ABSTRACT
Premenstrual symptoms are gradually becoming recognized socially and measures taken to cope with premenstrual symptoms are changing. The purpose of this study was to determine the differences in degree of recognition, in physical and emotional symptoms and in means for coping with premenstrual symptoms between nursing students and their mothers at the ages of the nursing students. This study was conducted between July and November, 2016. 272 nursing students and 272 mothers of the students were recruited. This study was approved by the Ethics Committee of Tokushima University Hospital. A self-administered questionnaire that took about 15 min to complete was designed. The proportion of students who recognized premenstrual symptoms was 98% and the proportion of mothers who recognized premenstrual symptoms at the same age as the students was 76%. The proportions of students who had moderate to severe physical and emotional symptoms were higher than those of the mothers. The items with the highest percentages of students and mothers who answered moderate to severe physical and emotional symptoms were desire for sweets and irritability, respectively. The proportion of students who took measures to cope with premenstrual symptoms was higher than that of the mothers. Physical symptoms in the students were significantly correlated with those in their mothers. The degrees of physical and emotional symptoms in the students were greater than those in the mothers at the same age as the students and measures taken for coping with these symptoms were diversified. The increasing availability of information on premenstrual symptoms and changes in lifestyle may contribute to the increase in prevalence of premenstrual symptoms.
Key words: Premenstrual symptoms, coping, nursing students, mothers.
Many women of reproductive age experience physical or emotional symptoms associated with the menstrual cycle. Premenstrual syndrome (PMS) is a cluster of mood, behavioral and physical symptoms occurring during the late luteal phase of the menstrual cycle that interfere with daily activities and are relieved by the onset of menstruation (Yonkers et al., 2008). It has been reported that the frequency of premenstrual symptoms is quite high (80-90%) (Angst et al., 2001) and that about 5% of women have severe symptoms that interfere with personal or social relationships or work and may require pharmacological management (Dimmock et al., 2000). In Japan, it has been reported that 95% of women aged 20 to 49 years suffered from premenstrual symptoms (Takeda et al., 2006) and that 64.8% of high school students suffered from premenstrual symptoms (Takeda et al., 2010).
The etiology of PMS has remained unknown, although hormonal changes and serotonin dysregulation have been suggested (Grady-Weliky, 2003). Lifestyle factors such as diet, exercise and sleep are considered to be involved. A potential role of dietary fat in premenstrual symptoms in Japanese women has been proposed (Nagata et al., 2004). Relationships of PMS with calcium intake, caffeine-containing beverages and chocolate or sweets containing refined sugar have also been reported (Tadakawa et al., 2016). Tadakawa et al. (2016) reported that a preference for salty food and a lack of regular exercise were identified in girls aged 15 to 19 years with physical premenstrual symptoms as risk factors for school absenteeism. It has been reported that exercise could be used as treatment for premenstrual disorders, suggesting that there is an association between PMS and lack of exercise (Daley, 2009). Skipping breakfast, insufficient sleeping and insufficient exercise were suggested to be exacerbation factors of PMS (Ogata and Daitou, 2013; Mori et al., 2004). Sakuma et al. (2008) reported that no feeling of fatigue when getting up, sufficient sleeping and appropriate exercise were associated with mild degrees of premenstrual symptoms. Considering the current lifestyles of young women, the prevalence of PMS may gradually increase.
Premenstrual symptoms and PMS had not been recognized as health concerns in Japan. However, premenstrual symptoms have gradually become recognized due to the availability of information regarding premenstrual symptoms. Lifestyle modifications including regular exercise, avoidance of stressful events, adjustment of sleeping habits, cognitive behavior therapy and dietary supplementation as well as pharmacological treatments have been proposed for coping with premenstrual symptoms (Ryu and Kim, 2015). However, the means of coping with premenstrual symptoms may have changed with times. The degree of recognition of symptoms, the physical and emotional symptoms, and coping strategies may be different for young women at present and their mothers at young ages because of differences in life style, background knowledge of symptoms and means for coping.
Premenstrual syndrome experienced by premenopausal women greatly interferes with the quality of life (Rapkin and Winer, 2009). Bertone-Johnson et al. (2015) showed in a prospective study that women who experienced moderate to severe PMS had a 40% higher risk of developing hypertension than did women who experienced few premenstrual symptoms. Symptoms such as hypersomnia and general fatigue in the daytime may increase since it has been reported that the quality of night sleeping deteriorated before menstruation (Baker and Driver, 2004). It has been reported that restriction of sleeping hours and disturbance of deep sleep induce insulin resistance (Tasali et al., 2008), suggesting that sleeping disorder due to premenstrual symptoms may be involved in the occurrence of diabetes mellitus.
The purpose of this study was to determine the differences in degree of recognition in physical and emotional symptoms and in the means for coping with premenstrual symptoms between nursing students and their mothers at the ages of the nursing students.
This study was conducted between July and November in 2016. 272 nursing students (66 first grade, 67 second grade, 71 third grade and 68 fourth grade students) and 272 mothers of the nursing students were recruited. The nursing students for whom agreement could be obtained were asked to complete a questionnaire after explanation of the study at the end of a lecture, and questionnaires were collected on the same day. Subsequently, invitation letters and questionnaires were mailed to their mothers through the nursing students for whom agreement had been obtained. The participants were informed of the purposes and procedure of the study in the invitation letter. It was stated in the invitation letter that cooperation in the questionnaire survey is based on free will and that there is no advantage for the subjects who do not cooperate. Agreement for participation in this study was obtained by having the questionnaire form returned by mail. The same connection numbers on the questionnaire forms we used for a nursing student and her mother. Each nursing student was asked to send her mother an envelope containing a questionnaire form with the same connection number as that on the nursing student’s questionnaire form. The questionnaire forms from the students and their mothers were anonymous, and questionnaire forms from the mother and her daughter could be identified by same connection numbers. Sufficient considerations were given to private information. This study was approved by the Ethics Committee of Tokushima University Hospital (2625).
A self-administered questionnaire that took about 15 min to complete was designed. The first part of the questionnaire consisted of questions on age, body height and weight, past history of hypertension, menstrual status including age of menarche, menstrual regularity and menstrual cycle, and degree of dysmenorrhea assessed by using a visual analogue scale (VAS). The second part of the questionnaire consisted of questions on recognition of premenstrual symptoms including PMS and physical symptoms beginning within 5 days before menstruation, including abdominal tension and pain, bloating, breast swelling and tenderness, headache, low back pain, hot flashes, rough skin, fatigue or lack of energy, overeating, food cravings/desire for sweets, hypersomnia, insomnia, constipation and diarrhea, and psychological symptoms including irritability, anger, anxiety, depressed mood, decreased interest in social relationships, and confusion/out of control. Items were rated as “not at all”, “mild”, “moderate”, or “severe”. The third part of the questionnaire consisted of questions on coping with premenstrual symptoms: lying down, warming the lower back and lower abdomen, having a massage, visiting a gynecologist, taking medicines, consulting somebody, appropriate exercise, sufficient sleeping, doing something to take one’s mind off the symptoms, refraining from favorite food and caffeine, restricting intake of water and salt, and telling somebody that one is now before menstruation. The mothers were asked to answer the questions based on their memory at the same age as their daughters.
Statistical analysis
Statistical analyses for data evaluation were carried out using SPSS version 20 for Windows. All p values are two-tailed and those less than 0.05 were considered to be statistically significant. The significance of differences in the degree of premenstrual symptoms between the students and their mothers was evaluated by the Wilcoxon rank sum test. Physical and emotional symptoms were scored according to the degree of symptoms (severe: 4 points; moderate such as having an impact on daily life: 3 points; a little: 2 points, and no symptom: 1 point) and total points of 14 physical symptoms and 6 emotional symptoms were calculated. Spearman’s correlation test was used for the correlation between the students and their mothers in physical and emotional symptoms. Scores of physical and emotional symptoms in the mothers with and those without hypertension were assessed by using the Mann-Whitney U test.
The response rates of the questionnaire were 93.0% (253 /272) in the students and 59.9% (163/272) in their mothers. Mean (± standard deviation: SD) ages of the students and their mothers were 20.1 ± 1.8 and 49.8 ± 4.1 years old, respectively. Mean body heights, body weights and body mass indices (BMIs) were 157.5 ± 4.9 cm, 50.9 ± 5.9 kg and 20.5 ± 2.1, respectively, in the students and 157.9 ± 4.9 cm, 53.7 ± 7.5 kg and 21.5 ± 2.7, respectively, in their mothers.
As is shown in Table 1, age of menarche in the students was significantly younger than that in their mothers. The proportion of students with an irregular menstrual cycle tended to be larger than the proportion of mothers with an irregular menstrual cycle at the same age as the students. The proportion of students who had menstrual pain was significantly larger than that of the mothers who had menstrual pain at the same age as the students. The mean score of VAS in the students was significantly higher than that in their mothers.
Four students had a past history of hypertension. Twenty-five mothers had a past history of hypertension and 15 mothers had taken anti-hypertensive drugs. Scores of physical symptoms and emotional symptoms were not significantly different in the mothers with and those without hypertension (p=0.575 and p=0.876, respectively).
Proportion of women who recognize premenstrual symptoms
The proportion of students who recognize premenstrual symptoms was 98%. The proportion of mothers who had recognized premenstrual symptoms at the same age as the students was 76%, and the proportion of mothers who now recognize premenstrual symptoms was 98%.
Physical and emotional symptoms in the students and the mothers at the same age as the students
The mean (± SD) numbers of moderate to severe physical symptoms and emotional symptoms in the students were 2.6 ± 2.4 and 1.7 ± 1.0, respectively. The mean (± SD) numbers of moderate to severe physical symptoms and emotional symptoms in the mothers at the same age as the students were 1.4 ± 0.85 and 0.75 ± 0.25, respectively. Both the number of physical symptoms and the number of emotional symptoms in the students were significantly larger than those in the mothers at the same age as the students (p<0.001).
As shown in Table 2, the item with the highest percentage of students who answered moderate to severe in physical symptoms was desire for sweets, followed by overeating and hypersomnia. The item with the highest percentage of mothers who answered moderate to severe symptoms was desire for sweets, followed by overeating. The degrees of physical symptoms including bloating, hot flashes, rough skin, general fatigue, hypersomnia, overeating and desire for sweets in the students were significantly greater than those in the mothers at the same age as the students.


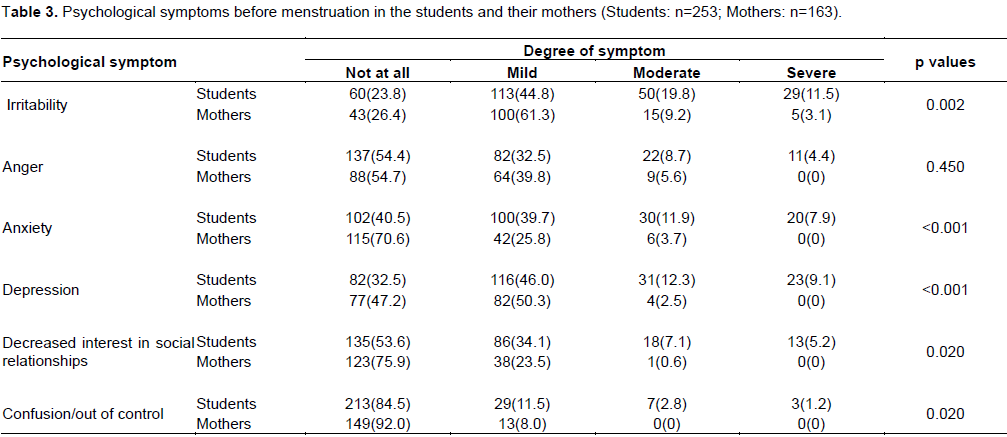
As shown in Table 3, the item with the highest percentage of students who answered moderate to severe in emotional symptoms was irritability, followed by depression and anxiety. The item with the highest percentage of mothers who answered moderate to severe in emotional symptoms was irritability. The degrees of emotional symptoms including irritability, anxiety, depression, decreased interest in social relationships and confusion in the students were significantly greater than those in the mothers at the same age as the students.
Correlations between premenstrual symptoms between students and their mothers
Physical symptoms in the students were significantly correlated with those in the mothers at the same age as the students (r=0.199, p=0.012), but emotional symptoms in the students were not correlated with those in their mothers (r=0.093, p=0.240).
Coping with premenstrual symptoms
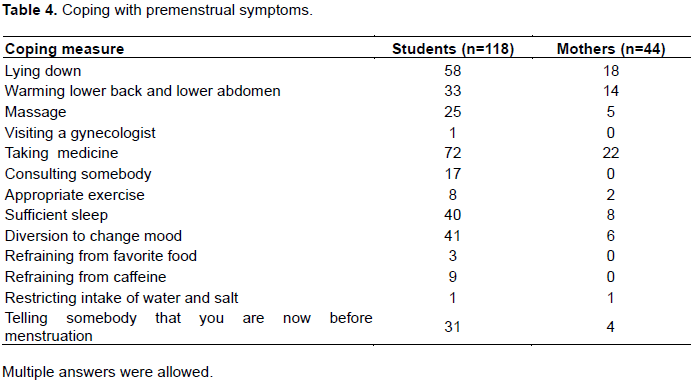
The proportion of the students who took measures to cope with premenstrual symptoms (54%) was higher than that of the mothers (29%). The measures taken to cope with premenstrual symptoms are shown in Table 4. The measures taken to cope with premenstrual symptoms were diversified in the students. The proportions of both students and mothers who answered “taking medicine” and “lying down” were high. The proportions of students who answered "consulting somebody" and "telling somebody that I am now before menstruation" were high. All of the 22 mothers who had taken medicine had used analgesic agents. Seventy-two students had used medicine, and 65 (90%) of the 72 students had taken analgesic agents as medicine. The students also used Japanese herbal medicines (8%), oral contraceptives (6%) and supplements (3%).
In the present study, it was shown that the proportions of students who had moderate to severe physical symptoms and emotional symptoms were higher than those of the mothers at the same age as the students and that the degrees of the symptoms in the students were significantly greater than those in the mothers at the same age as the students. Physical symptoms in the students were significantly correlated with those in the mothers at the same age as the students. The proportion of students who took measures to cope with premenstrual symptoms was higher than that of the mothers at the same age as the students.
It was confirmed that the rate of recognition of premenstrual symptoms including PMS was extremely high (98%). Ogata and Daitou (2013) reported that the proportion of nursing students who recognized PMS was only 18.6% in the first grade but increase with advance of grade and reached 69.6% in nursing students in the fourth grade. Recognition of PMS by a high proportion of nursing students might be due to a high level of awareness of health care. Sakuma et al. (2008) reported that not only knowledge of menstrual disorders including premenstrual symptoms but also knowledge of health care was insufficient in non-medical vocational school students. Possible reasons for the relatively high rate of recognition in the nursing students’ mothers are that the mothers obtained medical information through their daughters as nursing students and that the proportion of mothers working as medical staff was high.
It was shown that the proportions of nursing students with bloating, general fatigue, desire for sweets, overeating and hypersomnia in physical symptoms and with irritability and depression in emotional symptoms were high. In Iranian university students, the most common symptoms were tiredness, depression and anxiety in emotional symptoms and backache and bloating in physical symptoms (Bakhshani et al., 2009). Another study showed that mood lability, anger and sadness were the most frequent emotional symptoms and that acne was the most frequent physical symptom (Lajoie and Desindes, 2002). The most frequent symptoms in Turkish medical students were bloating, irritability and breast tenderness (Goker et al., 2015). The frequencies of physical symptoms in the present study were rather low compared to those in a previous study (Czajkowska et al., 2015). The differences in physical symptoms may be due to differences in race and lifestyle.
Compared to the results of a previous study for Japanese high school students, the frequencies of overeating, irritability, depression and decreased interest in social relationships were high in the present study (Takeda et al., 2010). In addition, compared to the results of a previous study for Japanese women whose mean age was 36 years, the frequencies of overeating, depression, decreased interest in social relationships, fatigue and hypersomnia were high in the present study (Takeda et al., 2006). The symptoms may change with advance in age.
The symptoms with significant differences between the students and mothers at the same age as the students were bloating, hot flashes, rough skin, general fatigue, hypersomnia, overeating and desire for sweets in physical symptoms and irritability, anxiety, depression, decreased interest in social relationships and confusion in emotional symptoms. The reasons for the differences are an increase in the general recognition of symptoms and availability of information on premenstrual symptoms. Students nowadays freely talk about premenstrual symptoms with their friends. However, their mothers about 30 years ago did not have opportunities to talk about menstrual disorders with their friends because of a lack of understanding of the symptoms. About 30 years ago Japanese women might have suppressed verbal expression of premenstrual symptoms in order to promote maintenance of social harmony.
According to the National Health and Nutrition Examination survey in 2014, the proportion of women aged 20 to 29 years who skipped breakfast was 23%, which was highest among all age groups, and the proportion of women aged 20 to 29 years who regularly did exercise was 10.1%, which was lowest among all age groups. Otsuka et al. (2015) reported that irregular sleeping was a risk factor for deterioration of premenopausal symptoms. Also, the proportion of women aged 20 to 29 years, whose sleeping time was less than 6 h was 45.1% in 2015, which was higher than the proportion in 2007, and the proportion of women aged 20 to 29 years who could not get adequate rest due to sleep disturbance was 24.5% in 2014, which was higher than that in 2012 (Ministry of Health, Labour and Welfare. National Health and Nutrition Examination survey, 2014). Thus, lifestyle has become irregular compared with that in the past. In addition, the proportion of women in whom psychological stress in daily life affected premenopausal symptoms was significantly higher for women being treated for PMS, suggesting that psychological stress as well as an irregular lifestyle were involved in the occurrence of PMS (Koda et al., 2012). According to the comprehensive survey of living conditions, the proportion of women who were suffering from stress (43.2%) in 1995 increased to 52.2% in 2013 (MHLW, 2013), and the proportion of women aged 20 to 29 years who were suffering from stress was 54.4%. The irregular lifestyle and increase in psychological stress may be involved in the intergenerational differences in degrees and types of premenstrual symptoms between the students and their mothers.
It was shown that measures taken to cope with premenstrual symptoms were diversified. Women can easily obtain information on coping with premenstrual symptoms through the internet. Also, various pharmacological treatments for PMS including treatments with oral contraceptives, selective serotonin reuptake inhibitors and gonadotropin-releasing hormone analogues have become available (Ryu and Kim, 2015). Students can get information on treatments for premenstrual symptoms through the internet, but they might easily believe the information without evidence. Selection of appropriate information regarding health care is needed. Communication with family and friends may also be needed. Exercise may improve emotional and physical premenstrual symptoms by increasing physical well-being (Delara et al., 2012). A previous study revealed beneficial effects of exercise on physical symptoms including breast tenderness and bloating (Daley, 2009). However, it was pointed out in that report that evidence-based recommendation regarding the effectiveness of exercise is needed because of the small sample size and low methodological quality in the study (Daley, 2009).
In the present study, a weak correlation was found between physical symptoms, but not between emotional symptoms, in the students and their mothers. Further study on predisposition of physical symptoms is needed. Ogata and Daitou (2013) reported that lifestyle-related factors such as no exercise habit, skipping breakfast, no mood change and short sleeping time were significantly associated with emotional symptoms. The fact that emotional symptoms are affected by individual lifestyle might be the reason for no correlation being found between emotional symptoms in the students and their mothers.
Derman et al. (2004) reported that there was an association between dysmenorrhea and PMS in adolescent girls aged 10 to 17 years and that 71% of the girls with dysmenorrhea had PMS. Kitamura et al. (2012) also reported that the prevalence rate of moderate to severe PMS increased with increase in the severity of dysmenorrhea. The reason for the correlation between PMS and dysmenorrhea has not been clarified. Prostaglandin (PG) may have a role in the biochemical etiologies in both PMS and dysmenorrhea. It has been reported that PGE2 and its receptor mediated elevated anxiety and social avoidance induced by repeated social defeat through attenuating a stress-coping action of the meso-prefrontal dopaminergic pathway (Tanaka et al., 2012). Haack et al. (2009) reported that increase in PGE2 metabolite levels in response to sleep loss was associated with the degree to which participants in their study reported spontaneous pain complaints. Lifestyle-related factors may influence both PMS and dysmenorrhea. It has been reported that the proportions of women with dysmenorrhea who skipped lunch and had a short sleeping time were significantly higher than those in women without dysmenorrhea (Yuasa et al., 2013). In the present study, the proportion of students with dysmenorrhea was higher than that of the mothers who had dysmenorrhea at the same age as the students, and the degree of pain in the students was higher than that in their mothers. Unfortunately, in the study questions regarding lifestyle were not asked so the association of lifestyle with dysmenorrhea could not be clarified.
This study has several limitations. A self-administered questionnaire was used to assess premenstrual symptoms. Therefore, the reliability of answers could not be verified. The recall bias of the mothers is of a serious nature. Retrospective recall regarding premenstrual symptoms at the time when mothers were about 20 years old is a limitation of this study. Since the contexts of behavior during menstruation may be changed by large time gaps, comparison between the nursing students and their mothers may not be valid. The subjects in this study were nursing students, who have basic medical knowledge. Therefore, further study in non-medical students is needed. The reasons for the drop-out were not known for there was no response on that since this study was a questionnaire survey. The results for the mothers who did not return the questionnaire form might be significant.
The degrees of physical symptoms and emotional symptoms in the students were greater than those in the mothers at the same age as the students, and measures taken to cope with these symptoms were diversified. The increasing availability of information on premenstrual symptoms and changes in lifestyle may contribute to the increase in prevalence of premenstrual symptoms.
The authors have not declared any conflict of interests.
REFERENCES
|
Angst J, Sellaro R, Stolar M, Merikangas KR, Endicott J (2001). The epidemiology of perimenstrual psychological symptoms. Acta Psychiatr. Scand. 104:110-116.
Crossref
|
|
|
|
Baker FC, Driver HS (2004). Self-reported sleep across the menstrual cycle in young, healthy women. J. Psychosom. Res. 56:239-243.
Crossref
|
|
|
|
|
Bakhshani NM, Mousavi MN, Khodabandeh G (2009). Prevalence and severity of premenstrual symptoms among Iranian female university students. J. Pak. Med. Assoc. 59:205-208.
|
|
|
|
|
Bertone-Johnson EB, Whitcomb BW, Rich-Edwards JW, Hankinson SE, Manson JE (2015). Premenstrual syndrome and subsequent risk of hypertension in a prospective study. Am. J. Epidemiol. 182:1000-1009.
Crossref
|
|
|
|
|
Czajkowska M, Drosdzol-Cop A, Galazka I, Naworska B, Skrzypulec-Plinta V (2015). Menstrual cycle and the prevalence of premenstrual syndrome/premenstrual dysphoric disorder in adolescent athletes. J. Pediatr. Adolesc. Gynecol. 28:492-498.
Crossref
|
|
|
|
|
Daley A (2009). Exercise and premenstrual symptomatology: a comprehensive review. J. Womens Health 18:895-899.
Crossref
|
|
|
|
|
Delara M, Ghofranipour F, Azadfallah P, Tavafian SS, Kazemnejad A, Montazeri A (2012). Health related quality of life among adolescents with premenstrual disorders: a cross sectional study. Health Qual. Life Outcomes 10(1):1.
Crossref
|
|
|
|
|
Derman O, Kanbur NO, Tokur TE, Kutluk T (2004). Premenstrual syndrome and associated symptoms in adolescent girls. Eur. J. Obstet. Gynecol. Reprod. Biol. 116(2):201-206.
Crossref
|
|
|
|
|
Dimmock PW, Wyatt KM, Jones PW, O'Brien PM (2000). Efficacy of selective serotonin-reuptake inhibitors in premenstrual syndrome: a systematic review. Lancet 356:1131-1136.
Crossref
|
|
|
|
|
Goker A, Artunc-Ulkumen B, Aktenk F, Ikiz N (2015). Premenstrual syndrome in Turkish medical students and their quality of life. J. Obstet. Gynaecol. 35:275-278.
Crossref
|
|
|
|
|
Grady-Weliky TA (2003). Clinical practice. Premenstrual dysphoric disorder. N. Engl. J. Med. 348:433-438.
Crossref
|
|
|
|
|
Haack M, Lee E, Cohen D, Mullington JM (2009). Activation of the prostaglandin system in response to sleep loss in healthy humans: Potential mediator of increased spontaneous pain. Pain 145:136-141.
Crossref
|
|
|
|
|
Kitamura M, Takeda T, Koga S, Nagase S, Yaegashi N (2012). Relationship between premenstrual symptoms and dysmenorrhea in Japanese high school students. Arch. Womens Ment. Health 15:131-133.
Crossref
|
|
|
|
|
Koda C, Takahashi M, Koda K, Sadamoto K (2012). Differences in premenstrual symptoms and life styles between healthy women and patients diagnosed with premenstrual syndrome. J. Jpn. Soc. Psychosom Obstet. Gynecol. 17:112-120.
|
|
|
|
|
Lajoie F, Desindes S (2002). Improving treatment for premenstrual syndrome. Can. J. CME 14(8):81-94.
|
|
|
|
|
Ministry of Health, Labour and Welfare (MHLW) (2013). Comprehensive survey of living conditions, 2013. Available at:http://www1.mhlw.go.jp/toukei/ksk/htm/ksk016.html
|
|
|
|
|
Ministry of Health, Labour and Welfare. National Health and Nutrition Examination survey (2014).
|
|
|
|
|
Mori K, Kawase K, Yoshizaki A, Wada M, Matsumoto S (2004). A study of premenstrual syndrome in mature Japanese women and their life-styles. J. Jpn. Soc. Psychosom. Obstet. Gynecol. 9:134-145.
|
|
|
|
|
Nagata C, Hirokawa K, Shimizu N, Shimizu H (2004). Soy, fat and other dietary factors in relation to premenstrual symptoms in Japanese women. BJOG 111:594-599.
Crossref
|
|
|
|
|
Ogata T, Daitou M (2013). The study on the actual situation of female college student's premenstrual syndrome and their personal lifestyle and self-care. J. Kyushu Univ. Nurs. Soc. Welfare 13(1):57-65.
|
|
|
|
|
Otsuka Y, Takahara M, Sakuragi S (2015). Risk Factors Related to the Onset and Aggravation of Premenstrual Syndrome. Bull. Aichi Univ. Educ. 64:27-31.
|
|
|
|
|
Rapkin AJ, Winer SA (2009). Premenstrual syndrome and premenstrual dysphoric disorder: quality of life and burden of illness. Expert Rev. Pharmacoecon Outcomes Res. 9(2):157-70.
Crossref
|
|
|
|
|
Ryu A, Kim TH (2015). Premenstrual syndrome: A mini review. Maturitas 82:436-440.
Crossref
|
|
|
|
|
Sakuma Y, Kanoya Y, Ishimitsu F, Hosona M, Mochizuki Y, Sato C (2008). The Factors Affecting Premenstrual and Menstrual Symptoms Among Young Women-Comparison of the Lifestyle/Health Behavior in Nursing Students and Non-medical Vocational School Student. J. Jpn. Soc. Nurs. Res. 31(2):25-36.
|
|
|
|
|
Tadakawa M, Takeda T, Monma Y, Koga S, Yaegashi N (2016). The prevalence and risk factors of school absenteeism due to premenstrual disorders in Japanese high school students –a school-based cross sectional study. Biol. Psychol. Soc. Med. 10:13.
Crossref
|
|
|
|
|
Takeda T, Koga S, Yaegashi N (2010). Prevalence of premenstrual syndrome and premenstrual dysphoric disorder in Japanese high school students. Arch. Womens Ment. Health 13:535-537.
Crossref
|
|
|
|
|
Takeda T, Tasaka K, Sakata M, Murata Y (2006). Prevalence of premenstrual syndrome and premenstrual dysphoric disorder in Japanese women. Arch. Womens Ment. Health 9:209-212.
Crossref
|
|
|
|
|
Tanaka K, Furuyashiki T, Kitaoka S, Senzai Y, Imoto Y, Segi-Nishida E, Deguchi Y, Breyer RM, Breyer MD, Narumiya S (2012). Prostaglandin E2-mediated attenuation of mesocortical dopaminergic pathway is critical for susceptibility to repeated social defeat stress in mice. J. Neurosci. 32:4319-4329.
Crossref
|
|
|
|
|
Tasali E, Leproult R, Ehrmann DA, Van Cauter E (2008). Slow-wave sleep and the risk of type 2 diabetes in humans. Proc. Natl. Acad. Sci. USA 105:1044-1049.
Crossref
|
|
|
|
|
Yonkers KA, O'Brien PMS, Eriksson E (2008). Premenstrual syndrome. Lancet 371:1200-1210.
Crossref
|
|
|
|
|
Yuasa Y, Kobayashi Y, Niibori T, Hatsushika S, Akedo Y (2013). Examination of the lifestyle-related factors affecting on menstrual symptoms. Int. J. Hum. Cult. Stud. 23:282-286
Crossref
|
|