Full Length Research Paper

ABSTRACT
Globally, postpartum care is a neglected part of maternal health, even though 50% of maternal deaths occur in the first weeks after childbirth. Literature is sparse on the quality and content of postnatal care provided in Nigeria. This study aimed to assess the quality of Postnatal Care (PNC) for mothers using the World Health Organization (WHO) practice guideline of postnatal care. An exploratory cross-sectional design was employed among 57 purposively selected mothers in postnatal clinic and wards. Data were collected in two phases using three checklists to examine facility resources and quality of postnatal care provided; and one questionnaire to evaluate mothers’ satisfaction in both the clinic and the wards. Data were analyzed using descriptive statistics. The facility assessment showed an inadequate infrastructure and human resources. Only 47.9% of the recommended routine postnatal care was provided on the postnatal wards and 42.3% in the postnatal clinic. Level of satisfaction was found to be poor among 63.2% of the women on the wards, and good among 82.5% of the women in the clinic. Findings suggest that inadequate resources for PNC. Organizations need to strengthen PNC services by providing recommended resources and a standard guideline that will serve as a framework for provision of quality postnatal care services.
Key words: Postnatal care, postnatal care guideline, quality care, maternal satisfaction.
INTRODUCTION
The postnatal period is the first six weeks after birth, which is critical to the health and survival of the mother and her newborn. The most vulnerable time for both is during the hours and days after birth (WHO, 2014). Despite this long-standing definition, the postpartum period frequently lasts for several months and it is documented as a neglected aspect of modern maternity care. Accordingly, Pallangyo et al. (2017), reported that the global picture confirms that postpartum care is a neglected part of maternal and neonatal health, yet 50% of maternal deaths occur in the first weeks after childbirth. It is therefore not surprising that literature is sparse on the puerperium and where it exists; it deals primarily with abnormal involution and pathology (Kearns et al., 2016). The WHO has highlighted widespread and persistent health problems, including death experienced by women after childbirth, many of which are unreported by women and not identified by healthcare professionals (WHO, 2014). Furthermore, WHO (2014) reports that of the 289,000 maternal deaths that occur each year, worldwide and 50 to 71% occur within the postnatal period. Unfortunately, 99% of these maternal deaths occur in low and middle income countries including Nigeria (Blencowe et al., 2012).
Despite the more than 20 years fight against maternal deaths, Nigeria still documents one of the worst maternal mortality statistics in the world. With a maternal mortality ratio of 576 per 100,000 live births, Nigeria is second only to India in the global estimates of maternal mortality.
Consequently, Nigeria loses about 153 women of childbearing age every day and a woman’s chance of dying from pregnancy and childbirth in Nigeria is 1 in 13 (NDHS, 2013). Specifically, over 40,000 maternal deaths occur in Nigeria yearly (APHRC, 2017). Reports from other low income countries such as Uganda also suggest poor Postnatal Care (PNC) services. There is no document to suggest an adapted standard for PNC services in Nigeria. However, effort is geared towards achieving the recommended standard specified by the WHO.
Khanal et al. (2014), reported that the postnatal care indicated that standards were infrequently met as only 2 in 5 women in their study were reported to have received a postnatal check-up within one hour of delivery. In another study in Pakistan, Munawar et al. (2017) revealed verbalization of the low quality of maternity care by most of the participants.
In Nigeria an extensive review of the literature suggests a dearth of researches on the content and quality of postnatal care, even though care is routinely provided for women. However, several important indicators such as mortality indices reported from recent studies raise concern about its quality and effectiveness, consequently the question of quality and coverage.
Accordingly, Kinney et al. (2010) reiterates that the burden of maternal death can effectively be reduced when efforts are geared towards overcoming both the coverage and quality gaps in postnatal care. This is also consistent with other reports. For example, Carvajal-Aguirre et al. (2017) in an audit review of the content of ANC and PNC services concluded that the gap between coverage and content as a measure of quality of care is tremendously wide in all countries.
Therefore, in order to accelerate maternal and newborn survival, the authors suggested an urgent need for increased efforts targeted at improving both the coverage and actual contents of maternal and newborn health interventions.
In response to the morbidity and mortality indices, the WHO in 2014 established guidelines of postnatal care, to promote quality and ensure effectiveness. Again in 2016 the organization indorsed the availability and the use of all recommended resources to achieve optimal health care outcomes and improve the use and satisfaction of individuals, families and communities with maternal health services.
Implicitly, a first step towards achieving the goals for maternal health in the Sustainable Development Goals (SDGs 3): ensuring healthy lives and promoting the well-being of all at all ages. For women this would mean to routinely monitor quality along the continuum of care in terms of structure, process and outcome, within the context of Donabedian model of quality care. The aim of this study was to assess the available resources (Structure) used in the provision of postnatal care in the facility, evaluate routine postnatal practices on the postnatal wards and clinic in accordance with WHO guidelines (Process), and to examine women’s level of satisfaction (Outcome) with the care they received in the study setting. The Donabedian model of quality care was used as the framework to evaluate the extent of implementation of WHO guideline for quality postnatal care. The three dimensions of quality care identified in the model namely; structure, process and outcome dimensions served as the basis for assessment in this study.
MATERIALS AND METHODS
This study was an exploratory cross-sectional survey. It employed a mixed method of data collection, which consists an initial phase of qualitative data collection followed by a second phase of quantitative data collection. The observation was the dominant method and it was employed in order to examine the actual care being provided by the care providers. On the other hand, the structured interview with questionnaire was used to assess the level of satisfaction among mothers.
The sample size of 57 mothers was determined using the formula n = N / [1 + N (e)2] Where; N = estimated population, e = level of error of tolerance (5%). A purposive sampling method was used in the selection of the mothers who gave consent to participate and affirmed that they would return to postnatal checkup. Purposive sampling method was used because only few of the mothers who had normal delivery confirmed they would return for postnatal follow-up in the facility. Mothers with still borne, postpartum hemorrhage or instrumental deliveries and caesarean section were excluded. Four data collection instruments were designed to achieve the objectives of the study, which included three checklists and one questionnaire. The checklists were adapted from WHO (2014) guideline for postnatal care to assess the structure (human resources, material resources and infrastructure), the process dimension (care provided) on the postnatal wards and postnatal clinic. A structured questionnaire was administered to the mothers to determine their level of satisfaction with postnatal care on the postnatal wards and postnatal clinic.
Ethical approval to conduct the study was issued after review by the University of Ibadan/University College Hospital Ethical Committee (NHREC/05/01/2008a). The respondents’ participation in the study was voluntary and consent was obtained after giving an explanation of the study. The respondents were assured of the absence of risk by their participation and confidentiality.
The qualitative data was collected first through non-participant observation using the prepared checklists to record relevant information on the available resources in the facility and on the postnatal care provided to the women. The duration of the observation on both the wards and the clinic was 4 weeks.
The mothers were selected for an exit interview and each respondent‘s questionnaire was marked and their phone numbers obtained to facilitate a follow up in the postnatal clinic. The mothers were followed up to their clinic appointment date, consent was obtained again and they were administered their individual questionnaires to complete on their exit from the postnatal clinic. Quantitative data obtained was analyzed using the Statistical package for social sciences (SPSS) version 22 and all results were presented using descriptive statistics, t-test, ANOVA and Chi square test.
RESULTS
Facility assessment (structure)
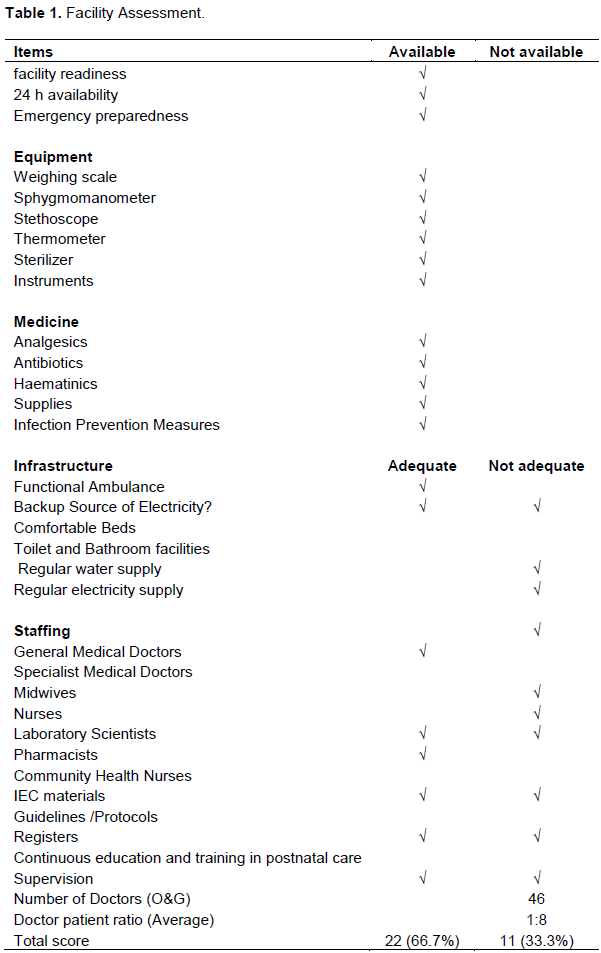
The result that only 66.7% of the required resources were available in the study setting, which is an indication of poor adherence to the WHO recommendation for postnatal care facility. The facility provides 24 h services and emergency preparedness alongside the availability of basic equipment needed to meet the health needs of postnatal women (Table 1). However, electricity supply, regular water supply, bathrooms and toilets are inadequate for the care of the postnatal women. The numbers of functional bathrooms and toilets on the wards and in the clinic appear insufficient in comparison to the population of the women. There are a total of 50 beds in the postnatal wards with an average of 25 patients on each ward including antenatal patients on admission, postnatal patients who had normal delivery and those who had complicated deliveries. In each ward and the clinic, there are two functional bathrooms and toilets with no regular water supply. On the average, 25 patients are seen in the postnatal clinic every clinic day. The available specialist medical doctors, midwives are insufficient with an average midwife to patient ratio of 1:8 per shift. There are no standardized postnatal guidelines and protocols used in the provision of care to the postnatal women in the facility. Although there are various in-service trainings organized in the institution on life saving skills, evaluation of nursing care, pain management, documentation, geriatrics, care of placenta, essential care of the newborn, advancement of health care, basic trauma care and cardio pulmonary resuscitation; continuing education and training on postnatal care is lacking.
Assessment of postnatal care (process)
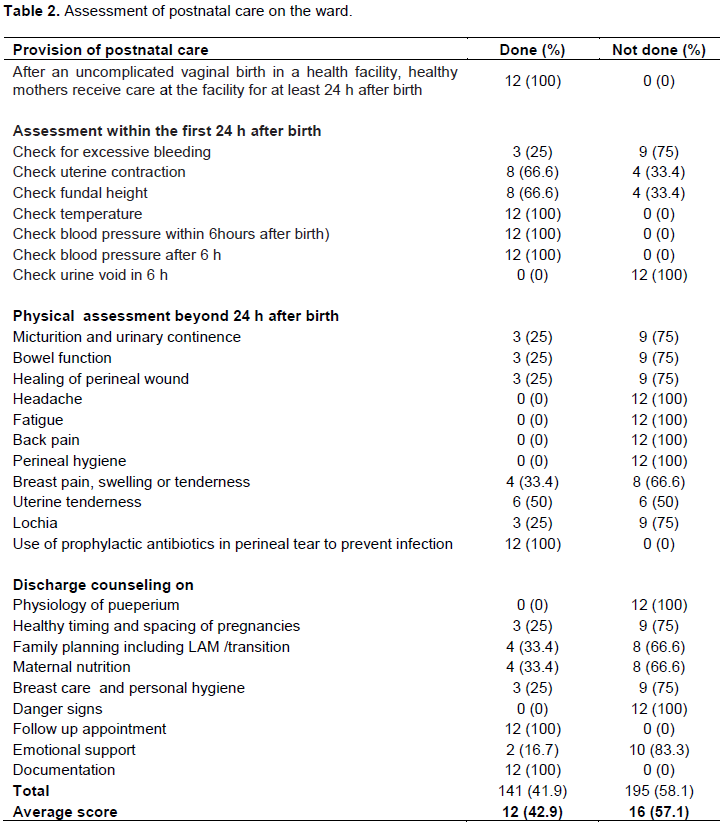
From the findings, only 42.9% of the required postnatal care was observed to be provided on the wards (Table 2) and 42.3% in the postnatal clinic (Table 3). This depicts poor adherence to the WHO practice guideline for postnatal care in the postnatal unit of the study setting. All women with uncomplicated vaginal delivery received care for at least 24 h after delivery in the study setting. On the wards, the initial assessment within the first 24 h after birth were conducted except checking for excessive bleeding which was not visually assessed, although the women were verbally asked if bleeding was normal or excess of 25% of the observation period. Meanwhile urine voiding resumption, frequency and characteristics were not assessed throughout the observation period. During the physical assessment beyond 24 h after birth bladder and bowel function, lochia, healing of perineal wound and breast were assessed about 30% of the observation period. Midwives were observed not to assess mothers for complaints such as headache, fatigue, back pain, and perineal hygiene during the period under investigation. Prophylactic antibiotics were prescribed for patients with perineal tears. Mothers were not provided with discharge counseling on the physiology of puerperium and danger signs. However, midwives (30%) provided counseling on family planning, maternal nutrition, breast care and follow up. Documentation was done in all cases and emotional support was observed in 16.7% of the observation period. While the only prescribed routine postnatal visit is from 6 weeks after birth and there is no provision for home visits within the first week of childbirth. A physical examination that was observed being conducted in the postnatal clinic was; blood pressure check, pallor, lochia, and uterine involution, while temperature, inspection of perineum for healing, and breasts were not assessed. Assessment of emotional and psychological wellbeing, resumption of sexual intercourse and dyspareunia were not observed in all the visits to the clinic.
Socio-demography of mothers
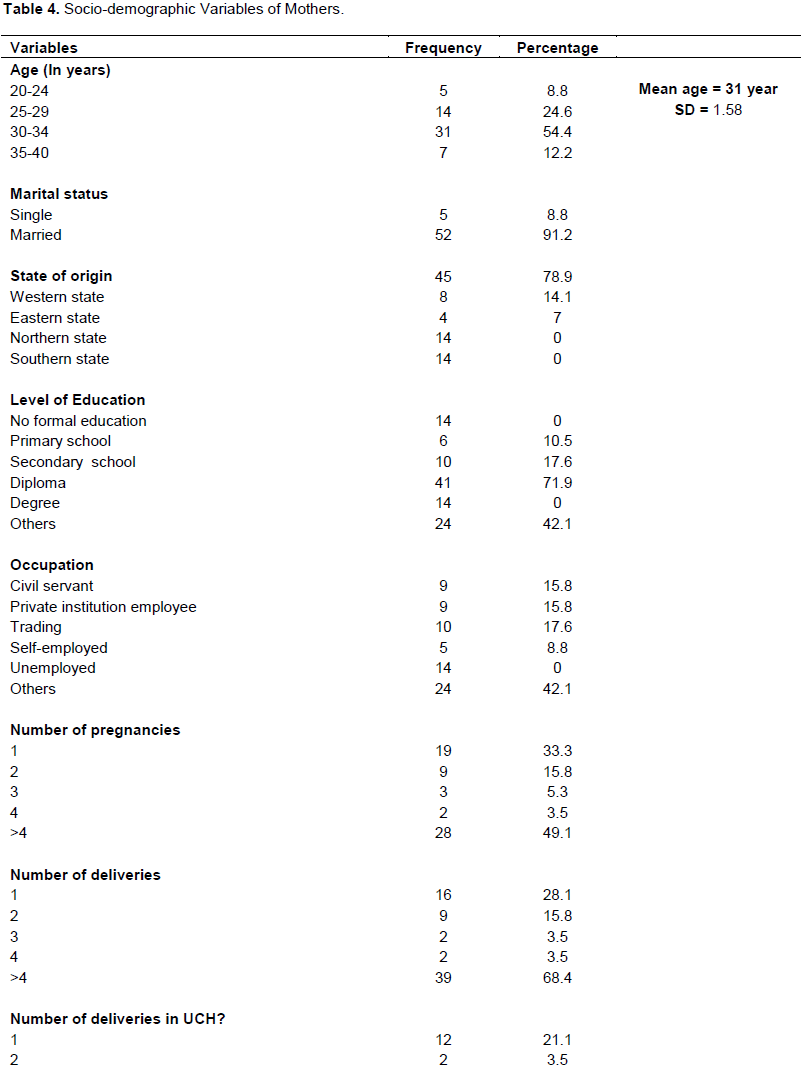
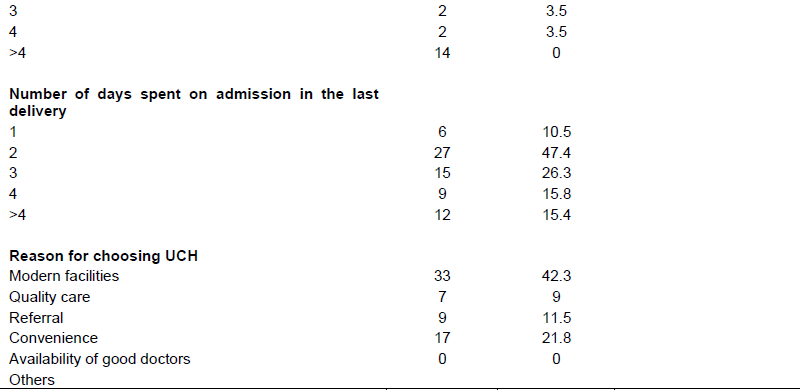
Table 4 illustrates the analysis of the demographic data of the postnatal women (mothers). A total of 57 mothers were sampled between the age of 20 and 40 with mean ±SD = 31±1.58. The majority (49.1%) were first time mothers. Reasons for choosing the facility included availability of modern facilities (15.4%), quality care (42.3%), convenience (11.5), and availability of good doctors (21.8%).
Mothers’ level of satisfaction
Satisfaction on the postnatal ward
Findings indicated that 36.5% of the mothers were not satisfied and 28.4% were fairly satisfied with the care received on admission after delivery. The majority (94%) of the women expressed satisfaction with routine vital signs monitoring and drug administration, but were not satisfied with the inadequate water and electricity, inadequate toilet and bathroom facilities, lack of individualized care (Table 5a). The analysis of variance revealed a significant difference (p<0.05) between the level of mothers’ satisfaction on the postnatal wards and the number of deliveries, the numbers of days they were on admission as well as the maternal age.
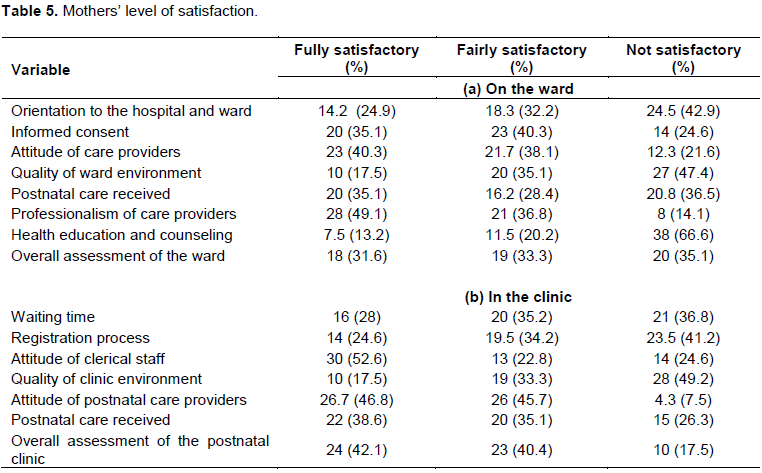
Satisfaction at the clinic
Majority (82.5%) of the mothers expressed good satisfaction with care received in the postnatal clinic. Specific areas of satisfaction were the attitude of the staff at the clinic, information provided and healthcare received. However, poor satisfaction was reported in the clinical environment (waiting area, toilet and bathroom) and cumbersome registration and payment procedures in the hospital (Table 5b). Additionally, the women in this study verbalized areas of dissatisfaction which include the following: bureaucracy, poor counseling, cumbersome registration and payment processes, inadequate provider-client relationship, admissions for days more than necessary, the assumption that patient knows everything, inadequate toilet and bathroom facilities, lack of regular water supply, waiting time, much cold at night on the wards, poor attention, lack of individualized care, lack of patient specific counseling and care by inexperienced doctors at the postnatal clinic. The analysis of variance revealed that there is a significant difference (p<0.05) between the mothers’ level of satisfaction with PNC at the clinic and the maternal age.
DISCUSSION
The findings of this study suggest that there is an insufficient human resources and infrastructure in accordance with the recommendations of the WHO. As explained by Donabedian (1988), poor structural quality will affect the provision of postnatal services to mothers and eventual outcome of postnatal care in this facility. Lotto (2015) also linked inadequate postnatal facility for the quality postnatal care to eventual decrease in the quality of postnatal services.
The facility is deficient in the staffing of Midwives and Doctors who are central to the provision of postnatal care to mothers. The average midwife: patient ratio in this study setting is 1:8 on the postnatal wards which is below the recommended standards and what is peculiar in more developed economies. Adelani et al. (2015) also observed a nurse/midwife to patient ratio ranging from ratio1:9 in a general hospital in Osun state, Nigeria. The NICE postulated for the Australian Nursing and Midwifery Federation a midwife/nurse to patient ratio of 1:4 plus a charge nurse in the morning and afternoon shift and 1:6 on the night shift (ANMF, 2015). The British Columbia Nurses Union (2016) on the other hand, recommended a range of midwife to patient ratio of 1:4 to 1:6 in an inpatient unit.
There are 46 Obstetrics/Gynecology specialists in this facility which are insufficient as opined by Agboghoroma and Gharoro (2015) in their study. They submitted that the number of Obstetrics/Gynecologists in Nigeria is inadequate in view of the population size, when computed this suggest a ratio of 1:181458 patients. When compared with the WHO (2010) recommendation of a ratio of one obstetric/Gynecologist to one thousand patients (1:1000), this is a far cry and may contribute to the poor maternal care services. In line with this majority of the women in a study in Nigeria submitted that the health providers are burdened with heavy workloads in the provision of maternal health care and linked the burden to the low quality of care (Ogu et al., 2017).
The high patient ratio to each of the postnatal care providers may be a contributing factor to the suboptimal quality of postnatal care offered at this facility. Empirical evidences suggest the number of patients allocated to a health provider on a shift is directly related to patient safety, patient satisfaction, mortality and quality of care (ANMF 2015). It is therefore imperative for the Nursing and Midwifery Council of NIGERIA and the National Association of Nigerian Nurses to collaborate to design a standard nurse: patient ration that is suitable to Nigerian health need which should also apply to the Nigerian medical association.
Consequently, the legislation of standard ratio would serve as a baseline for employment in all government hospitals in the country, reduce waiting time, improve the quality of care, improve retention of health providers as a result of better and safer working environment, increase capability of hospitals to meet patient demands, and improves the economic performance of hospitals. Inadequate in-service training was also observed in this study, as none of the 50 postnatal care providers who had continuous education in the last 2 years had any training on postnatal care. Continuous training and education is an essential pre-requisite for quality improvement in the provision of services and also contributes to quality of inpatient and outpatient care (Chaghari et al., 2017). Staff shortages and inadequate in-service training were also observed in China (Chen et al., 2014) while Chimtembo et al. (2013) in addition to inadequate facility, identified poor postnatal counseling in their study in Malawi.
There is non-availability of a guideline or protocol for the postnatal care of mothers in the study setting, as such there is no laid down standard for care givers in providing their services. Some healthcare providers in Tanzania also perceived that postnatal care was suboptimal in their facilities resulting from care being based on clinical experiences due to lack of guidelines and inadequate health personnels (Pallangyo et al., 2016). Kopp (2011) opined that use of clinical guidelines is an indispensable part of a professional quality system, and is an important tool to improve the knowledge, processes and outcomes in healthcare. They also provide a foundation for assessing and evaluating the effectiveness of healthcare.
The findings in this study suggest that the routine postnatal care provided in both the postnatal clinic and the wards of the facility are below the standard in accordance with WHO practice guidelines. This finding is supported by Chimtembo et al. (2013) whose study in Malawi revealed that the contents of postnatal services were below reproductive health standards. A sub-standard process component of postnatal care was also observed by Lotto (2015) in Tanzania. Luegmair et al. (2018) identified shortcomings in puerperal care and counseling in their study in Austria. Assessment is the second recommendation on the WHO (2014) practice guideline for postnatal care which was found to be poorly adhered to in this setting. Routine assessments are important for early identification of complications, prompt treatment or referral as needed. The majority of the assessment within the first 24 h after birth was done while the majority of the assessment beyond 24 h after birth was not done. Assessment of the psychological and emotional wellbeing of the mothers was not given much attention. Kanyunyuzi et al. (2017) study in Uganda revealed that assessment of the mothers after admission to the postnatal ward was found to be low.
Poor adherence to practical guidelines identified in this study can be attributed to the non-availability of a standard guideline in this facility, inadequate human resources and infrastructure amongst others. To achieve this vision of “every pregnant woman receives quality care throughout pregnancy, childbirth and the postnatal period”, six strategic areas have been identified by the WHO (2016) for improving the quality of maternal care namely; clinical guidelines, standards of care, effective interventions, quality measures, and the relevant research and capability building. The results of the evaluation of this study revealed that mothers received postnatal services that were below the WHO standard of quality postnatal care an indication of poor compliance with the guideline. In this study, 36.5% of the mothers were not satisfied and 28.4% were fairly satisfied with the overall postnatal care received on the postnatal wards. This was also the findings of Okonufua et al. (2017) who evaluated 8 secondary and tertiary hospitals in Nigeria. Many of the mothers had areas of dissatisfaction, or were not satisfied at all with the quality of care in antenatal, intra-partum and postnatal period. Reasons for dissatisfaction with postnatal care included poor staff attitude, long waiting time, high cost of services, and sub-standard facilities.
Most of the participants in a Pakistan study verbalized low quality of maternity care, disrespect and impolite behavior of health professionals (Munawar et al., 2017). On the other hand, Sacks et al., (2017) submitted that a large proportion of their participants reported positive postnatal experiences with more satisfaction among the Zambian than the Ugandan women. The third hypothesis tested in this study found a relationship between maternal satisfaction on the wards and the age and parity of the mother out of all the other selected maternal socio-demographic characteristics tested. While the fourth hypothesis revealed the absence of a significant difference between maternal satisfaction on the ward and in the clinic. Therefore, it is important for postnatal care providers to provide individualized, age and parity appropriate care to mothers in order to be able to meet their various health needs and yield satisfaction.
It was observed that this facility does not have any system in place for measuring outcomes of postnatal care. Measuring the quality of health care provided is an important evaluation that leads to improved care and accountability among care providers. Patient satisfaction in one of the indicators of quality care and it requires the provision of patient-centered care (including health education and counseling). Patient-centered care is health care that is respectful of, and responsive to, the preferences, needs and values of patients and consumers. Therefore, the quality of PNC in this facility can be greatly improved by the provision of individualized care and regular evaluation of patients through various feedback mechanisms. There should be awareness of feedback mechanisms among patients followed by inquiry through feedback questionnaires and other platforms (interviews, group discussions, online reviews etc) for expressing their complaints, satisfaction and suggestions on exit from the facility. There should be record keeping and analysis of degree of patients’ satisfaction through which gaps in care can be identified and resolved. Regular feedback evaluation will also promote accountability among the health care givers.
Additionally, hospital managers should ensure availability and adherence to guidelines and protocols in all the hospital department and wards. The hospital should also have a unit in charge of formulating protocols from recent evidences, from research and guidelines. In-service training of health workers should be specific to their units and specialties within the hospital.
CONCLUSION
The findings of this study have shown a poor adherence to the international practice guideline for postnatal care in the study setting in the structural, process and outcome aspects of postnatal care. Maternal satisfaction was good on exit from postnatal clinic and poor on exit from the postnatal wards. There is a need to strengthen the facility by availability of recommended resources and also need to have a standard guideline that will serve as a framework for provision of quality postnatal care.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Agboghoroma CO, Gharoro EP (2015). Coverage and Distribution of Obstetricians and Gynecologists in Nigeria. International Journal of Gynecology andObstetrics 129(1):50-53. |
|
|
African Population and Health Research Center (APHR) 2017. Maternal Health in Nigeria Facts and Figures. APHRC facts sheet June 2017. Available @ www.aphrc.org/wp. accessed June 23, 2018 |
|
|
Australian Nursing & Midwifery Federation (2015). Nurse/Midwife: Patient Ratios. It"s a matter of saving lives publication. ANMF Victoria Branch. |
|
|
Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, Adler A, Vera Garcia C, Rhode S, Say L, Lawn JE (2012). National, regional and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. The Lancet 379(9832):2162-2172. |
|
|
Carvajal-Aguirre L, Amouzou A, Mehra V, Ziqi M, Zaka N, Newby H (2017). Gap between contact and content in maternal and newborn care: An analysis of data from 20 countries in sub–Saharan Africa. Journal of Global Health 7(2). |
|
|
Chaghari M, Saffari M, Edabi A, Ameryoun A (2017). Empowering Educataion: A new Model for In-service Training of Nursing Staff. Journal of Advances in Medical Education and Professionalism 5(1):26. |
|
|
Chen L, Qiong W, Velthoven M, Yanfeng Z, Shuyi Z, Ye L, Wei W, Xiaozhen D, Ting Z (2014). Coverage, quality of and barriers to postnatal care in rural Hebei, China: a mixed method study. BMC Pregnancy and Childbirth 14(1):31. |
|
|
Chimtembo L, Maluwa A, Chimwaza A, Chirwa E, Pindani M (2013). Assessment of quality of postnatal care services offered to mothers in Dedza district, Malawi. Open Journal of Nursing 3(04):343. |
|
|
Donabedian A (1988). The quality of care. How can it be assessed? JAMA 260(12):174-1748 |
|
|
Kanyunyuzi AE, Ekong EN, Namukwaya RE, Namala AL, Mudondo L, Mwebaza E, Smyth R (2017). A criteria-based audit to improve early postnatal care in Jinja, Uganda. African Journal of Midwifery and Women's Health 11(2):78-83. |
|
|
Kearns AD, Caglia JM, Hoope-Bender P, Langer A (2016). Antenatal and postnatal care: a review of innovative models for improving availability, accessibility, acceptability and quality of services in low-resource settings. BJOG: An International Journal of Obstetrics & Gynaecology 123(4):540-548. |
|
|
Khanal V, Adhikari M, Karkee R, Gavidia T (2014). Factors associated with the utilization of postnatal care services among the mothers of Nepal: analysis of Nepal Demographic and Health Survey 2011. BMC Women's Health 14(1):19. |
|
|
Kinney M, Kerber K, Black R, Cohen B, Nkrumah F, Coovadia H, Nampala P, Lawn J, Axelson H, Bergh A, Chopra M, Diab R, Friberg I, Odubanjo O, Walker N, Weissman E (2010). Sub-Saharan Africa's mothers, newborns, and children: where and why do they die? PLoS Medicine 7(6): e1000294. |
|
|
Kopp IB (2011). From Clinical Practice Guidelines towards Quality Assurance. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz 54(2):160-165. |
|
|
Lotto TD (2015). Assessment of the quality of postnatal Care services (Doctoral dissertation, Mzumbe University). |
|
|
Luegmair K, Zenzmaier C, Oblasser C, Konig-Bachmann M (2018). Women's satisfaction with care at the birthplace in Austria: Evaluation of the babies born better survey national dataset. Midwifery 59:130-140. |
|
|
Munawar A, Hassan Z, Ayub A, Shaikh BT, Buriro NA, Ahmed F, Kumar R (2017). Women's perceptions about quality of maternity care at tertiary care hospital Karachi, Pakistan. Pakistan Journal of Public Health 7(2):109-112. |
|
|
Nigeria Demographic and Health Survey (NDHS) (2013). Nigeria Demographic and Health Survey by National Population Commission Federal Republic of Nigeria. |
|
|
Ogu RN, Ntoimo LFC, Okonofua FE (2017). Perceptions of women on workloads in health facilities and its effect on maternal health care: A multi-site qualitative study in Nigeria. Midwifery 55:1-6. |
|
|
Okonofua F, Ogu R, Agholor K, Okike O, Abdus-salam R, Randawa A, Abe E, Durodola A, Galadanci, The WHARC WHO FMOH MNCH Implementation Research Study Team (2017). Qualitative assessment of women's satisfaction with maternal health care in referral hospitals in Nigeria. Reproductive Health 14(1):44. |
|
|
Pallangyo E, Mbekenga C, Olsson P, Källestål C (2017). A baseline mixed-methods study on postpartum care among health professionals in Tanzania. African Journal of Midwifery and Women's Health 11(3):115-122. |
|
|
Pallangyo EN, Mbekenga C, Källestål C, Rubertsson C, Olsson P (2016). Healthcare provides' perceptions of postpartum care and its potential for improvement in low-income suburbs in Dar es Salaam, Tanzania. Sexual & Reproductive Healthcare 11:7-12. |
|
|
Sacks E, Masvawure TB, Atuyambe LM, Neema S, Macwan'gi M, Simbaya J, Kruk M (2017). Postnatal care experiences and barriers to care utilization for home and facility delivered newborns in Uganda and Zambia. Maternal and Child Health Journal 21(3):599-606. |
|
|
World Health Organization (2014). Trends in Maternal Mortality: 1990-2013, Estimates by WHO, UNICEF, UNFPA, The World Bank and the United Nation"s Population Division, Geneva. |
|
|
World Health Organization (WHO) (2014). WHO recommendations on postnatal care of the mother and the newborn. WHO Library Cataloguing-in- Publication Data. ISBN 978 92 4 1506649. |
|
|
World Health Organization (WHO) (2010). WHO Technical Consultation on Postpartum and Postnatal Care. Geneva, Switzerland. |
|
|
World Health Organization (WHO) (2016). Standards for improving quality of maternal and newborn care in health facilities. ISBN: 9789241511216. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


