Full Length Research Paper
ABSTRACT
For women with irritable bowel disease (IBD), leading a healthy life during the perinatal period is important because it may affect their quality of life and motherhood. However, little attention has been paid to their challenges and the methods of coping with them. This study therefore aims to explore the challenges women with IBD face and the methods of coping with them during the perinatal period from their viewpoint. Exploratory, qualitative interview study design was used in this study. In-depth, one-on-one, semi-structured interviews were conducted in 2010 to 2011 among eight women having IBD, who experienced pregnancy, delivery and child rearing. The results of the interviews were analyzed by inductive content analysis. The participants recognized the following as challenges: high-risk management by obstetricians in collaboration with gastroenterologists, high risk to physical, mental and social well-being due to IBD relapse, limitation of information necessary during the perinatal period, issues related to the medical profession, and breastfeeding in their own way. They were coping with these issues by self-care for IBD, and making the most of various social support. Since IBD is often diagnosed during women’s reproductive years, gastroenterology and obstetric specialists should cooperate with each other to routinely provide reproductive counseling to women with IBD. Furthermore, we should establish, as early as possible, health care communities for women with IBD, where they can maintain their quality of life and increase their preparedness for parenthood before pregnancy and during the perinatal period, based on multidisciplinary collaboration.
Key words: Inflammatory bowel disease (IBD), women’s health, nursing, midwifery, multidisciplinary collaboration, reproductive care, pregnancy, child rearing, chronic illness, gastroenterology, qualitative approach.
INTRODUCTION
Recently, the incidence of inflammatory bowel disease (IBD), comprising ulcerative colitis and Crohn’s disease, a chronic, refractory and debilitating disease, has been increasing around the world, and has been acknowledged as a global disease (Molodecky et al., 2012). In Japan, the age-adjusted morbidity (/100,000 people) of IBD was estimated to be 84.5 for ulcerative colitis and 26.3 for Crohn’s disease in 2009 (Kuwahara and Asakura, 2013).
As the incidence of IBD has so increased in Japan as in other countries, IBD has become a major social issue.
IBD is considered to involve a complex interaction of four different mechanisms – a genetic predisposition that results in immune regulatory cell derangement, defects in the mucosal barrier, susceptibility to environmental triggers including specific antigens, and commensal bacteria in the patient’s intestinal lumen. IBD is characterized by repeated periods of remission and exacerbation, accompanied by fecal urgency, frequent bowel movements, diarrhea, rectal bleeding, loss of appetite, abdominal pain and fatigue. Further, IBD affects joints, eyes, skin, bones and organs other than the intestine during the course of the disease. Relapsing IBD attacks sufferers unexpectedly, and this calls for frequent medical checks at clinics or hospitals. Consequently, IBD sufferers experience mental fatigue (Beck et al., 2013), as well as social disabilities including unemployment, sick leave, unfulfilled potential in the workforce (Mallett et al., 1978; Bernklev et al., 2006) and deterioration of quality of life associated with health (Guassora et al., 2000; Graff et al., 2006; Lix et al., 2008; Jäghult et al., 2011) in addition to physical distress. Most IBD sufferers are diagnosed in the second or third decade of their life (Takebayashi and Nishiwaki, 2007; Bernick and Kane, 2010), and they experience significant life events, such as entering school, employment, marriage, pregnancy and delivery, after the development of IBD. Especially, since approximately 25% of women with IBD were reported to conceive for the first time after diagnosis (Baiocco and Korelitz, 1984), special care is needed in the perinatal management of women with IBD.
Recently the public has paid more attention to the health of women with IBD, especially medical aspects such as intensified symptoms, known as ‘mini-flares’, difficulties before and/or during menstruation (Kane, 2002), fertility (Willoughby and Truelove, 1980; Steinlauf and Present, 2004), the risk of deterioration of IBD during pregnancy (Alstead, 2002; Reddy et al., 2008; Habal and Huang, 2012), effects of drugs for IBD treatment during pregnancy (Coelho et al., 2011) and breastfeeding (Kane, 2002; Habal and Kapila, 2009). On the other hand, only a few studies have reported on the transitional process to parenthood for women with IBD, their experiences in the perinatal period (Mukherjee et al., 2002), and women with aggravated IBD during pregnancy (Cooper et al., 2011).
Research to elucidate how IBD affects mothers and their families including children in the transition period to motherhood would be useful for IBD women to prepare for their parenting role and to create new families. Findings from such studies would serve as effective information for health professionals, such as physicians, nurses and midwives, when supporting IBD women and their families in the reproductive period. Thus, the aim of this study was to examine the challenges women with IBD face and how they handle them, and to focus on the role of health professionals in supporting women with IBD from pregnancy to child rearing .
METHODOLOGY
Design
An exploratory design was employed, in order to elucidate the ascribed significance and perspectives of IBD women based on their experiences from pregnancy to child rearing.
Participants
The inclusion criteria were women with IBD within five years after the latest childbirth without serious complications and/or the history of mental disorder, and who were in a good condition in the IBD remission stage. They were given the formal request for this study including the email address of the primary investigator by a gastroenterologist, the second investigator, at a gastroenterology clinic in Saitama, Japan, or through internet sites where women could link to this study via the representative of the Society of Patients with Intractable Diseases. Although, ten women with IBD expressed their will to participate in the study, two abstained from interviews due to serious health conditions, and eight participated in the study. After receiving emails from women with IBD, the primary investigator returned a compliment and scheduled interviews.
Data collection
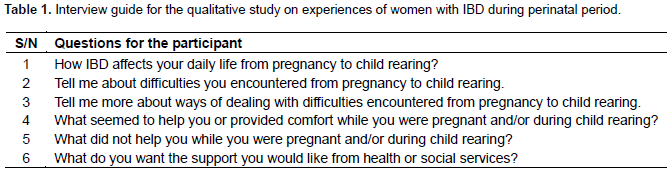
In 2010 to 2011, CK (the first author) conducted in-depth, one-on-one, semi-structured interviews (for 1.5 to 2 h) with eight women with IBD, at their homes, considering their physical condition, especially bowel control, and busy life due to child rearing, in order to interview them in a quiet and calm atmosphere. The interview guide had been prepared in advance by reviewing previous research (Mukherjee et al., 2002) that handled similar topics to ours. On the day of interviews, written informed consent was obtained before the interview. The participants first completed a brief questionnaire consisting of demographics, IBD history such as diagnosis, medication and surgery, and obstetric history, followed by a series of open-ended questions (Table 1). The interviews were tape-recorded with the participants’ permission, and transcribed verbatim by an experienced transcriber.
Ethical considerations
Ethical permission was obtained from the Tokyo Metropolitan University Ethics Committee. We assured the participants of their voluntary participation, protection of confidentiality/privacy, and right to withdraw participation whenever they want. Moreover, we explained that they could choose the date of the interview, and could suspend the interview at any time according to their physical condition. Lastly we explained the possibility of publishing our research findings in the future.
Data analysis
The contents of the recorded interviews were analyzed by inductive content analysis (Graneheim and Lundman, 2004; Elo and Kyngäs, 2008). The transcription was first read through several times to obtain a sense of the whole (Burnard, 1991). Then, the text about the participants’ experiences during the perinatal period was extracted as a unit of analysis, condensed as an analytical unit, and labeled with a code (Graneheim and Lundman, 2004). Next, the various codes were compared based on differences and similarities, and grouped into sub-categories, which were then abstracted and named using content-characteristic words. Sub-categories with similar events were grouped together as categories, and the categories were further grouped as themes. The tentative categories were examined by two researchers (the authors) and amended. Finally, the codes, sub-categories, categories and themes were tabulated, and it was reconfirmed that the classification presented the validity and totality of the original narratives of the participants. In this connection, we quoted, in our manuscript, the participants’ original narratives that seemed to most appropriately represent the phenomena or meaning based on the empirical data.
Rigour
The researchers examined the rigour of our qualitative research based on the following five standards: credibility, transferability, dependability, conformability and authenticity (Guba and Lincoln, 1994). Concerning credibility, the researchers conducted a peer debriefing to compare the emerging codes and themes with the contents of the transcripts and interview summaries, and verified them in order to enhance the credibility of the findings. To ensure dependability and conformability, the researchers tape-recorded all interviews, and transcribed them verbatim, while preserving the documents/memos including all the trails of procedures or decision making regarding the research methodology. For this purpose also, the researchers utilized peer debriefing. As for transferability, the researchers reviewed the research findings of other studies concerning perinatal experiences or perinatal care of women suffering from other chronic diseases or disabilities, and provided, in the discussion section, sufficient descriptive data to enable the readers to evaluate the applicability of the data to other settings by comparing our research findings with others. Finally, concerning authenticity, the researchers repeatedly read the transcripts in consideration of the preliminary themes, and provided descriptive data, using the narratives of the participants categorized from the meaningful units in the synthesized sub-categories.
RESULTS
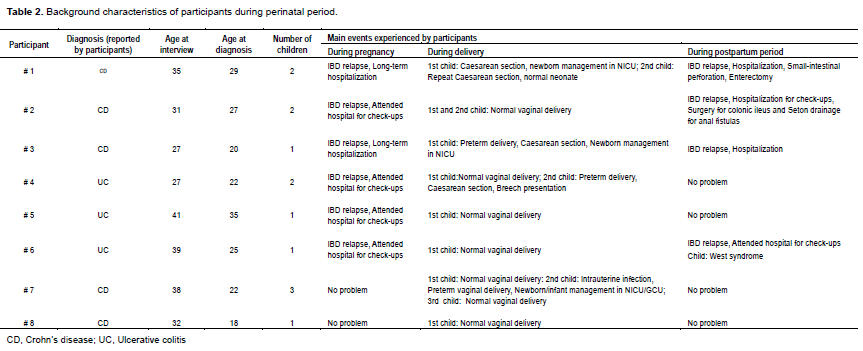
Table 2 shows the characteristics of the participants. All participants were aged between 27 and 41 years (mean: 33.8 years), with children aged from 7 months to 7 years. Three participants had two children, and one had three children. All participants were diagnosed with IBD when they were 18 to 35 years old. The diagnoses they reported are shown in Table 2. Although, the severity of symptoms varied, six participants experienced a relapse of IBD during pregnancy, and four had deterioration of IBD after delivery. Three participants had caesarean sec-tions, and three had a preterm delivery, including one with caesarean section because of IBD, which necessitated the newborn’s admission to the Neonatal Intensive Care Unit (NICU). Two women with Crohn’s disease remained in remission by using biological preparation (#7) or mesalazine (#8) from pregnancy to child-rearing. One woman, per doctor’s orders, stopped taking biological preparation during the first trimester, but resumed from the second trimester through postpartum due to relapse (#2). One started to take biological preparation after enterectomy due to her small-intestinal perforation three months postpartum (she took mesalazine from pregnancy to two month postpartum) (#1). One woman began a course of biological preparation after her caesarean section due to relapse despite steroid use during pregnancy (#3). All three women with ulcerative colitis maintained their health by using mesalazine or predonine enema in spite of slight flares during pregnancy. These three women took the above-mentioned medications during postpartum, and two had no relapse (#4, 5). One experienced relapse due to stress related to her child’s disease, West syndrome (#6). We here present the challenges women with IBD faced and the methods of coping with them based on the main themes derived from the qualitative data. The names of participants are con-cealed and replaced with numbers to assure anonymity.
Experiences of women with IBD during perinatal period
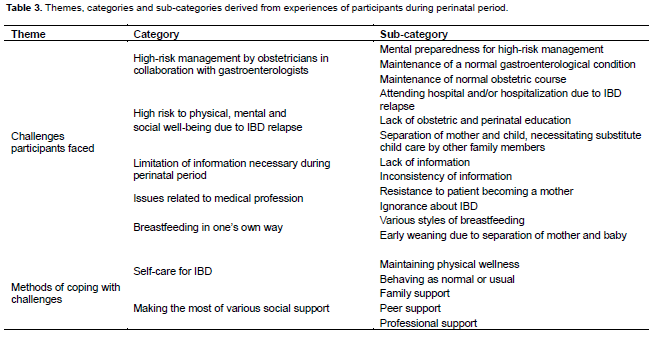
We identified two themes derived from the experiences of women with IBD during the perinatal period: challenges women with IBD faced and methods of coping with the challenges, as summarized in Table 3.
Challenges women with IBD faced
We identified five categories under the heading “Challenges women with IBD faced”: High-risk manage-ment by obstetricians in collaboration with gastroentero-logists; high risk to physical, mental and social well-being due to IBD relapse; limitation of information necessary during perinatal period; issues related to medical profession; breastfeeding in one’s own way.
High-risk management by obstetricians in collaboration with gastroenterologists: Participants in this study described three concepts: mental preparedness for high-risk management, maintenance of a normal gastroenterological condition and maintenance of normal obstetric course. They felt that these concepts influenced each other.
1. Mental preparedness for high-risk management: Though the participants felt it was a bother to receive management by both an obstetrician and a gastroenterologist, they accepted the high-risk management as a safe system.
“My pregnancy was risky because I needed to be managed by both an obstetrician and a gastro-enterologist. It was bothersome for me to have check-ups in two different departments. But I felt at ease to know that collaborative management was possible if needed.”
2. Maintenance of a normal gastroenterological condition: Most participants continued to take medication and/or elemental dietary supplement (Elental) to control IBD. However, frequent bowel movements with associated faecal urgency and anemia did not resolve. Therefore, the participants tried to lead a stress-free life with a wait-and-see approach without receiving check-ups, refraining from going out, etc.
“I took 5-ASA (mesalazine) during my pregnancy because my IBD symptoms were severe. But my symptoms did not get better. And I had little trouble in my daily living though I felt sluggish due to anemia. The worst thing about this disease is that I have little time from when my stomach starts hurting to get to a restroom. So, I tried to only go to places where I could find a toilet easily.”
3. Maintenance of normal obstetric course: The participants tried to continue taking Elental during pregnancy to maintain a normal fetal body weight. When the courses of IBD and pregnancy were normal, they led lives like a healthy woman, almost forgetting about IBD.
“I tried to take Elental for growth of my baby, but I couldn’t while I was pregnant. My obstetrician, gastroenterologist and I monitored the growth of my baby with ultrasound scans. Other than that, my condition was good while I was pregnant, and I had a really happy, stress-free time. It was as if my IBD disappeared!”
High risk to physical, mental and social well-being due to IBD relapse: When IBD relapsed, participants in this study experienced three major concerns: attending hospital and/or hospitalization because of IBD relapse, lack of obstetric perinatal education and separation of mother and baby necessitating substitute childcare by other family members. All these factors negatively affected the physical, mental and social well-being of the mothers and their families.
1. Attending hospital and/or hospitalization because of IBD relapse: Six pregnant and four postpartum participants had an IBD relapse, and attended hospital and/or were hospitalized in the gastroenterology department. One participant who had to be hospitalized for a long time from pregnancy to the postpartum period and underwent abdominal surgery after caesarean section experienced intolerable abdominal stinging and mental distress including anxiety about insufficient preparedness for motherhood.
“I had an emergency admission to hospital because of inflammation of the small intestine when I was four months pregnant. I couldn’t eat anything, and received only intravenous hyperalimentation for a long time, and restarted steroid use. As my baby grew, it pressed on my small intestine, and I was having intolerable abdominal pain. I was depressed. I was worried about whether I could take care of my baby.”
2. Lack of obstetric and perinatal education: All participants who were hospitalized because of IBD relapse commonly experienced adaptation delay in postnatal child rearing because of insufficient preparedness for motherhood.
“I had no chance to prepare for delivery or childcare like mothers who were attending mothers’ classes, and so, I didn’t have any childcare skills because I was in hospital so long. After the caesarean section, I underwent abdominal surgery again, so my husband and mother-in-law had to take care of my baby for 2 months.”
3. Separation of mother and baby necessitating substitute childcare by other family members: Participants who had to be hospitalized for IBD relapse commonly experienced separation from their baby, and were forced to discontinue breastfeeding. Their own mothers and mothers-in-law had to take care of their babies, and the grandmothers experienced refusal of bottle-feeding by the babies, resulting in weaning babies from milk and starting supplementary foods.
“I had a normal postpartum after a C-section, but one day I suddenly developed strong abdominal pain. I took my two daughters to my parents-in-law by car and left them there. I was then taken to hospital by ambulance, and had an emergency enterectomy. It was a close call, and I am glad I survived. I was hospitalized and separated from my baby, and so my mother had to wean my baby from milk and started to give her solid food, little by little. My daughter was exclusively breastfed until that time, so my mother had a lot of trouble.”
Limitation of information necessary during perinatal period: The participants searched on the internet for the effects of IBD on pregnancy and delivery while consulting their doctors at all reproductive stages. They were confused by the lack and/or discrepancy of information.
Lack of information: Most participants stated that they had little or no information from other women with IBD. They searched for information about IBD and pregnancy/delivery on the internet as the first step. They asked their gastroenterologists to provide them with information, but they could only receive information limited to medical aspects of IBD.
“I searched the web for information on how other women with IBD were dealing with difficulties during pregnancy and delivery because I couldn’t get such information from other women with IBD. My doctor just gave me some papers written by other doctors.”
Inconsistency of information: Most participants searched for the effects of medication, especially of Infliximab and/or painkillers, on the internet. However, they could not find accurate information. Moreover, they recognized the inconsistency of information given by doctors from different specialty areas, and were confused by discrepancies.
“I searched for the effects of Infliximab and painkillers on the internet. But I couldn’t find accurate information on the fetus and breastfeeding, so I was afraid of the effects. For example, I felt that the internal medicine doctor’s opinion wasdifferent from that of surgeons with regard to the use of painkillers for my anal pain.”
Issues related to medical profession
This category included two sub-categories: resistance to patient becoming a mother, and ignorance about IBD among nurses and midwives.
Resistance to patient becoming a mother
One participant encountered direct resistance to her desire to have a baby by the gastroenterologist during the pregnancy. She was greatly hurt, and continued to have feelings of inferiority about having a child even in the later child-rearing stage, five years after delivery. However, she balanced her negative feelings with the confidence that she could deliver a child and love her.
“I don’t want to mention, but the doctor said to me “Don’t you care about your husband and children and the problems they’ll have because of your IBD?”. After that, I always had a feeling of inferiority. But my children are very lovely. I am happy that I could deliver babies and can take care of them.”
Ignorance about IBD
The participants expressed their gratitude to nurses and midwives for their compassionate care, while they considered that the nursing profession had only limited knowledge about IBD. Therefore, some participants did not dare to consult nurses and midwives about their disease or concerns.
“I think that the midwives didn’t care about my disease during pregnancy and the postpartum. I had a normal pregnancy and delivery, and so, I didn’t consult them. I felt that they did not know much about IBD, anyway.”
Breastfeeding in one’s own way
The participants experienced various styles of breastfeeding including exclusive/partial breastfeeding, early weaning due to separation of the mother and baby.
Various styles of breastfeeding
Seven participants practiced and enjoyed exclusive or partial breastfeeding, and finally accepted their own style of breastfeeding.
“I wanted to exclusively breastfeed my baby. I can contact my baby warmly while breastfeeding, and it makes me feel like a mother. All my friends exclusively breastfed their babies. So I wanted to do so, too.”
Early weaning due to separation of mother and baby
Five participants, who had to introduce artificial milk or supplementary food to their babies when they were hospitalized for IBD relapse, did not consider the change to be negative, and understood that it was a necessary decision.
“I had to stay in hospital during the early period of childcare. One week after my hospitalization, my daughter was weaned from breast milk and began to take formula milk. But I think it was a good choice because I just had to do so.”
Methods of coping with challenges
This theme was summarized into two categories: self-care for IBD and making the most of various social support.
Self-care for IBD
The participants categorized self-care for IBD into two: maintaining physical wellness and behaving as normal or usual.
Maintaining physical wellness: The participants were making efforts to maintain their physical wellness from the perspective of IBD sufferers, though they continued to avoid food unsuitable for their constitution, prevent fatigue, and monitor for bloody stools and the pattern of bowel movements.
“Oily or cold foods affect my abdominal condition, especially ice cream. So I don’t eat it. I have dairy products with low fat. I pay careful attention to the amount of sleep I have, and try not to get too tired. I always have diarrhea and frequent bowel movements when I am tired.”
Behaving as normal or usual: In social relationships, the participants adopted two ways of letting other people know about their disease; by getting people to understand IBD without concealing it, or by avoiding informing people except their family members and friends about IBD. In these ways, they felt comfortable and able to prevent stress or problems.
“I used to talk about my disease to my old friends be-cause I didn’t want to conceal it. It was easier for me. But, now, I don’t tell my friends who are also mothers about my disease. I feel it is not necessary to tell them about my IBD.”
Making the most of various social support
Three sub-categories of social support utilized by the participants were identified: family support, peer support and professional support.
Family support
Regardless of IBD relapse, the participants commonly utilized the support of their parents (or parents-in-law) as the first choice, which covered complete or partial childcare. Partners’ support consisted of emotional or financial support.
“During my regular checkups and hospitalization for IBD relapse, my parents take care of my child. My husband always comes back home late at night, so I can’t rely on him on weekdays. My husband and children spent time with me every weekend in the hospital.”
Peer support
Most participants had already established networks with female friends with IBD before their pregnancy or in the perinatal period. They had received effective information to visualize concrete images of daily life during the perinatal period, from the viewpoint of IBD sufferers.
“My friend with IBD became pregnant, and delivered a baby a few months earlier than me. She has Crohn’s disease, and talked to me about her experience. We have been friends for a long time. I can ask her at any time about pregnancy/delivery and child-rearing, as well as about IBD.”
Professional support
All participants had established a strong relationship with their IBD specialists. The IBD specialists monitored the symptoms of the participants, guided them about ways to have a healthy life based on their clinical assessment, and provided them with appropriate information and necessary treatment. IBD specialists were the persons who offered a sense of security to IBD women and their families.
“I always depend on my doctor. If I have any problem with the disease, I go to the clinic at any time. My doctor suggested a good time to get pregnant, with consideration of my condition.”
DISCUSSION
Strategies for IBD women to overcome difficulties in perinatal period
The participants in this study had regularly monitored their IBD symptoms, such as diarrhea, by themselves, and paid close attention to diet and keeping themselves rested to maintain physical well-being in the same way as they did before pregnancy. This is in agreement with the research finding that many IBD sufferers acquire the ability to take care of themselves in order to maintain ‘normality as an IBD sufferer’ in their own way (Fletcher and Schneider, 2006; Fletcher et al., 2008; McCormick et al., 2012). Since the perinatal period is a transitional stage, which is associated with changes in the family sys-tem and the need to acquire new parental skills including breastfeeding, all couples experience some psychological stress. As women with IBD have only limited information about pregnancy and the disease, it is important for them to pay attention, before pregnancy, to their daily diet, rest, coping with stress, symptom control by medication, and postpartum childcare, and discuss these concerns with their families.
Regarding self-care for psychological health, some participants thought it was better to pretend to be normal and experience ordinary daily life as if they were healthy women, in spite of their difficult experiences of IBD relapse in the perinatal period. Maintaining ‘health-related normality’ and ‘pretending to be normal’ are reported to be essential for IBD sufferers (Hall et al., 2005). The same was true for the participants in this study. If IBD sufferers had a relapse in the perinatal period, they would be categorized into the group of ‘pregnant women with disability’. When women with difficulties (example, disability or illness) receive reproductive care, they are forced to confront tasks different from those women with a normal course, including collection of various information about repro-ductive health care, despite little information being available, and to spend the perinatal period communicating effectively with multidisciplinary care providers (Wong, 2000).
However, women with disabilities are adaptive to and knowledgeable about their own conditions and difficulties, and want to be respected by healthcare professionals as individuals (Barber, 2008). Therefore, women with dis-abilities, in particular those with ‘a high risk’, should have the chance to access appropriate maternity-care information and consultation as easily as their ‘low risk’ or ‘normal’ counterparts enjoy, and be looked after by a health care system that supports their maternal identity and values (Walsh-Gallagher et al., 2012). Most parti-cipants in our study could overcome the challenges during the perinatal period by making use of various social support. Especially, family support during IBD relapse was essential for IBD women to become a parent while overcoming difficulties. As the perinatal period is a transitional stage not only for IBD women but also for their family members, IBD women should develop supportive communication with their families through having anticipatory guidance on the risk of relapse and coordinated childcare with their partners and/or family members.
Further, most participants had utilized gastroenterologist as one of their social supports. In particular, they had received suggestions about the appropriate time to get pregnant and information about the interaction between pregnancy and IBD when they planned to get pregnant. At the same time, they had searched for this information on the web. These findings coincide with the results of previous studies showing that the particular information sources about pregnancy for IBD women were gastroenterologists and the internet (Marri et al., 2007; Mountifield et al., 2009; Gawron et al., 2014). Although, the internet should not be the main source of information for women with IBD, as people are accustomed to seeking information on the internet, it would probably be necessary to have a reliable web-based information package for pregnant IBD patients and those planning to get pregnant including specific guidance for daily life from before pregnancy to postpartum such as self-care and/or social supports including family and/or peers.
Considering that the peak age of IBD onset is during the reproductive period, IBD women should receive ap-propriate reproductive health guidance before pregnancy, on an individual or group basis, as follows: appropriate time to get pregnant, various courses and risks in the perinatal period, effects of IBD medication on pregnancy/ breastfeeding, necessity for high risk manage-ment, ways to get appropriate information and methods of coping with IBD relapses. At the, IBD women should have the opportunity to come in contact with peers with IBD, and establish a supportive environment, such as a ‘buddy system’ with peers, by themselves, because they usually hesitate to talk about IBD-related topics that are rarely covered in regular parents’ classes (Blackford et al., 2000).
Roles of health professionals involved in care of women with IBD
Gastroenterologists are the key sources for women with IBD of reproductive age who decide to have a baby. Therefore, they should always support IBD women in their decision-making by providing them with updated and precise information. Gastroenterology nurses are in the best position to concretely show IBD women the challenges they face and need to manage during the perinatal period. These gastroenterology specialists should integrate, as a routine care system, reproductive counseling, such as discussion about contraceptive methods and birth control, into education for IBD women of reproductive age and their families (Gawron et al., 2014). For example, gastroenterology specialists can provide IBD women and their partners with not only appropriate information about pregnancy, but also opportunities to participate in perinatal health education classes to come in contact with IBD peers, based on collaboration with other professionals including midwives and public health nurses. Such inter-professional care would play a pivotal role in caring for IBD women, and could help to create a favorable health care community for IBD women before their babies’ conception (Barber, 2008). Such an approach coincides with the research findings that pointed out the need for specific care for women with disabilities due to other chronic medical conditions (Corbin, 1987; Blackford et al., 2000; Aukamp and Sredl, 2004; Thompson et al., 2008).
The results of this study suggest that, in the case of long-term hospitalization during pregnancy because of IBD relapse, IBD women and their families have little or no chance to learn about childcare during the maternity stage, resulting in possible insufficient preparedness for parenthood including immediate postpartum childcare and mental stress. It is speculated that gastroenterology nurses may lack the understanding that women with IBD hospitalized for relapse should simultaneously prepare for motherhood, because gastroenterology nurses tend to manage IBD women as a medical model, while midwives tend to undervalue the disease course and management of IBD. A similar situation has often been criticized when pregnant women with complications or disabilities received multidisciplinary follow-up (Thierry, 2006; Piotrowski and Snell, 2007). Recently, although medical collaboration between gastroenterology and obstetrics has become standard policy for treatment of women with IBD, collaborative care by gastroenterology nurses/ midwives and community health professionals, including public health nurses, has lagged behind. Therefore, it is necessary to establish, as early as possible, a perinatal collaborative model for IBD women based on effective communication among gastroenterology nurses, midwives and community health professionals with a multidisciplinary team approach. Such an approach may include health education for IBD women such as methods of birth control, knowledge about the course and risks of IBD, breastfeeding care during hospitalization for IBD relapse, and care coordination in communities, and will improve the quality of life of women with IBD during the perinatal period.
On the other hand, previous studies suggested that IBD sufferers have a tendency to refrain from talking about their typical symptoms, such as fatigue, to health profes-sionals and even their own family members and friends (Beck et al., 2013; Hall et al., 2005). Gastroenterology nurses and midwives should focus on these tendencies, consider the health-related and learning needs of IBD women, and offer them opportunities to express their feelings or concerns during the perinatal period.
LIMITATIONS
This study has a few limitations. First, the fact that all interviews were conducted by the first author alone might have weakened the credibility of the findings. Second, the sample size was too small to generalize the findings to other populations. In particular, participants in this study may not present an average IBD mother as six of the eight relapsed during pregnancy, and four the perinatal period affects the results. Finally, age of their children at the interviews ranged from 7 month to 7 years old. Due to limitations within the interview surveys, there is some uncertainty whether interviewees have mixed memories with similar events when the answers involve past events or feelings. Consequently, we should plan the prospective research design to include interviews at some points from pregnancy to child rearing stage in the future.
CONCLUSION
Since IBD is often diagnosed during a woman’s reproductive years, gastroenterologists and obstetricians should cooperate with each other to routinely provide IBD women with reproductive counseling through individual or group education. Furthermore, we should establish, as early as possible, health care communities for women with IBD and their families, where good IBD control and health of IBD women can be maintained before pregnancy and during the perinatal period, based on multidisciplinary collaboration.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
ACKNOWLEDGEMENTS
The authors thank all the participants with IBD, and Mr. Tomotaka Akiyama, the representative of The Patient Association of Intractable Disease (Asebi-kai), for recruitment of participants.
REFERENCES
|
Alstead EM (2002). Inflammatory bowel disease in pregnancy. Postgrad. Med. J. 78(915):23–26. Crossref |
||||
|
Aukamp V, Sredl D (2004).Collaborative care management for a pregnant woman with an ostomy. Compl. Ther. Nurs. Midwif. 10(1):5–12. Crossref |
||||
|
Baiocco PJ, Korelitz BI (1984). The influence of inflammatory bowel disease and its treatment on pregnancy and fetal outcome. J. Clin. Gastroenterol. 6(3):211–216. Pubmed |
||||
|
Barber G (2008). Supporting pregnant women with disabilities. Pract. Nurse 19(7):330–334. Crossref |
||||
|
Beck A, Bager P, Jensen PE, Dahlerup JF (2013). How fatigue is experienced and handled by female outpatients with inflammatory bowel disease. Gastroenterol. Res. Pract. 1-8. Crossref |
||||
| Bernick S, Kane S (2010). Inflammatory Bowel Disease. In Diarrhea, Diagnostic and Therapeutic Advances (Guandalini S & Vaziri H eds.), Humana Press, New York. pp. 61–79. | ||||
|
Bernklev T, Jahnsen J, Henriksen M, Lygren I, Aadland E, Sauar J, Schulz T, Stray N, Vatn M, Moum B (2006).Relationship between sick leave, unemployment, disability, and health-related quality of life in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 12(5):402–412. Crossref |
||||
|
Blackford KA, Richardson H, Grieve S (2000). Prenatal education for mothers with disabilities. J. Adv. Nurs. 32(4):898–904. Crossref |
||||
|
Burnard P (1991). A method of analysing interview transcripts in qualitative research. Nurs. Educ. Today 11(6):461–466. Crossref |
||||
|
Coelho J, Beaugerie L, Colombel JF, Hébuterne X, Lerebours E, Lémann M, Baumer P, Cosnes J, Bourreille A, Gendre JP, Seksik P, Blain A, Metman EH, Nisard A, Cadiot G, Veyrac M, Coffin B, Dray X, Carrat F, Marteau P, CESAME Pregnancy Study Group (France) (2011). Pregnancy outcome in patients with inflammatory bowel disease treated with thiopurines: cohort from the CESAME Study. Gut 60(2):198–203. Crossref |
||||
|
Cooper JM, Collier J, James V, Hawkey CJ (2011). Living with inflammatory bowel disease:diagnosis during pregnancy. Gastrointest. Nurs. 9(5):28–34. Crossref |
||||
|
Corbin JM (1987). Women's perceptions and management of a pregnancy complicated by chronic illness. Health Care Women Int. 8(5-6):317–337. Crossref |
||||
|
Elo S, Kyngäs H (2008). The qualitative content analysis process. J. Adv. Nurs. 62(1):107–115. Crossref |
||||
|
Fletcher PC, Schneider MA (2006). Is there any food I can eat? Living with inflammatory bowel disease and/or irritable bowel syndrome. Clin. Nurse Spec. 20(5):241–247. Crossref |
||||
|
Fletcher PC, Schneider MA, Van Ravenswaay V, Leon Z (2008). I am doing the best that I can!: Living with inflammatory bowel disease and/or irritable bowel syndrome (part II). Clin. Nurse Spec. 22(6): 278–285. Crossref |
||||
|
Gawron LM, Hammond C, Keefer L (2014). Documentation of reproductive health counseling and contraception in women with inflammatory bowel diseases. Patient Educ. Couns. 94(1):134–137. Crossref |
||||
|
Graff LA, Walker JR, Lix L, Clara I, Rawsthorne P, Rogala L, Miller N, Jakul L, McPhail C, Ediger J, Bernstein CN (2006). The relationship of inflammatory bowel disease type and activity to psychological functioning and quality of life. Clin. Gastroenterol. Hepatol. 4(12):1491–1501. Crossref |
||||
|
Graneheim UH, Lundman B (2004). Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 24(2):105–112. Crossref |
||||
|
Guassora AD, Kruuse C, Thomsen OO, Binder V (2000). Quality of life study in a regional group of patients with Crohn disease. A structured interview study. Scand. J. Gastroenterol. 35(10):1068–1074. Crossref |
||||
| Guba EG, Lincoln YS (1994). Competing paradigms in qualitative research. In: Handbook of qualitative research (Denzin NK & Lincoln YS eds.), Sage, Thousand Oaks, CA. pp.105–117. | ||||
|
Habal FM, Kapila V (2009). Inflammatory bowel disease and pregnancy: evidence, uncertainty and patient decision-making. Can. J. Gsatroenterol. 23(1):49–53. Pubmed |
||||
|
Habal FM, Huang VW (2012). A decision-making algorithm for the management of pregnancy in the inflammatory bowel disease patient. Aliment Pharmacol. Ther. 35(5): 501–515. Crossref |
||||
|
Hall NJ, Rubin GP, Dougall A, Hungin AP, Neely J (2005). The fight for 'health-related normality': a qualitative study of the experiences of individuals living with established inflammatory bowel disease (IBD). J. Health. Psychol. 10(3):443–455. Crossref |
||||
|
Jäghult S, Saboonchi F, Johansson UB, Wredling R, Kapraali M (2011). Identifying predictors of low health-related quality of life among patients with inflammatory bowel disease: comparison between Crohn's disease and ulcerative colitis with disease duration. J. Clin. Nurs. 20(11-12):1578–1587. Crossref |
||||
|
Kane S (2002). Gender issues in the management of inflammatory bowel disease and irritable bowel syndrome. Int. J. Fertil. Women M. 47(3):136–142. Pubmed |
||||
| Kuwahara E, Asakura K (2013). The epidemiology and etiology of inflammatory bowel disease - The epidemiology of inflammatory bowel disease. Stomach Intestine 48(5 Suppl):547–553. | ||||
|
Lix LM, Graff LA, Walker JR, Clara I, Rawsthorne P, Rogala L, Miller N, Ediger J, Pretorius T, Bernstein CN (2008). Longitudinal study of quality of life and psychological functioning for active, fluctuating, and inactive disease patterns in inflammatory bowel disease. Inflamm. Bowel Dis. 14(11):1575–1584. Crossref |
||||
|
McCormick JB, Hammer RR, Farrell RM, Geller G, James KM, Loftus EVJr, Mercer MB, Tilburt JC, Sharp RR (2012). Experiences of patients with chronic gastrointestinal conditions: in their own words. Health Qual. Life. Outcomes 10(1):1-11. Crossref |
||||
|
Mallett SJ, Lennard-Jones JE, Bingley J, Gilon E (1978). Colitis. Lancet. 2(8090):619–621. Crossref |
||||
|
Marri SR, Ahn C, Buchman AL (2007) .Voluntary childlessness is increased in women with inflammatory bowel disease. Inflamm. Bowel Dis. 13(5):591–599. Crossref |
||||
|
Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff G, Benchimol EI, Panaccione R, Ghosh S, Barkema HW, Kaplan GG (2012). Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 142(1):46–54. Crossref |
||||
|
Mountifield R, Bampton P, Prosser R, Muller K, Andrews JM (2009). Fear and fertility in inflammatory bowel disease: a mismatch of perception and reality affects family planning decisions. Inflamm. Bowel Dis. 15(5):720–725. Crossref |
||||
|
Mukherjee S, Sloper P, Turnbull A (2002). An insight into the experiences of parents with inflammatory bowel disease. J. Adv. Nurs. 37(4):355-363. Crossref |
||||
|
Piotrowski K, Snell L (2007). Health needs of women with disabilities across the lifespan. J. Obstet. Gynecol. Neonatal Nurs. 36(1):79–87. Crossref |
||||
|
Reddy D, Murphy SJ, Kane SV, Present DH, Kornbluth AA (2008). Relapses of inflammatory bowel disease during pregnancy: in-hospital management and birth outcomes. Am. J. Gastroenterol. 103(5):1203–1209. Crossref |
||||
|
Steinlauf AF, Present DH (2004). Medical management of the pregnant patient with inflammatory bowel disease. Gastoroenterol. Clin. North Am. 33(2):361–385. Crossref |
||||
| Takebayashi T, Nishiwaki Y (2007). Current status of epidemiology of IBD in Japan. In Recent Advances in Inflammatory Bowel Disease (Hibi T ed.), Elsevier Japan, Tokyo. pp. 143–165. | ||||
|
Thierry JM (2006). The importance of preconception care for women with disabilities. Matern. Child Nurs. J. 10(5 Suppl):S175–176. Crossref |
||||
|
Thompson D, Thomas H, Solomon J, Nashef L, Kendall S (2008). Chronic illness, reproductive health and moral work: women's experiences of epilepsy. Chronic Illness 4(1): 54–64. Crossref |
||||
|
Walsh-Gallagher D, Sinclair M, Mc Conkey R (2012). The ambiguity of disabled women's experiences of pregnancy, childbirth and motherhood: a phenomenological understanding. Midwifery 28(2): 156–162. Crossref |
||||
|
Willoughby CP, Truelove SC (1980). Ulcerative colitis and pregnancy. Gut 21(6): 469–474. Crossref |
||||
|
Wong A (2000): The work of disabled women seeking reproductive health care. Sex Disabil. 18(4): 301–306. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


