigerian childbearing population, the family (nuclear and extended) are expected to provide emotional and material support at every stage of the pregnancy and birth continuum. The following quotes from FGNW interviewed express the level of the network of support available to FGNW during birth:
“it’s the culture that when a woman has a baby, if the mother is alive the mother have to go and look after her. In my culture they call it Omugwo, so the mother always comes for Omugwo...’, “when my mummy was here, she was even doing all the care for the baby. I was just looking. And she was even doing all the cooking and the cleaning of the house” (C5).
Oates et al. (2004) point to the benefits of such network of support (omugwo) as protective and the best cure for some of the emotional and psychological ills of childbirth amongst trans-cultural women. In Morhason et al (2009) study about the attitudes and preferences of Nigerian antenatal women to social support during labour, reported that 80.2% of Nigerian women desired emotional support from their partners while about 18 and 7% desired spiritual and physical support respectively. They reiterated the benefits of social support in improving the outcome for both the mother and baby. Social support has also been reported as the ‘catalyst for early breastfeeding initiation for first-time Nigerian mothers’ (Morhason et al., 2009). Similarly, the midwife informants concurred with Morhason’s assertion by reporting that FGNW in their care found breast feeding easy, even for first-time mothers. According to the reports of a randomised controlled trial of the effect of psychosocial support in labour by Morhason et al. (2009), the median time of breastfeeding initiation was significantly longer in supported women than in their counterparts who had no companion and therefore were un-supported throughout labour and delivery. The network of support available to FGNW during birth experiences in London could influence duration and patterns of their breast-feeding habits, as the Nigerian women from this study who had support expressed intention to want to continue breasting beyond the period of the study. This is in congruence with UNICEF Baby Friendly initiative (2012) of encouraging breastfeeding for at least the first six months of a baby’s life. One FGNW spoke of the assistance of her husband as part of the replacement support network while giving birth in London:
“He (husband) did more than I did because ….I don’t have any parents too, which is something. So, he did everything. You do get more support from them” (FGN wm 3).
Where reference is made to the husband’s absence (FGN wm 3), a replacement network of support in the way of sister-in-law’s, friends or church members appear to be arranged to ensure that support is gained, as portrayed in the next quote by a FGNW:
“I am pregnant and they have this way of reaching out to me.....there’s this exceptional service” (C2), “I have a couple of Nigerian friends...they really help me; they have been consistent in bringing me food so that I don’t have to cook”.(C2) “mother in-law comes to stay for first six months for Omugwo ceremony” (C1).
“... where you live in urban area, probably you just have the house maid and your mother but very few people coming around to see you and all the rest” (C5). “There’s no harm in it, you know that pampering yes, it’s an advantage so you tend to... cos if you are left all by yourself: nobody around, nobody helping, you tend to be unhappy: having a baby is a joyous time and it’s a time that brings family, friends and everyone together” (C6).
This general pattern of accessing social and economic resources through networks of support grounded in ties to kin and community appear characteristic across the Nigerian ethnic spectrum (Smith and Firth 2011). A notion previously reported in literature by Morhason-Bello et al. (2009) who reported that most of the women (7 in 10) in their study who were mostly professionals (as per the sample of this study) were willing to pay extra to have a professional source of support, such as a doula. Social support has been defined as access to and use of individuals, groups or organisations in dealing with life’s vicissitudes (Pearlin, 1989). Ohaeri (1998) assents that the lack of an organized social welfare system in Nigeria places a burden of care on the extended family, hence perpetuating this cognisance of kinship at home in Nigeria or abroad, especially in times of need; such as during birth.
The Omugwu ceremony has also been explored by FGNW as part of the reason for the network of support to ensure rest and recuperation from birth and was positively endorsed in the literature review and further endorsed by some of the midwifery informants in the current study as portrayed in the following extracts:
“if I have a Nigerian lady there, she will explain to me that her aunt or her mum is flying over from home … she’s looking forward to them coming because they’re going to do all these things that’s going to be great and wonderful” (H1, mw 2).
“I get the impression as well…that the aunties and mums are coming and that they will help ...and the new mum just breastfeeds…” (H1, mw 4).
This network of support holds the key to recovery and recuperation from childbirth for most (if not all FGNW) as believed by Nigerian women at home and abroad, and affirmed by midwifery informants. Care and support is often anticipated with great excitement, as women look forward to being pampered by family, extended relatives and friends. Evidence from literature (Oates, 2004, Morhason et al., 2009) affirms the benefits of such support networks for Nigerian women. Anugwom (2007) has highlighted the benefits of the Omugwo ceremony in the Eastern parts of Nigeria, where the newly delivered mother receives assistance from her own mother, her elder sisters or her-sisters-in-law who takes care of the household chores and of the entire family’s physical care for a period of six weeks to six months. During the Omugwo, mothers follow a special diet in order to restore energy, promote breast milk production, and facilitate healing from childbirth. The Omugwo practice has been elaborately studied and described by Anugwom (2007) in a book published by Liamputtong (2007) and titled ‘Childrearing and infant care issues: a cross-cultural perspective.
At times there seems to be a separation between level of support and total loneliness and isolation for some FGNW who are recently arrived to Britain and are yet to establish a network of friends or to form this adapted kinship, as expressed by C6 in the earlier quote from FGNW. This measure is taken to formulate or replace absent kinship resulting from immigration. However, not all FGNW manage to obtain support from this form of adapted kinship.
Theme 4: Discrepancy in expectations may impact pregnancy and birth outcomes for FGNW in London
The midwifery informants in this study expressed some discrepancy in the expectations on FGNW by family and high self- expectations in pregnancy and birth that may compound the childbirth experience and impact professional care delivery:
“They’re expected to labour with no pain relief during labour. That makes them a proper woman. I think its honour. The family as well, will be very proud of them if they see they’ve laboured, no caesarean section, normal delivery. “Some people are stressed because not a lot of them like these cultural beliefs. They don’t want to do it but because they are forced into doing it, by their, maybe mother, grand parent, may be mother-in-law and everything” (H2, midwife 4).
Some of the expressed views on family expectations have great implications both for family dynamics and for demonstrations of power (on the part of FGNW’s family) and powerlessness (on the part of FGNW). Nevertheless, in a culture where respect for age, especially of older relatives, is culturally instilled from cradle; and where some degree of subservience forms part of cultural norms, this may have overwhelming impact on care expectations and delivery. In similar vein, in such culture, dignity and honour become highly priced assets that guarantee security and reciprocity of support within the family, but fall out of line with what is achievable within professional care.
The family dynamic intricacies interwoven in decision-making processes of Nigerians form part of their emic belief that merits an entire thesis, and therefore is better left for such an opportunity. As alluded to earlier, these family dynamic intricacies are linked to demonstration of power, subservience and respect for age and the ultimate reward of being cared for by those one shows respect to. Such intricacies give rise to high expectations of the woman and hence compound her ability to make the right choices in her care. Furthermore, it places the woman in a precarious dichotomy of pleasing her family and/or the health care provider(s) instead of herself. This situation can compound FGNW’s autonomy and induce a degree of powerlessness that compounds self-efficacy and can hamper their independence as individuals in their own right. Moreover, as migrants, there is pressure on FGNW to please the extended family by proving their womanhood through natural birth. These cultural dictates may have grave implications not just for FGNW giving birth in London but for their counterparts in Nigeria and in the diaspora, in terms of delay in action in the face of apparent clinical complications that can endanger the life of the mother and/or her baby. Equally, it is an irony for healthcare professionals in London who have the interest and wellbeing of the mother and baby to uphold, to be confronted with such abject complex culturally-imposed resistance against warranted medical intervention.
Theme 5: Midwives perceive FGNW as amiable and strong but lacking in understanding of etic care
Evidence from this study suggest that FGNW tend to present late for antenatal booking and antenatal care according to the midwife informants, FGNW themselves and evidence from literature review. Adewuye et al. (2007: 20) report that, most African women register for antenatal care quite late in pregnancy, making early detection of fetal problems difficult”. This is contrary to NICE (2006) recommendation that pregnant women in Britain should book for maternity care within the first ten weeks of pregnancy. The following extracts from midwifery informants from the focus group discussions highlight aspects of poor care access demonstrable in late booking, poor attendance and poor compliance by some FGNW in London:
“I’ve actually noticed that which is very common among Nigerian women, is their antenatal care is quite poor. You know it is in their DNA’s; they don’t take things serious at all. First of all they don’t want to come to antenatal clinic care (a) they like coming late because they believe they have to leave it till late. That’s something to do with their cultural beliefs” (H2, mw 2).
“Nigerian women book the latest. One was a lady who presented at 28 weeks gestation with a hydrocephalic child. We’ve had a mother again that came in very late who again had extremely blood pressure, ended up with a Caesarean section… I’m not sure if she wasn’t one of our maternal deaths” (H1, mw 2).
Some of these assertions by midwifery informants affirm Aquino et al. (2015) findings that lack of understanding of etic care and conflict between women and midwives care approaches and expectations. Similarly, Raine et al. (2010) upon uncovering that poor interaction between women and midwives had negative impact on care access, recommended that a different ‘interaction style be taken by midwives to improve communication in a manner that may positively influence care access by women.
Inadvertently, late booking and poor care access could influence birth outcomes for FGNW in London and may result in poor pregnancy and birth experiences as evidenced by the assertions of these midwifery informants. MBRRACE (2019/2014), CMACE (2011) and Bharj and Salway (2008) highlighted poor birth outcomes for migrants in Britain compared to their white counterparts. This may be attributable to poor care access, poor compliance and poor understanding of the healthcare system common amongst this population. The midwifery informant did not explain the reason behind FGNW’s late booking for maternity care. However, two FGNW in the prospective study explained the superstition behind their late booking in the following comments:
“Some go into hiding when they are pregnant….”. (C1) “I had to hide the pregnancy until it was no more to be hidden so as to avert ‘evil forces / evil eye and bewitching” (C5).
Taking cues from these expressions, convoluted reasons are implicated as factors influencing FGNW’s late booking for antenatal care. These multi-factorial reasons are particularly linked with social factors and bear spiritual associations for them. The interplay of the notion of evil eye with late booking and poor antenatal care attendance warrant further exploration as it has potential for negatively influencing FGNW’s maternity care outcomes and midwifery care delivery. FGNW’s social situation in their home country is fraught with poor maternity care provision compounded by high morbidity and mortality, and hence compels many pregnant Nigerian women to conceal their pregnancy in a bid to protect themselves and their babies from negative forces (‘evil eye’); believed capable of causing miscarriage. Some FGNW seek maternity care abroad believing this to be safe and more efficient. It is often on the backdrop of seeking free maternity care abroad, late presentation for care and late booking that FGNW have been labelled ‘Health Tourists’ (CMACE 2011). Even as ‘health tourists, difficult visa processes in their home country may contribute to delays in arriving UK to seek maternity care. Furthermore, they may have to work late into their pregnancies to raise the funds for this journey as highlighted by the FGNW informant (C5), who spoke about her personal experience in regards to her personal experience of booking late for maternity care.
Conversely, the reason for late booking may simply be elitist or political, where affluent and rich FGNW mistrust the poorly resourced healthcare services in Nigeria and would fly out to any foreign destination other than Nigeria to seek safe medical care; in a bid to avert risking death in a Nigerian setting. It is the researcher’s observation that there is also the misperception among some Nigerians that childbirth in London and/or America grants the child foreign citizenship that paves the way for a better future not just for the child but also for the entire family and extended relatives. Even so, in travelling to Britain, some women can avert the cost of maternity care in Nigeria. Concomitantly, there are also immigration issues that hamper care access and timely booking such as fear of deportation as highlighted in the following extract by a Nigerian midwife:
“I think majority of them, in this area as well, I’ve found, they don’t access health care because they don’t want to: one they don’t have papers, there’s the fear of deportation, and they don’t know how the system works. You have to constantly remind them of that… “we’re just here to make sure you and the baby are fine”. I’m not gonna pick up the phone and go (sic: to police): “oh she’s here, she doesn’t have papers, come and arrest her. So tell us what we need to know to look after you and this baby” (H2, mw 1).
The annotated expression by this midwifery informant highlights her concerns over the poor care access of a FGNW in London. The statement also portrays concerns over the impacts of poor care access on FGNW’s pregnancy and birth outcomes. Midwifery staff serving this population should examine further the core factors associated with this apparent poor care access by FGNW. Some of the reasons has been highlighted in existing literature. A study examining access to maternity care (DH, 2005) found that user’s ability to access maternity services was heavily influenced by their ability to embrace their pregnancy, their understanding of the role and value of the services and cultural relevance, fear of discrimination, fear of referral to social services or immigration agencies, language difficulties and misconceptions about eligibility for care.
CEMACH (2007) emphasises that maternity service providers should ensure that antenatal services are accessible and welcoming so that all women, can be reached easily and earlier in their pregnancies. An earlier study by Harris (2006) also suggested that locating services at accessible venues might promote and improve access to care. Individualization and continuity of care has also been highlighted as improving care access through establishment of rapport between the woman and the midwife (Sandall et al., 2009). Moscardino et al. (2006) claim that individuals with relatively easy access to healthcare may be more likely to adopt the childrearing beliefs of the host community compared to those with limited access. In this way, easy maternity care access may enhance positive birth outcomes and enhance acculturation of FGNW to maternity services in London.
Nonetheless, when inherent superstitious beliefs like the notion of ‘evil eye’, is compounded by social factors such as those expressed in the last quotes; it becomes clearer while some women may present late for antenatal care. Proactive strategies by maternity care professionals are vital to combat such strongly held mythical beliefs that may hinder care access and impact birth outcomes of FGNW. Equally, maternity care providers may need to address social factors hindering care access through effective health promotion and health education measures. More innovative strategies such as reaching FGNW in community settings such as in Churches, may need to be employed to encourage FGNW to attend educational sessions such as parenthood education to dispel some of the myths that prevent them from presenting for antenatal care in a timely manner.
Midwifery informants also explored other social factors affecting prompt care access amongst FGNW such as those expressed in the following quote:
“I have to say they haven’t got good time management skills…but I wonder if it’s cultural” (H1, mw 7).
The notion of ‘African time’ was explored during the focus group discussion where it arose among FGNW. Umez (2010) coined the notion of ‘African time’: this idea of lateness as selective punctuality /commitment where lateness to appointments and events are culturally accepted amongst Nigerians at home and abroad. The researcher pointed out the habitual and perpetual tardiness of time management of some Nigerians in their home country and even while abroad. The notion is that some Nigerians will deliberately turn up for appointments or events several hours behind schedule and do not perceive this as poor time keeping. This poor time-keeping behaviour can be in the least frustrating for health care providers and at worst, ostracise FGNW from their care providers who may be ignorant of or non-accepting of the notion of ‘African time’.
Furthermore, discrepancy in communication abilities of FGNW with healthcare professionals may affect care planning, care delivery and outcomes. English is Nigerian’s official language and the language of business, exchange and transactions amongst Nigerians at home and in the diaspora, as most Nigerians acquired basic education and many in the diaspora originate from elite and privileged background in their nation. Those Nigerians not in command of the English language would benefit from professional interpretation service to make meaning of new care approaches in the UK. MacFarlen et al. (2009) assent with the later assertion as they highlight that FGNW accessing maternity care in Ireland prefer the use of professional, trained interpreters in general practice consultations. For FGNW, the use of informal interpreters can be inadequate and problematic and can leave them worried, frustrated and anxious of experiences of error and misinterpretation of diagnosis and treatments. This situation may further hamper the provision of efficient maternity care for some FGNW who were reported to have language barriers mostly related to accent/intonation. Issues around some of the cultural beliefs and emic care practices of FGNW highlighted herein, alongside unfavourable mannerisms and approaches of some FGNW to their caregivers could strain relations between them and maternity care providers. Both parties should avoid this situation arising as it could affect efficient care delivery and impact birth outcome of FGNW.
Theme 6: Acculturation and migration militate against care access and transition to motherhood of first-generation Nigerian women in London
Evidence from this study indicates that acculturation and immigration issues militate against care access and positive transition to motherhood in FGNW’s birth experiences in London. Immigration restrictions compounded by high demands of nuclear and extended families may perpetuate FGNW’s strivings to autonomy and independence while in Britain. The midwives commented on FGNW tenacity and hardworking ethos as part of their striving towards self-actualization when this may stem from family expectations and the pressure for success that is common amongst immigrant populations in diaspora (Jiménez and Horowitza, 2013). FGNW’s drive to self-actualization in the face of apparent obstacles and difficulties imposed by high family expectations and their host environment in Britain seems to mitigate and enhance their adaptation to work ethic of their host nation, a view expressed by some midwifery informants:
“A lot of them are working, and will work up to quite late into their pregnancy…. (H1 mw 2). They work almost the last log and they’re busy looking after children, and have got a lot of children”. (H1, mw 4)
The midwifery informants in this study expressed that FGNW seem to get on with pregnancy as a normal life event and tend to juggle it with other life demands. Even so, the midwives highlight the expectation of family on this population to juggle pregnancy with life aspirations. This precarious dichotomy between desire to self-actualize and to fulfil family expectations has the potential for compromising the health and wellbeing of FGNW giving birth in London, and can compound positive transition to motherhood. Some of the following extracts from the focus group discussion portray the determination of FGNW to succeed in Britain:
“The average Nigerian woman, pregnant, she might have two jobs to go to. So she’s trying to maintain two jobs, keep the house going, and then you have the husband who believes he’s the man and the culture doesn’t allow him to come back and wash dishes and cook, and you know, she’s expected to come back from work still cook, clean, look after these kids and still be a wife and a mother” (H2, mw 1).
These self-efficacy skills or traits of FGNW are developed and perpetuated due to their functional state and evolve out of necessity for survival as migrants. According to Hamilton (2013: 174), “rather than perceiving resilience as an attribute which individuals either possess or do not, or being the product of a single cause, resilience is considered to be a disposition derived from a complex series of accumulated experiences”. In the case of FGNW, it is the researcher’s belief that fortitude and resilience are typical survival attributes engraved in the core of almost all Nigerian women at home and in the diaspora. Evidently, almost all Nigerian informants in the current study (midwives and women) held at least a first degree and hence were middle class, a demonstration of their self-actualisation.
However, the apparent work pressures and family commitments have implications for the health and wellbeing of the pregnant Nigerian woman in London who may be daunted by multiple commitments that do not allow time for attending antenatal care and other health promotion activities such as parenthood education sessions. Lack of their attendance in parenthood education classes was evident during the recruitment phase of this study, when every effort to recruit FGNW via parenthood classes proved futile due to their lack of attendance. As discussed previously, this situation could compound and perpetuate the reported poor outcome in comparison to their non-Nigerian counterparts in London who promptly attend antenatal care and parenthood education sessions. It is beneficial that FGNW achieve some rest and recuperation in the postnatal period through the omugwo ceremony, given the conflicting juxtaposition of work and other expectations in pregnancy.
FGNW appreciate and value maternity care services in London as a measure of acculturation and transition from a poor health provision in Nigeria to a more robust health care provision in their host nation, as apparent in the following comments by two of them:
“I was actually grateful” (FGN, wm 3).
“I will be too happy because if it is back home I mean you pay for it and, you just go to the midwife... here (sic: in Britain), its, its good” (FGN, wm 5).
FGNW expressed gratitude for free maternity care in London in the absence of an established National Health Service in their home country. This gratitude stems from their evaluation of maternity care in Nigeria which operates a ‘pay as you go’ health service system, with services rendered only to the members of the population who can afford the costs; against free maternity care in Britain. Moreover, in Nigeria, maternity care services suffer chronic limited infrastructure and poor administration, resulting in high levels of morbidity and mortality especially in childbirth. Poor birth outcome inherent in Nigeria’s maternity care provision was highlighted by Ezegwui and Nwogu-Ikojo (2005), who reported that almost 92% (91.9%) of women developed vaginal ï¬stula following prolonged obstructed labour. This had bearing on the reported ‘health tourism’ (CMACE, 2011) of FGNW, who might wish to escape the ill-fate of poor care outcome; and travel to London to receive effective maternity care. It is therefore understandable that they bear such positive affirmation of maternity services in London.
Therefore, there is positive optimism by a midwifery informant, that women should not lose their lives in a normal life event such as childbirth. The reference to death or “not dying from it” is a salient portrayal of the dread of morbidity and mortality associated with giving birth in Nigeria settings (World Health organization, 2004a, b). Nonetheless, this recent MBRRACE reports is in no way re-assuring of safer births in Britain. The notion of increased morbidity for FGNW experiencing birth in London is reiterated in the following comments from two different midwives working in two separate NHS trusts in London:
“You just have to be careful when you look after Nigerian women. When they come in through the door, they might be fine, next minute, something might go wrong, that is one thing I’ve learnt. They have a lot of it than the general population. Particularly PIH, one minute they’ll be fine, the next minute they’re not”. “Blood pressure is…, the rate is quite high among Nigerians” (H2, mw 2).
This is in line with findings of WHO (2012) study of health systems in Africa in which it was reported that, respondents in urban areas of Nigeria and other urban areas of West Africa reported hypertension as being common while rural areas in Nigeria reported higher levels of hypertension than the urban areas. Given the fivefold in perinatal mortality of BAME women, and earlier (CEMACH, 2007) report that, black African women suffer maternal mortality rates 5.6 times higher than Caucasians and the rest of the migrant populations in Britain (UNICEF, 2012). This could explain the uneasiness of some Nigerian midwives about caring for FGNW; coupled with the reported poor attitude/animosity of some FGNW to Nigerian midwives as portrayed in the following extract:
“I ‘don’t really like looking after Nigerians; because they come with a lot of baggage and they have lot of attitude; and they are very difficult to look after in labour. Particularly a lot of them don’t like we Nigerians again to care for them, I don’t know why. They believe we won’t give them the care or may be, they’ve come to abroad to be looked after by white people and when they see you, they get kind of “oh I don’t want her”. They get uneasy with you and they show a lot of attitude’ H2, mw 4).
FGNW’s mistrust of Nigerian midwives’ ability to deliver efficient care could stem from experiences of negative birth experiences or outcomes in Nigeria. This past negative care experience and outcome could generate anxiety and fear in the FGNW that could be perceived by the Nigerian midwife as rejection, or be interpreted by the annotated comment of the Nigerian midwife in the last quote as ‘baggage and attitude’. Such mistrust could be perceived as lack of trust in the midwife’s ability to deliver competent or congruent care that meets the care needs of FGNW. Nonetheless, the midwife informant in this situation could have explored the woman’s reason for expressing preference for a White midwife. Moreover, the inexperience of this midwife who has only been qualified for four years could engender insecurity, making her more sensitive to rejection, implied or otherwise. Bedwell (2012) report that, a significant proportion of midwives referred to lack of confidence in the job role as a factor for dissatisfaction and as the main reason for leaving the profession. Even so, the midwife could be weathering from the inherent discrimination endured by staff of BAME background in the NHS.
CONCLUSION
Similarities and incongruences between the expectations of FGNW and midwives have been explored in regards to emic care perspectives of FGNW and etic care app-roaches of midwives providing maternity care. From the narratives of both, apparent discrepancies exist between the care approaches of midwives and care expectations of FGNW and vice versa. Based on the dual accounts of both FGNW and midwives, it is apparent that midwives endeavour to work in line with their Nursing Midwifery Council UK Professional Code of Practice (2019/2015) but do not seem to understand or appreciate the rationale for some emic care practices of FGNW. Such divergence in care approaches could explain the divergent perspectives of midwives and FGNW in the annotated narratives.
It could be deduced from the analysis of this work that effective health promotion measures need to be adopted by midwives to address any incongruence in emic care approaches of FGNW and etic care approaches of midwives to ensure culturally congruent care. Given some of the highlighted reasons for some of the emic care practices of FGNW, midwives should encourage and affirm positive emic care approaches and counter potentially harmful practices such as the notion of ‘evil eye’, aversion to caesarean section and some other untoward practices, as a way of affirming competency in maternity care and enhancing congruency in meeting the care needs of FGNW accessing maternity care in London.
A framework for providing Culturally Congruent Care for FGNW based on the theoretical frameworks and philosophies that underpin this study is formulated and recommended to effect maternity care that is culturally congruent and competent for this population. In next article to follow, interpretation and synthesis of know-ledge espoused from this study is to be presented and summarized to inform effective approaches of midwives and FGNW based on Culture Care Midwifery Module.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
ACKNOWLEDGMENTS
The author expresses her gratitude to first- generation Nigerian women and midwives within three NHS Trusts in South London for honouring the invitation to participate in this study and for their insightful contribution to the data generated through focus group and interviews.
REFERENCES
|
Adami MF, Kiger A (2005). The use of triangulation for completeness purposes. Nurse researcher 12(4). Crossref |
||||
|
Adewuye AO, Ola BA, Aloba OO (2007). Relevance and correlates of depression in late pregnancy among Nigerian women. Depression and Anxiety 24:15-21. Crossref |
||||
| Anugwom ED (2007). Starting out: The Omugwo practice and instilling the rudiments of childrearing in mothers among the Igbo of Southeastern Nigeria. Reproduction, childbearing and motherhood: A cross-cultural perspective pp. 155-166. | ||||
|
Aquino MRJV, Edge D, Smith DM (2015). Pregnancy as an ideal time for intervention to address the complex needs of black and minority ethnic women: Views of British midwives. Midwifery 31(3):373-379. Crossref |
||||
| Aveyard H, (2010). Doing a literature review in qualitative research in Health and Social Care: A practical guide (second edition). Open University Press, London. | ||||
|
Barwell I (2009). Understanding narratives and narrative understanding. The Journal of Aesthetics and Art Criticism 67(1): 49-59. Crossref |
||||
| Bedwell C (2012). An analysis of the meaning of confidence in midwives undertaking intrapartum care (Doctoral dissertation, University of Manchester). | ||||
| Blunt L (2014). Improving Service User Experience in Maternity Services. A report prepared by The Patient Experience Network. The Patient Experience Network. | ||||
|
Bonevski B, Randell M, Paul C, Chapman K, Twyman L, Bryant J, Hughes C (2014). Reaching the hard-to-reach: a systematic review of strategies for improving health and medical research with socially disadvantaged groups. BMC Medical Research Methodology 14(1):42. Crossref |
||||
| Bowling A (2009). Research Methods in Health (3rd Ed). Open University Press: London. | ||||
| Bowling A (2014). Research methods in health: investigating health and health services. McGraw-Hill education (UK). | ||||
|
Braun V, Clarke V (2006). Using thematic analysis in psychology. Qualitative Research in Psychology 3:77-101. Crossref |
||||
|
Bryman A (2004). Social Research Methods (Second edition). Oxford: Oxford University Press. Crossref |
||||
|
Callister LC, Khalaf I (2010). Spirituality in childbearing women. The Journal of perinatal education 19(2):16 Crossref |
||||
| Centre for Maternal and Child Enquires (CMACE) (2011). Saving Mothers' Lives: Reviewing Maternal Deaths to make Motherhood Safer: 2006-2008. British Journal of Obstetrics and Gynaecology Press Wiley-Blackwell, London. | ||||
| Cluett E, Bluff R (2000). Principles and Practice of Research in Midwifery Edinburgh. London, New-York, Philadelphia, St Louise, Sydney, Toronto: Baillére Tindal. | ||||
| Confidential Enquiries into Maternal and Child Health (CEMACH) (2004). Why Mother's Die 2000-2002 - Report on Enquiries into Maternal Deaths in the United Kingdom. Royal College of Obstetrics and Gynaecology Press, London. | ||||
| Confidential Enquiry into Maternal and Child Health (CEMACH) Perinatal Mortality (2007). United Kingdom. CEMACH, London. | ||||
| Cowman S (2008). Triangulation. Nursing Research: Designs and Methods. R. Watson, H. Mckenna, S. Cowman, J. Keady eds. USA: Elsevier pp. 269-278. | ||||
| Cross C, Gelderblom D, Mafukidze J, Roux N (2006). Views on migration in Sub-Saharan Africa: Proceedings of an African Migration Alliance workshop. HSRC Press. | ||||
|
Department of Health (DH) (2005). Race Equality Scheme. |
||||
|
Dike P (2013). Birth practices of Nigerian women: a literature review. African Journal of Midwifery and Women's Health 7(1):39-48. Crossref |
||||
|
Elwood SA, Martin DG (2000). "Placing" interviews: location and scales of power in qualitative research. The professional geographer 52(4):649-657. Crossref |
||||
|
Ezegwu HU, Nwogu-Ikojo EE (2005). Vesico-vaginal ï¬stula in Eastern Nigeria. Journal of Obstetrics and Gynaecology 25(6): 589-591. Crossref |
||||
|
Gil-González D, Carrasco-Portiño M, Vives-Cases C, Agudelo-Suárez AA, Castejón Bolea R, Ronda-Pérez E (2015). Is health a right for all? An umbrella review of the barriers to health care access faced by migrants. Ethnicity & Health, 20(5):523-541. Crossref |
||||
|
Hamilton PL (2013). It's not all about academic achievement: supporting the social and emotional needs of migrant worker children. Pastoral Care in Education 31(2): 173-190. Crossref |
||||
|
Helman C (2007). Culture, health and illness. CRC press. Crossref |
||||
|
Hussein A (2009). The use of Triangulation in Social Sciences Research: Can qualitative and quantitative methods be combined? Journal of Comparative Social Work 1(8):1-12. Crossref |
||||
|
Izugbara CO, Etukudo IW, Brown AS (2005). Trans-ethnic itineraries for ethno-medical therapies in Nigeria. Crossref |
||||
|
Jiménez TR, Horowitz AL (2013). When white is just alright: How immigrants redefine achievement and reconfigure the ethnoracial hierarchy. American Sociological Review, 78(5): 849-871. Crossref |
||||
| Katbamna S (2000). "Race" and Childbirth. Buckingham: Open University Press. | ||||
|
Kincheloe JL, McLaren P (2011). Rethinking critical theory and qualitative research. In Key works in critical pedagogy (pp. 285-326): Brill Sense. Crossref |
||||
|
Kumar R (2019). Research methodology: A step-by-step guide for beginners. Sage Publishing. |
||||
| Leininger MM (2002). The theory of culture care and the ethno-nursing research method. In: Leininger MM, McFarland MR (Eds.), Transcultural nursing: Concepts, Theories, Research, and Practice (3rd edition). New York, NY: McGraw-Hill. | ||||
| Leininger MM (2006a). Culture care diversity and universality theory and evolution of the Ethno-nursing method'. In MM Leininger, MR McFarland (Edition), Culture care diversity and universality: A worldwide nursing theory (2nd edition). Sudbury, MA: Jones and Bartlett Publishers. | ||||
| Leininger MM, McFarland MR (2006). Culture Care Diversity and Universality: A Worldwide Nursing Theory. Sudbury, MA: Jones and Bartlett Publishers. | ||||
| Liamputtong P (2007). Childrearing and infant care issues: A cross-cultural perspective. Nova Publishers. | ||||
| Maalouf A (2012). Violence and the Need to Belong: In the Name of Identity. Penguin Books: London. | ||||
|
MacFarlen A, Dzebisova Z, Karapish D, Kovacevic B, Ogbebor F, Okonkwo E (2009). Arranging and negotiating the use of informal interpreters in general practice consultations: Experiences of refugees and asylum seekers in the west of Ireland. Social Science and Medicine 69(2):210-214. Crossref |
||||
|
Mitchell JR, Baker MC (2000). Religious commitment and the construct of sources of help for emotional problems. British Journal of Medical Psychology 73(3):289-301. Crossref |
||||
|
Morhason-Bello IO, Adedokun BO, Ojengbede OA (2009). Social support during childbirth as a catalyst for early breastfeeding initiation for first-time Nigerian mothers. International Breastfeeding Journal 4(1):16. Crossref |
||||
|
Moscardino U, Nwobu O, Axia G (2006). Cultural beliefs and practices related to infant health and development among Nigerian Immigrant mothers in Italy. Journal of Reproductive and Infant Psychology 24(3):241-255. Crossref |
||||
| Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries across the UK (MBRRACE-UK) (2014). Saving Lives, Improving Mothers Care lessons learned to inform future maternity care from the UK and Ireland. Confidential Inquiries into Maternal Deaths and Morbidity 2009-2012. National Perinatal Epidemiology. | ||||
|
Nadeem R, Lange JM, Miranda J (2008). Mental Health preferences among low-in-come and minority women. Archives of Women's Mental Health 11(2):93-102. Crossref |
||||
| National Institute for Health and Clinical Excellence (NICE) (2008). Antenatal Care for the Healthy Pregnant Woman. Royal College of Obstetrics and Gynaecology (RCOG) Press: London. | ||||
| National Service Framework (NSF) (2007). Children's health, our future: a review of progress against the National Service Framework for Children, Young People and Maternity Services 2004. Department of Health: England. | ||||
| Nursing and Midwifery Council (Great Britain) (2015). The Code: Professional standards of practice and behaviour for nurses and midwives. NMC. | ||||
| Nursing Midwifery Council UK (2019). The Code: Professional standards of practice and behaviour for nurses, midwives and nursing associates. NMC UK. | ||||
| Nwokocha EE (2007). Maternal crises and the role of African men: the case of a Nigerian community. | ||||
| Nzegwu N (2004). Cultural Epistemology of Motherhood: Refining the Concept 'Mothers'. Journal of Culture and African Women Studies: www. jendajournal. com/issue5/nzegwu. htm (accessed 6 December 2012). | ||||
| Nzegwu N (2004). The epistemological challenge of motherhood to patriliny. JENdA: A Journal of Culture and African Women Studies (5) | ||||
|
Oates MR, Cox JL, Neema S, Asten P, Glangeaud-Freudenthal N, Figueiredo B, Klier CM (2004). Postnatal depression across countries and cultures: a qualitative study. The British journal of psychiatry, 184(S46): s10-s16. Crossref |
||||
| Office for National Statistics (ONS) (2009). Life expectancy at birth and at age 65 for health areas in the United Kingdom, 2003-05 to 2007-09'. ONS: London. | ||||
| Office for National Statistics (ONS) (2012). Population by country of birth and nationality. ONS: London. | ||||
|
Ohaeri JU (1998). Perception of the Social Support Role of the Extended Family Network by some Nigerians with Schizophrenia and Affective disorders. Social Science and Medicine 47(10): 1463-1472. Crossref |
||||
|
Papadopoulos I, Tilki M, Ayling S (2008). Cultural competence in action for CAMHS: Development of a cultural competence assessment tool and training programme. Contemporary Nurse 28(1-2):129-140. Crossref |
||||
|
Pearlin LI (1989). The Sociological Study of Stress. Journal of Health and Social Behaviour 30:241-256. Crossref |
||||
| Polit DF, Beck CT and Hungler BP (2001). Essentials of Nursing research - Methods, Appraisal and Utilization', 5th edition. JB Lippincott: Philadelphia. | ||||
| Psoinos M, Hatzidimitriadou E, Butler C, Barn R (2011). Ethnic monitoring in healthcare services in the UK as a mechanism to address health disparities: a narrative review. | ||||
|
Raine R, Cartwright M, Richens Y, Mahamed Z and Smith D (2010). A qualitative study of women's experiences of communication in antenatal care: Identifying areas for action'. Maternity and Child Health Journal 14(4):590-599. Crossref |
||||
| Rees C (2011). An Introduction to Research for Midwives E-Book. Elsevier Health Sciences. | ||||
|
Sandall J, Benoit C, Wrede S, Murray SF, van Teijlingen ER, Westfall R (2009). Social Service Professional or Market Expert? Maternity Care Relations under Neoliberal Healthcare Reform. Current Sociology 57(4):529-553. Crossref |
||||
|
Smith J, Firth J (2011). Qualitative data analysis: the framework approach. Nurse researcher 18(2):52-62. Crossref |
||||
| Smith LK, Draper ES, Manktelow BN, Fenton A, Kurinczuk JJ (2019). MBRRACE-UK Supplementary report on survival up to one year of age for babies born before 27 weeks gestational age. | ||||
| Steup M (2014). Epistemology. I Edward N. Zalta (Red.). | ||||
|
Ukwuani FA, Suchindran M (2003). Implications of women's work for child nutritional status in sub-Saharan Africa: a case study of Nigeria. Social Science and Medicine 56:2109-2121. Crossref |
||||
| UNICEF United Kingdom Baby Friendly initiative (2012). Transforming healthcare for babies, their mothers and families in the UK.UNICEF UK. | ||||
|
Weller K, Kinder-Kurlanda KE (2016). A manifesto for data sharing in social media research. In Proceedings of the 8th ACM Conference on Web Science ACM pp. 166-172. Crossref |
||||
| World Health Organisation (WHO) (2012). Respectful Maternity Care: The Universal Rights of Childbearing Women. | ||||
| World Health Organisation (WHO) (2004a). Maternal Mortality in 2000: Estimates Developed by WHO, UNICEF and UNIFPA. WHO, Geneva. | ||||
| World Health Organisation (WHO) (2004b). Commission on Social Determinants of Health: Note by the Secretariat. WHO: Geneva. | ||||
| Zumpe J, Dormon O, Jefferies-ONS J (2012). Childbearing among UK born and non-UK born women living in the UK. | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


