Full Length Research Paper

ABSTRACT
Human Immunodeficiency Virus (HIV) is a global public health crisis with sub Saharan Africa having a disproportionately high burden of the epidemic. Women and children in many settings experienced high rates of new infection, HIV related illnesses, and deaths. High rate of infection among women reflected directly on children. This study aimed at assessing the acceptance of prevention of mother to child transmission (PMTCT) of HIV among pregnant women in Ogbomosho. A descriptive cross-sectional design was adopted for this study. It cuts across tertiary, secondary and primary health care in order to ensure appropriate representation of pregnant women attending different categories of health facilities. The instrument for the study was a self-structured questionnaire. Of the 300 pregnant women assessed, more than 50% of the respondent (n=184, 61.3%) had a high knowledge of PMTCT. Majority (89.0%) were willing to accept PMTCT measures if they are positive. There was a significant association between knowledge of PMTCT and acceptability of PMTCT of HIV measures (ï£2:12.34, p-value 0.002). There was no significant association between antenatal location and acceptability of PMTCT (ï£2:0.69, p-value 0.71). The study revealed that majority of the respondents had high knowledge of PMTCT and were willing to accept PMTCT measures if they are HIV positive. This underlines the necessity for improved availability of PMTCT services. The inclusion of health education on PMTCT during antenatal visits will improve pregnant women’s knowledge of PMTCT.
Key words: Prevention of mother to child transmission (PMTCT), acceptance of PMTCT, knowledge of PMTCT, HIV, pregnant women.
INTRODUCTION
Human Immunodeficiency Virus (HIV) is a global public health crisis with sub Saharan Africa having a disproportionately high burden of the epidemic (World Health Organization, 2014). Women and children in many settings continue to experience high rates of new infection, HIV related illnesses, deaths and high rate of infection among women reflect directly on children (WHO, 2014). Recent reports alarmingly showed that approximately 36.7 million people worldwide are living with HIV/AIDS, and of these are 2.6 million children less than fifteen years (WHO, 2015). Only 32% of children living with HIV were receiving antiretroviral treatment (UNICEF, 2015). With an estimated population of 177,071,561 people in Nigeria in 2013 (National Population Commission, 2014), Nigeria is second in the world in terms of the number of people living with HIV (United Nations, 2013). In 2014, an estimated 3.4 million people in Nigeria were HIV positive, 1,700,000 of these were women age 15 years and above and 380,000 were children aged 0 to 14 years (UNAIDS, 2015). Six states in Nigeria account for 41% of people living with HIV, including Kaduna, Akwa Ibom, Benue, Lagos, Oyo and Kano (NACA, 2017). Oyo State where Ogbomosho is located is ranked 7th among the 36 states including the Federal Capital Territory (FCT), in Nigeria, with a prevalence of 5.6% (National HIV/AIDS and Reproductive Health Survey, 2013).
Vertical transmission also known as Mother-To-Child-Transmission (MTCT) occurs when an HIV positive woman passes the virus to her baby (US President’s Emergency Plan for AIDS Relief, (PEPFAR), 2010). Greater than 90% of HIV infections among children occur through MTCT with 90% of MTCT occurring in sub-Saharan Africa (UNAIDS, 2012). A woman with HIV who had no prevention of MTCT intervention has a 30 to 45% chance of passing the virus to her baby during pregnancy, labor and delivery as well as during breast feeding (WHO, 2012). The rate of MTCT is dependent on factors which include viral load, mode of delivery, prolonged rupture of membranes, prematurity and breastfeeding (Boucher et al., 2009).
Prevention of Mother-To-Child Transmission (PMTCT) of HIV aims at reducing the risk of a mother infecting her child with HIV and starts with primary prevention of the infection in women of childbearing age who are the main vehicles of pediatric HIV transmission (WHO/UNAIDS/ UNICEF, 2011). Primary prevention is considered the most important way to decrease MTCT of HIV (Lynne, 2002). PMTCT strategies include testing for HIV during pregnancy, modified obstetric practices, preventive anti-retroviral (ARV) drugs, and modified infant feeding practices. With the introduction of PMTCT globally, the strategy has reduced the risk of MTCT from nearly 40% to fewer than 5% thereby making PMTCT a gateway for HIV prevention, treatment, and care support services for the whole family (UNICEF, 2010).
Statement of the problem
Over the years, great achievements have been attained in the area of eliminating new HIV infections in children globally. In developed countries, MTCT rates have fallen to as low as 2% of births among HIV-infected mothers with the introduction of HIV counseling and testing, Zidovudine prophylaxis, elective Caesarean delivery, and safe use of infant formula instead of breastfeeding (Maputle, 2008). The number of new HIV infections among children declined by 13% between 2000 and 2008, and by 48% between 2009 and 2014. Some countries in sub-Saharan Africa are also having good progress in reversing the high rate of new infection in children, this includes countries like Ghana that experienced a decline of 76% and South Africa that experienced a decline rate of 76% (USAIDS, 2015). However, some other sub-Saharan countries still face significant challenge in rolling out effective PMTCT services. This includes Nigeria that has the second largest number of new HIV infections among children with as much as 60,000 new pediatric infections occurring in 2012 alone (WHO, 2014). Since 2009, new pediatric HIV infections in the country have declined by only 15% (USAIDS, 2015). This is quite low compared to what is been experienced in other sub Saharan countries
This clearly indicates that there is a problem in the country which needs to be addressed urgently. This is especially distressing as good progress is being achieved in other countries within the region using the same approaches. The reasons for this might include poor knowledge of mothers on the risk of MTCT, poor knowledge on prevention of mother to child transmission strategies such as the use of anti-retroviral drugs during and after delivery, infant feeding options, and poor obstetric practice by health personnel (De Cock et al., 2012). There is limited information on the acceptability of pregnant women in relation to prevention of mother to child transmission of HIV in Ogbomosho, Oyo State. It is due to this perceived paucity of information and the problem identified earlier (poor decline rate in mother to child transmission of HIV in the country) that this study was conducted to assess the acceptance of prevention of mother to child transmission of HIV among pregnant women in Ogbomosho, Oyo State.
Study objectives
The broad objective is to assess the acceptance of Prevention of Mother to Child Transmission of HIV among pregnant women attending ANC in Ogbomosho, Oyo State.
Specific objectives
(1) To evaluate the knowledge of prevention of mother to child transmission of HIV among pregnant women.
(2) To examine pregnant women’s willingness to accept prevention of mother to child transmission of HIV.
Study hypotheses
(1) There is no significant association between the pregnant women knowledge of PMTCT of HIV and their acceptance of PMTCT of HIV.
(2) There is no significant association in the pregnant women acceptance of prevention of mother to child transmission of HIV and their place of antenatal care.
Significance of the study
This study will help to provide baseline information on knowledge and acceptance of PMTCT of HIV among pregnant women. It will also help to facilitate quality and efficient health care services to reduce MTCT of HIV infection and identify the specific areas in the program that need to be improved. In order to optimize the use of PMTCT services, good knowledge of pregnant women is paramount, and potential mothers need to be aware of the risk of MTCT of HIV and the possibility of reducing it. The findings of this study will also help to inform health workers, educators and policy makers in designing appropriate and tailored health education and policies for women. This will increase their level of knowledge of PMTCT of HIV, translating into better access and utilization of PMTCT services in Ogbomosho. This should consequently result into reduced MTCT of HIV and improved maternal and child health. The study findings would establish data for nursing education and other health professionals to meet the pregnant women needs effectively by providing information about HIV/AIDS to pregnant women, and to improve the quality of care to HIV/AIDS positive mothers.
MATERIALS AND METHODS
Research design
The study was a descriptive cross sectional design (Neuman, 2011).
Study setting
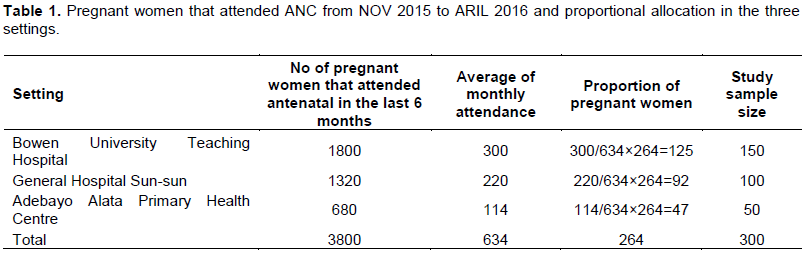
Ogbomoso was founded around the mid-1600, the people predominantly belong to the Yoruba ethnic group. The study was conducted in selected health facilities in Ogbomosho, Oyo State. It cut across tertiary, secondary and primary health facilities in order to ensure appropriate representation of pregnant women attending different categories of health facilities. The selected facilities include Bowen University Teaching Hospital, General Hospital Sunsun and Adebayo Alata Primary Health Care.
Target population
This consisted of all pregnant women attending ante natal clinics in health institutions within Ogbomosho.
Sample size
The sample size for the study population was determined using the formula for studying single population proportions with population less than 10,000 as follows:
n = (Zα)2pq / d²
n = (1.96 × 1.96 × 0.5 × 0.5) / (0.05)² = 384.16
= 385
Since the study population was less than 10,000, then nf = n/1+(n)/(N) (Araoye 2004),
Nf = 385 / 1 + (385) / (634)
nf = 239.58
= 240
Adjusting for non-response using a rate of 10% is 24. Sample size after adjusting for non-response = 264. Since the sample size calculated (264) is the minimum that could be used, an additional 38 was added to the sample size to make it 300 (Table 1).
Inclusion criteria
The respondents who were eligible to participate in the study were pregnant women who were attending antenatal clinics, those who speak and understand Yoruba or English and all pregnant women who gave an informed consent.
Sampling technique
A simple random technique (paper balloting) was used in selecting a health facility from the three categories (tertiary, secondary, primary). Consecutive sampling method was then used in selecting participants, as pregnant women presenting at the clinic meeting the inclusion criteria were recruited.
Instrument for data collection
The instrument for the study was a self-administered structured questionnaire. Section A seeks information on socio demographic characteristics of the pregnant women, Section B focused on knowledge of PMTCT among the respondents and Section C exposed the acceptance of PMTCT measures among pregnant women. The instrument for data collection was translated into Yoruba (the local language) and back translated to English by a research expert who is also a Yoruba translator.
Validity of instrument
Face and content validity of the instrument was ensured by the use of relevant literature, as well as by presenting it to the study supervisor, HIV/AIDS researcher, obstetricians, research experts, and a statistical analyst.
Reliability of instrument
The reliability of the instrument was statistically determined using the test retest method with 20 pregnant women attending antenatal clinic in LAUTECH University Teaching Hospital. A reliability coefficient (Cronbach’s alpha) of 0.79 was approved acceptable for the study.
Ethical considerations
Ethical approval for the study was obtained from the Oyo State Ministry of Health and permission from the various hospitals under study. Informed consent was obtained from participants after being duly informed about the details of the study.
Method of data collection
The questionnaires were administered by the researcher and research assistants. Two research assistants were recruited and trained on data collection instrument (correct and proper filling of the questionnaire). The research assistants were students who understand and can communicate in Yoruba (the local language) from School of Midwifery, Bowen University Teaching Hospital. During administration of the instrument, necessary assistance were made available to pregnant women in cases where they were unable to interpret the questions because of their level of formal education by reading out the questions in Yoruba (the local language) and their response were documented. The questionnaire was translated to Yoruba and back translated to English. Data was collected for a period of four weeks at the three health facilities.
Method of data analysis
Statistical Package for the Social Sciences (SPSS) version 23 was used for data analysis.
Objective one
To determine the knowledge of Prevention of Mother-To-Child Transmission of HIV among pregnant women. This constitutes 23 items and was dichotomized into good and poor knowledge using the average of the total score (12) score as cut-offs. The items were rated 0 (wrong) and 1 (correct) based on participant’s responses. A score of 12 and above was rated as high knowledge, while a score below 12 was rated low knowledge. This was analyzed using frequency table, percentages and descriptive statistics such as mean and standard deviation.
Objective two
To determine pregnant women’s willingness to accept PMTCT of HIV, acceptance of PMTCT constitutes 11 items. Responses were either Yes or No. Each correct response was scored 1 mark and incorrect response scored 0. Respondents with score of 6 or greater than 6 were categorized to be willing to accept PMTCT while those with scores less than 6 were categorized not to be willing to accept PMTCT. It was analyzed using frequency table and percentages and descriptive statistic such as mean and standard deviation. Statistical hypotheses were tested using Chi square test of significance.
RESULTS
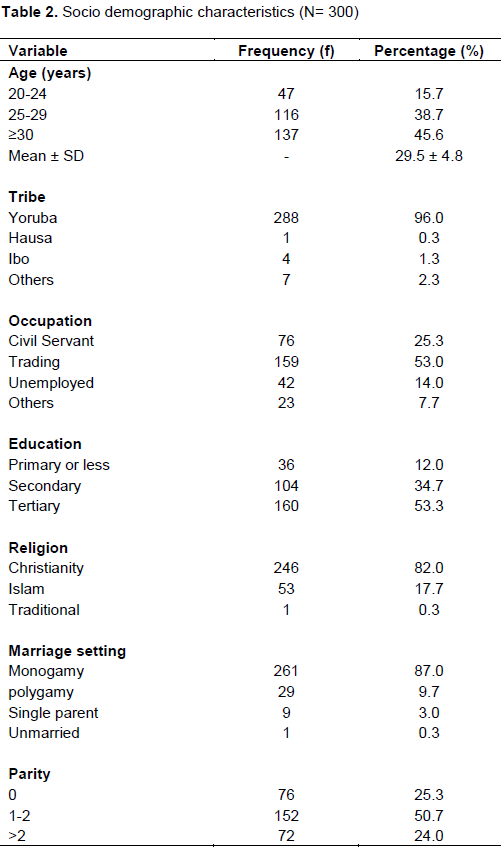
Table 2 shows that among the overall 300 women selected for this study, the mean age was 29.5 ± 4.8 years. Majority (96.0%) were of Yoruba tribe and 53.0% involved in trading as a means of livelihood. About half of the women (53.3%) had tertiary education, more than 80% were Christians and in monogamous marriage. About one-quarter of the women (25.3%) have never given birth, 50.7% have 1 to 2 children while 24.0% have more than 2 children.
In Table 3, more than 50% of the total number of women selected for the study (n=184, 61.3%) had a knowledge score greater than 12 while the remaining 38.7% had knowledge score below 12. The mean knowledge score was 25.97 ± 7.78 greater than average of the total score and the range 0 to 23. More than 80% knew that a mother with HIV can infect her unborn child with the virus. A good proportion of the women knew that transmission of mother to child could occur during pregnancy while just 30.7% knew that transmission could occur during labor. More than three quarter of the respondents knew that mother to child transmission is preventable. Infants feeding options identified by majority of the respondents was breastfeeding alone with 50% followed by infant formula alone with 48.7%. 60.7% of the respondents knew that mixed feeding option increases the infant’s risk of acquiring the infection and should be discouraged. More than half of the respondents knew the means of preventing mother to child transmission of HIV except Caesarean section in which only 45.7% of the respondents identified as a means of prevention (Figure 1).
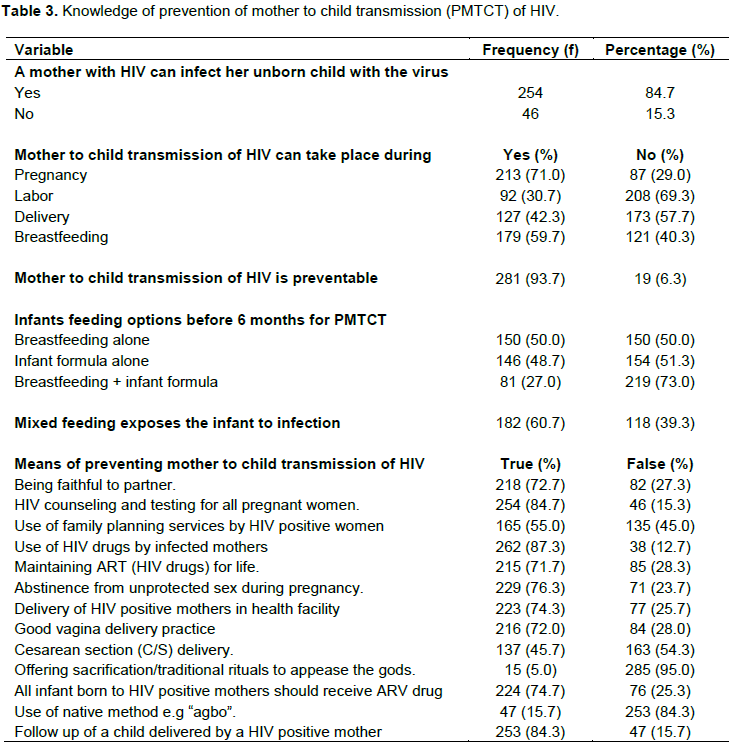
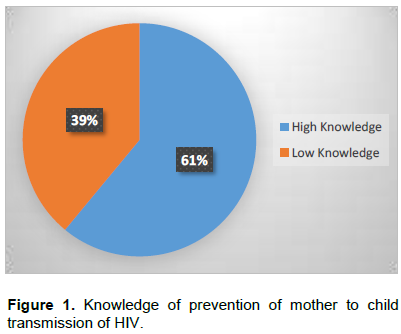
Table 4 shows that majority of the pregnant women (89%) had an acceptance score of 6 and above while the remaining 11% had a score below 6. The mean average of the total score, with a range of 0 to 11. Furthermore, all the women have had HIV test done in their current pregnancy. More than three-quarter of the women stated that if they were to be HIV positive they would accept prescribed drugs, exclusive breastfeeding and replacement feed for baby for 6 months, to administer prescribed HIV medication to their newborn, cesarean section, to deliver their baby in a health facility (hospital), take baby for follow up visit in the hospital, and family planning measures after delivery to prevent unplanned pregnancy. A little above half of the respondents (61%) indicated that they would not practice mixed feeding in the first 6 months if they are HIV positive.
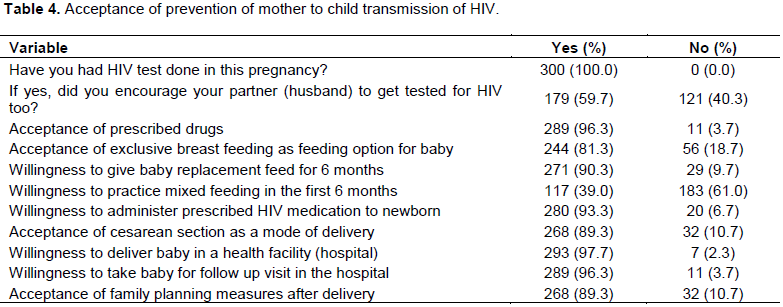
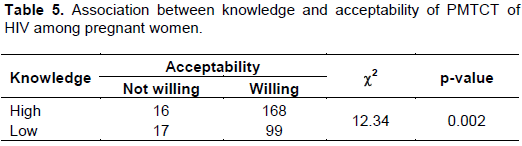
Table 5 shows that the null hypothesis of no significant relationship between knowledge of PMTCT and acceptability of PMTCT of HIV was accepted because the c2 value (12.34) yielded a p-value (0.002) which is less than 0.05. This implies that the proportion of women who would accept PMTCT of HIV vary significantly with knowledge of PMTCT. Hence, we could conclude that there was significant association between knowledge of PMTCT and acceptability of PMTCT of HIV among the respondents.
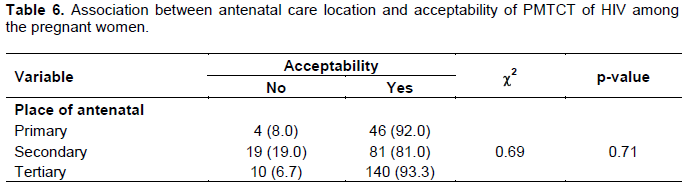
In Table 6, the null hypothesis of no significant relationship between antenatal location and acceptability of PMTCT of HIV in Table 5 was rejected because the c2 value (0.69) yielded a p-value (0.71) which is greater than 0.05. This implies that the proportion of women who would accept PMTCT of HIV do not vary significantly by place of antenatal delivery. Hence, we could conclude that there was no significant association between antenatal location and acceptability of PMTCT of HIV among the respondents.
DISCUSSION
Socio demographic characteristics
The mean age of the respondents was 29.5 ± 4.8 years. This report is similar to what was reported by Samuel et al. (2012), where the mean age of the respondents was 26.6 ± 1.4 years. This may be because this age bracket is the most productive age of an individual. Ogbomosho is dominated by Yoruba and majority were involved in trading as a means of livelihood. Being a semi urban environment, the percentage of respondents with education above secondary level is more than 50%. More than 80% were Christians; this may be the reason why a high percentage of the respondents were in monogamous marriage.
Knowledge of PMTCT among pregnant women
This study focused on pregnant women regardless of their HIV status because one of the key components of PMTCT of HIV is primary prevention of HIV infection among women of childbearing age and HIV testing and counselling for all pregnant women during ante natal. Knowledge of PMTCT of HIV among the pregnant women was high. This is slightly similar to the findings of Olugbenga et al. (2013) in a study in South-Western Nigeria and Abajobir and Zeleke (2013) Hawassa Referral Hospital, South Ethiopia where a high level of knowledge about MTCT and PMTCT of HIV was recorded. The finding may be attributed to the fact that the study was conducted in South West Nigeria similar to the work of Olugbenga et al. (2013). Also, generally, in Nigeria it is believed that people from south west value education. This may also be the reason why the knowledge on PMTCT was high as majority of the study respondent had at least a secondary education.
Furthermore, more than three quarter of the respondents (87.3%) knew that use of ARV (HIV drugs) by infected mothers as soon as possible after diagnosis is a means of preventing mother to child transmission, this is contrary to what was concluded by Abajobir and Zeleke (2013) where only 48.3% of the respondents knew that ART drugs given to HIV positive pregnant mothers could reduce transmission from HIV-positive mother to child. This may be because of the high level of awareness of PMTCT demonstrated by the respondents, as respondents identified health workers, media and church/mosque as their major sources of information of PMTCT.
A good proportion of the respondents from this study (84.7%) knew that a mother with HIV can infect her unborn child with the virus, but in a hospital based study by Tatagan et al. (2011) in Togo among women attending ante natal clinic, only 27.1% were able to identify that a mother with HIV can infect her unborn child with the virus. These differences may be due to an increase awareness of PMTCT. Also from this study, majority of the respondents (93.7%) knew that mother to child transmission of HIV is preventable, this is similar to what was obtained by Artwine et al. (2012) on knowledge and practice of women in rural Uganda where 72% of the respondents were aware that mother to child transmission of HIV can be prevented. This can also be attributed to the high level of knowledge and awareness displayed by the study participants. According to Samuel et al. (2012) in a similar study, awareness of breastfeeding as a source of infection to new born was high at 83.6% but in this study only 59.7% of the respondents knew that mother to child transmission of HIV can take place during breastfeeding. The researcher could not ascertain the quality of health education given on PMTCT to pregnant mothers as none of the health facilities under study gave health education on PMTCT throughout the study period hence there could be an inadequacy in the health education given by health workers to pregnant women on PMTCT. Maputle and Jali (2008) also found low level of knowledge about MTCT through breast feeding among women attending an urban teaching hospital in Natal. In this study, less than half of the respondents identified that mother to child transmission of HIV can occur during pregnancy, labor and delivery, this is similar to what Falnes reported where only 40% of the women studied in rural and urban areas of Moshi district in the Kilimanjaro region of Tanzania were aware MTCT could occur during pregnancy. This finding is less than what the researcher expected since the respondents demonstrated a high level of awareness of PMTCT.
Acceptance of PMTCT among pregnant women
Having a positive knowledge of PMTCT is highly important, but it is the positive utilization of the knowledge through accepting measures aimed at preventing mother to child transmission of HIV that will eventually lead to the desired outcome of eliminating new infection in children. In this study, majority of the pregnant women (89.0%) were willing to accept prevention of mother to child transmission of HIV. This may be because of their high level of knowledge of PMTCT. All the women have had HIV test done. In all the study settings, HIV test is a major part of the ANC booking requirement, it is mandatory and not optional for all pregnant women. Majority reported that they would accept prescribed HIV medication to prevent mother to child transmission of HIV if they are positive. This is similar to what was reported in a study by Moses et al. (2008) and Urban and Chersich (2014) on a similar topic where most of the women will accept HIV screening antiretroviral drugs if offered. The study also identified that only 29% will accept cesarean section if offered to prevent MTCT of HIV but in this study, majority of the respondents (89.3%) reported that they will accept cesarean section if procedure will reduce the risk of transmission to baby if they are positive. This may be because of the heighten advocacy on the important of caesarean section in delivery which has now translated to people seeing it as a safe method of delivery. Majority of pregnant women examined in another study by Moses et al. (2009) on knowledge, attitude and practice of ante-natal attendees toward PMTCT of HIV infection in a tertiary health facility, Northeast-Nigeria accepted PMTCT as a veritable means of preventing infants from HIV infection as well as an opportunity to know ones HIV status through voluntary testing.
Hypotheses testing
There was significant association between knowledge and acceptability of PMTCT of HIV among pregnant women as the proportion of women who would accept PMTCT of HIV varies significantly with knowledge of PMTCT (c2 value (12.34) yielded a p-value (0.002) which is less than 0.05). Hence, the higher the knowledge of PMTCT of HIV, the more the willingness to accept PMTCT.
There was no significant association between antenatal location and acceptability of PMTCT of HIV among the respondents as the proportion of women who would accept PMTCT of HIV do not vary significantly by place of antenatal delivery (c2 value (0.69) yielded a p-value (0.71) which is greater than 0.05).
CONCLUSION
The findings revealed that knowledge of PMTCT of HIV among the respondents was high and majority of them were willing to accept prevention of mother to child transmission of HIV measures. Hence, knowledge of PMTCT and acceptance of PMTCT among pregnant women may not be the reasons for the poor decline rate of mother to child transmission of HIV leading to increased number of children living with HIV in the country.
Implication for nursing
Health education on PMTCT of HIV should be included during every antenatal visit to all pregnant women to increase their level of awareness and knowledge. As the concept of PMTCT is not static and the role of nurses cannot be over emphasized, it is therefore paramount for nurses to attend workshops and conferences on PMTCT to update their knowledge and improve their skills.
RECOMMENDATIONS
In as much as knowledge of prevention of mother to child transmission of HIV was good, inclusion of health education on PMTCT during antenatal visits on a daily basis will be of great importance as it was observed that none of the facilities gave health talk on the concept of PMTCT throughout the 4 weeks of the study. Though the acceptance rate was also excellent, there should still be increase awareness of prevention of mother to child transmission of HIV available to the members of the community.
Since this study is hospital based, a more encom-passing evaluation of knowledge and attitudes of the community about HIV/AIDS and mother-to-child transmission, including the male partners, will provide added information for establishing a community involvement and intervention program on PMTCT Male involvement in programs to prevent mother to child transmission of HIV will also go a long way in promoting their support and participation in order to reduce mother to child transmission of HIV.
Willingness of PMTCT among HIV infected mother can be assessed in order to assess their actual level of acceptance.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abajobir AA, Zeleke AB (2013). Knowledge, Attitude, Practice and Factors Associated with prevention of Mother-to-Child Transmission of HIV/AIDS among Pregnant Mothers Attending Antenatal Clinic in Hawassa Referral Hospital, South Ethiopia. Journal of AIDS and Clinical Research 4(6):2-7. |
|
|
Araoye MO (2004). Research methodology with statistics for health and social sciences. NATHADEX Publishers Ilorin pp. 117-118. |
|
|
Artwine BR, Rukundo A, Mutibwa D, Sebikali JM, Tumusiime D, Amureeba RT, and Birungi L (2012). Knowledge and Practices of Women Regarding PMTCT in Mwizi Sub County. |
|
|
Boucher M, Cohen H, Gruslin A, Money D, Steben M, Wong T (2009). Mode of delivery for pregnant women infected by the Human Immunodeficiency Virus. Journal of the Society of Obstetricians and gynecologists of Canada 23(4):348-350 |
|
|
De Cock KM, Fowler MG, Mercier E, De Vincenzi I, Saba J (2012). Prevention of mother-to-child HIV transmission in resource-poor countries: translating research into policy and practice. JAMA 283 (9):1175-1182 |
|
|
Falnes EF, Tylleskar T, Paoli MM, Manongi R, Engebretsen IS (2010). Mothers' knowledge and utilization of prevention of mother to child transmission services in northern Tanzania. Journal of International AIDS Society. |
|
|
Lynne M, Munderi M, Mofenson P (2002). Safety on anit retroviral prophylaxis of perinatal transmission of HIV infected pregnant women and their children. Journal of Acquired Immune Deficiency Syndromes pp. 200-215. |
|
|
Moses AE, Chama C, Udo SM, and Omotora BA (2009). Knowledge, attitude and practice of ante-natal attendees toward prevention of mother to child transmission (PMTCT) of HIV infection in a tertiary health facility, Northeast-Nigeria. East Africa Journal Public Health 6(2):128-135. |
|
|
Moses OA, Munir'deen AI, Peter AA (2008). Awareness and Knowledge of Mother-to-Child Transmission of HIV among Pregnant Women. Journal of the National Medical Association 99(7):758-763. |
|
|
Maputle MS, Jali MN (2008). Pregnant women's knowledge about MTCT of HIV infection through breastfeeding. Curationis 31(1):45-51. |
|
|
NACA (2017). National Strategic Framework on HIV and AIDS: 2017-2021 |
|
|
National HIV/AIDS and Reproductive Health Survey (2013). HIV prevalence in Nigeria; Abuja, Nigeria. |
|
|
National Population Commission (2014). Nigeria Demographic and Health Survey; NPC and ICF International Abuja, Nigeria |
|
|
Neuman WL (2011). Social Research Methods, Qualitative and Quantitative approaches. Allyn and Beacon; Boston |
|
|
Olugbenga-Bello AI, Adebimpe WO, Osundina FF, Abdulsalam ST (2013). Perception on prevention of mother-to-child-transmission (PMTCT) of HIV among women of reproductive age group in Osogbo, Southwestern Nigeria Dovepress, |
|
|
President's Emergency Plan for AIDS Relief (2010). Scaling up the response to gender-based violence in PEPFAR. Consultation on gender-based violence, Washington DC: AIDSTAR-1 |
|
|
Samuel KH, Terlumun ZS, Terkaa TB (2012). Knowledge, Attitudes and Barriers towards Prevention of Mother To-Child Transmission of HIV among Women Attending Antenatal clinics in Uyam District of Zaki-Biam in Benue State, Nigeria. African Journal of Reproductive Health 16(3):27-34. |
|
|
Tatagan A, Mouhari-Toure A, Saka B, Akakpo AS, Kombate D, Tchama R, Singo A, Mpélé K, Pitche P (2011). Knowledge, attitudes and practices about prevention of mother to child transmission of HIV (PMTCT) among pregnant women in antenatal clinic at 2010 in Togo. Medecine tropicale: revue du Corps de sante colonial 71(5):472-476. |
|
|
Joint United Nations Programme on HIV/AIDS (UNAIDS) (2012). UNAIDS Report on the global AIDS epidemic. Geneva. |
|
|
Joint United Nations Programme on HIV/AIDS (UNAIDS) (2013). Progress Report on the Global Plan toward eliminating HIV in children by 2015 and keeping their mothers alive retrieved on 30th October, 2013. |
|
|
Joint United Nations Programme on HIV/AIDS (UNAIDS) (2015). Epidemiological slides – How AIDS Changed Everything report. |
|
|
Joint United Nations Programme on HIV/AIDS (UNAIDS) (2015). Fact sheet; 2014 statistics. |
|
|
United Nations Children's Fund (2010). PMTCT Factsheet. |
|
|
UNICEF (2015). Preventing mother-to-child transmission (PMTCT) of HIV. |
|
|
Urban M, Chersich M (2004). Acceptability and utilization of voluntary HIV testing and Niverapine to reduce mother to child transmission of HIV-1 integrated into routine clinical care south African Medical Journal 94(5):362-366. |
|
|
WHO/UNICEF/UNAIDS (2011). A guide on indicators for monitoring and reporting on the health health sector response to HIV/AIDS. Geneva. |
|
|
World Health Organization (WHO) (2012). Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants: Recommendations for a Public Health Approach; World Health Organization: Geneva, Switzerland. |
|
|
World Health Organization (WHO) (2014). Guidance on Global Scale up of the Prevention of PMTCT of HIV. Toward Universal access for Eliminating HIV and AIDS among children. WHO, Geneva. |
|
|
World Health Organization (WHO) (2014). Global HIV and AIDS statistics. |
|
|
World Health Organization (WHO) (2015). Global Health Observatory data repository on HIV |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


