Full Length Research Paper

ABSTRACT
The use of cesarean section (CS) and oxytocin for labour augmenttion may contribute to increase morbidity and mortality of mothers and newborns. The objective of the study was to evaluate the Criterian Based Audit (CBA) on CS rates and oxytocin use in labouring women. A prospective intervention study by CBA was performed at hospital in Tanzania. Included were 523 labouring women at a gestational age of at least 28 weeks and birth weight ≥1000 g. All data on actual care were compared to criteria for best practice agreed with the staff. Interventions were discussed with the staff followed by a training session. At follow up, data were achieved from 438 women. Performance and outcomes were compared before and after the intervention. The overall CS rate decreased from 46.1 to 38.4% (RR=0.83; CI: 0.72 to 0.97). The use of oxytocin decreased from 76.2 to 47.3% (RR=0.63; CI: 0.45 to 0.85). The study demonstrates suboptimal care in labour monitoring and management, and that CBA resulted in a reduction in CS and use of oxytocin, and suggests that CBA can be used for quality assurance of women’s health care.
Key words: Prolonged labor, low-income country, cesarean section, vacuum extraction, criterion-based audit, oxytocin, partograph.
INTRODUCTION
bleeding that can be challenging to control with restrained ressources (Bailey et al., 2017; Harrison et al., 2017; Nolens et al., 2019).
The use of oxytocin for labour augmentation at prolonged labor can increase the risk of intrauterine asphyxia and Safe deliveries are essential for a healthy society. Pregnancy and childbirth claim the lives of almost 300 000 women each year and of these, 99% occurs in low-resource countries. (Hailu and Berhe, 2014) Prolonged labour is aA major risk factors for maternal morbidity and mortality. is prolonged labour. An increasing frequency of cesarean section (CS) has raised concern with increased risk of anaesthetic complications, infections and excessive bleeding that can be challenging to control with restrained ressources. (Bailey, van Roosmalen et al., 2017, ; Harrison, Pasha et al., 2017, ; Nolens, Capelle et al., 2019) .
The use of oxytocin for labour augmentation at prolonged labor can increase the risk of intrauterine asphyxia and neonatal deaths, this risk is higher in low-income countries were where close monitoring of fetal wellbeing and frequency of contracions contractions is often is difficult to conduct in low-income countries.(Suleiman and Mokuolu, 2014). Survivors of perinatal asphyxia may suffer from cerebral palsy, functional disability and cognitive impairment. (Azzopardi, Strohm et al., 2014).
Monitoring the progress of labor using the partograph is one globally recommended to secure safe progress of labour and maternal and fetal wellbeing. throughout Throughout active labour it guides the correct use of interventions like CS and oxytocin .(Brown, Paranjothy et al., 2013, ; Yisma, Dessalegn et al., 2013).
One way to assess and improve clinical performance is criterion-based audit (CBA), which is a quality assurance tool. Criteria for best practice are set through a review of international and local guidelines and adjusted with staff to be realistic for the local context. Actual practice is compared to these criteria and findings are discussed with staff with the aim of clarifying areas that need improvement. Suggestions for quality improvements are implemented and subsequently assessed .(Graham, 2009). However, there is limited evidence for the effect of CBA in relation to management of normal and prolonged labor .(Maaloee, Sorensen et al., 2012a).
Accordingly, wethis study aimed The to evaluate the effect of CBA onf CS rates an oxytocin use, was therefore the aim of this study. The purpose of the study was therefore to investigate the effect of CBA on rates of CS and oxytocin use.
MATERIALS AND METHODS
This prospective quasi-experimental study was planned to assess the impact of CBA on management of normal and prolonged labor at Kilimanjaro Christian Medical Centre (KCMC), northern Tanzania. The hospital is a referral hospital with 3312 deliveries in 2015, of which 43% were by cesarean section (CS). Five consultants in gynecology and obstetrics and 21 residents constitute the departmental medical staff. The labor and antenatal wards are staffed by 29 midwives.
The partograph was initiated when the women appeared in the antenatal ward and cervix was at least four centimeters dilated, as this is considered as active labour. Normal progression was defined as ≥≥1 cm/h visualized on the partograph as the Alertline. A delay during the delivery of more than 4 h, was defined as prolonged labour, and the Actionline on the partograph was crossed. The women were referred to the labor ward when the uterine cervix was dilated 7 cm . Midwives with at least one year of midwifery training attended deliveries. A medical intern and a resident were always on call at the labor ward. They were always supervised by a consultant.
Included were women admitted for delivery at KCMC with a gestational age more than 28 weeks after informed consent. Excluded were women who delivered a baby with a birthweight below 1000 g. All women and staff members received verbal and written information about the study and informed consent was signed. They were assured that their identities would be kept confidential and participation was voluntary, and that nonparticipation would not affect the care received.
The study was a full CBA cycle including five steps (Figure 1). The first step was establishing audit criteria (Figure 1) based on international and Tanzanian guidelines ( Mathai et al., 2003) and , Welfare (2015)by two local consultants and two midwives, to reach a consensus. The following criteria were agreed upon regarding partograph: . Prolonged active phase first stage of labor was defined as dilation less than 1 cm/h indicated by the alert line on the partograph. The action line was reached if the progress deviated more than four hours from the alert line. Artificial rupture of membranes should be performed at a crossed alert line .(Brown, et al., 2013). Augmentation of contractions with oxytocin should be performed at a crossed action line ,(Sorensen, et al., 2010)and a CS was recommended if these actions did not normalize progress (Appendix 1) .(Yisma, et al., 2013). Fetal distress were defined as a fetal heart rate <110 or >180.
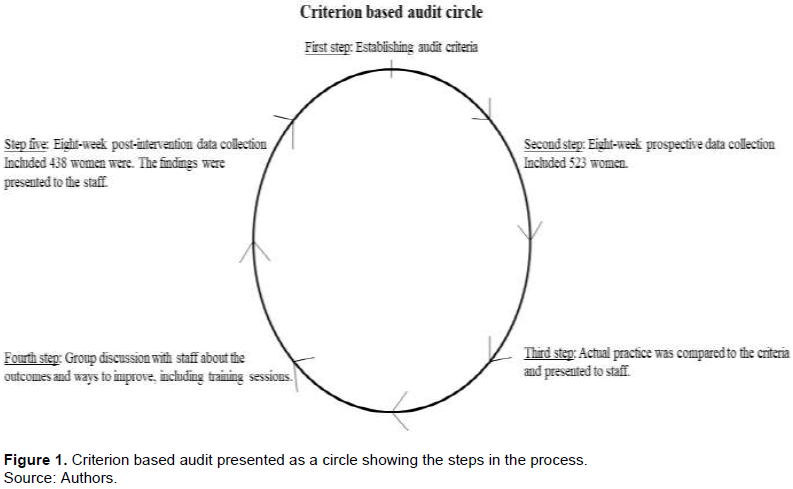
The second step of the CBA (Figure 1) was an eight-week prospective data collection from March to May 2016. It included 525 women delivering at the hospital after 28 weeks of gestation. Case files were reviewed every morning and staff were consulted for clarification of events. Two of the 525 women were excluded one because of no signed informed consent and one due to a birthweight <1000 g. A consultant in obstetrics was consulted in case of doubt when categorising the data. The delivery registry was cross-checked and the first author participated in the morning meeting all week days. Any practice not documented was assumed not done.
In step three (Figure 1) actual practice was compared to the criteria and presented to staff as frequencies of delivery outcomes and fulfilment of audit criteria.
Step four (Figure 1) was a group discussion with staff about the baseline findings and ways to improve outcomes. Furthermore, two hands-on training sessions, each lasting 1 h, were offered to all staff members with a instructor-learner ratio of one to three. The first session was about correct use of the partograph and indications for interventions. Staff were advised to avoid oxytocin administration before the action line was crossed and instead encourage the mother to eat, drink and ambulate.
Focus areas identified in the pre-intervention data collection were indications for emergency CS due to prolonged labor, suspected asphyxia and planned CS because of previous scar. Artificial rupture of membranes was advised if the alert line was crossed, and should always precede augmentation with oxytocin. The training also included hands-on training on vacuum aextraction using a pelvic and fetal mannequin and a vacuum extractor (kiwi OmniCups 747 West 4170 South Murray, Utah 84123). A Danish obstetric consultant, three Danish midwifes and the first and third authors conducted the training sessions. Before the training sessions, an Objective Structured Assessment of Technical Skills in a standardised ‘clinical scenario’ were conducted. It took place in a classroom using a partograph, pelvic and fetal mannequin and a vacuum extractor. ,Staff received points according to a structured observation list. In the scenario the woman was in labour and the partograph had to be filled in. The scenario ended in delivering the baby by using the vacuum extraction. After the training session at step four in the audit circle (Figure 1), all staff members were asked to do the same clinical scenarios again, to evaluate improvement .(Maagaard, et al., 2012). Overall, 72% of staff members participated in the tests.
In step five (Figure 1), a post-intervention data collection was carried out over eight weeks from June to August 2016. In total, 438 women were included after one was excluded, because she did not want to participate.
The findings were compared to pre-intervention data and presented to the staff.
Statitical analyses:
Data management were done using IBM SPSS Statistic 23 (SPSS Inc., Chicago, IL, USA). All categorical data were compared before and after the intervention by Chi-square with relative risk (RR) and 95% confidence interval (CI). In case of cells with less than five entries, a two-tailed Fisher’s exact test was used. Cases with missing data were excluded from comparisons. A one-way ANOVA test was used for comparing results from skills and confidence tests. A p-value below 0.05 was accepted as stastistically significant .
Ethical approval:
Permission and ethical clearance was received from the hospital’s ethical review board and the Tanzanian National Institute for Medical Research (Research Ethical Clearance Certificate No. 927).
RESULTS
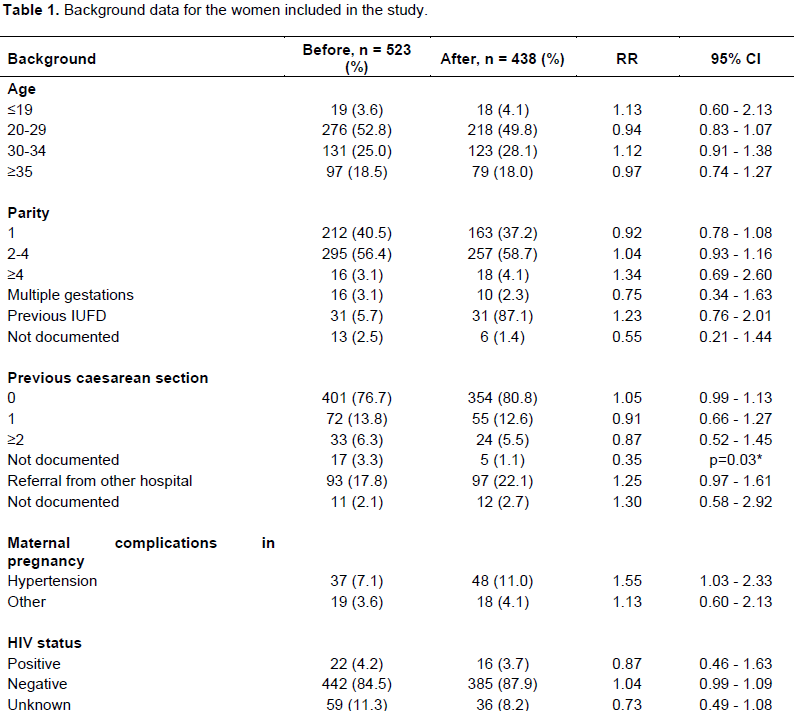
Demographic data were comparable between the pre- and post-intervention data except the frequency of registered cases of hypertension in pregnancy, which was higher in the post-intervention period (RR=1.55, CI : 1.03 - 2.33), and so was the frequency of newborns with a birthweight above 4000 g (RR=2.12, CI : 1.21 - 3.73) (Table 1).
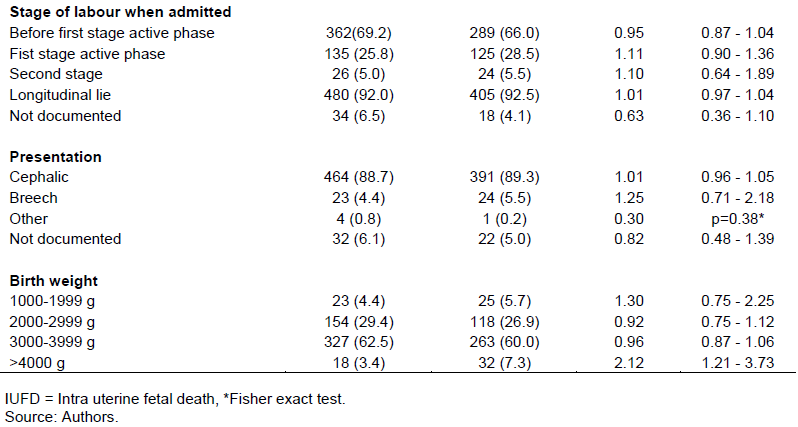
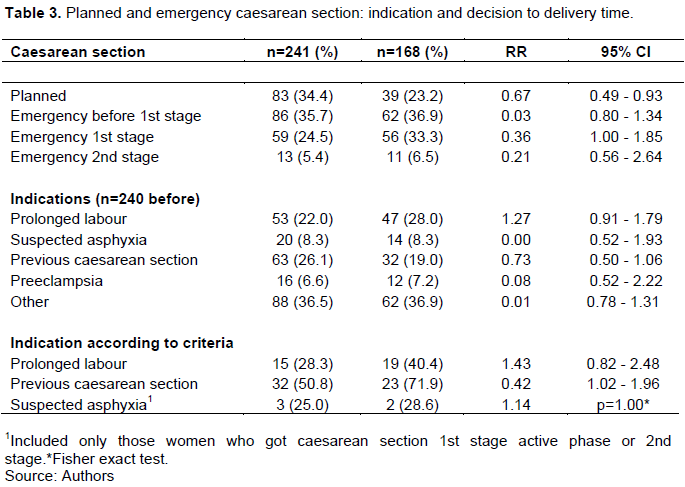
The overall CS rate decreased from 46.1 to 38.4% (RR=0.83, CI: 0.72 - 0.97) (Table 2). The main indications for CS were previous CS, prolonged labor and suspected fetal asphyxia. CS due to prolonged labor met the audit criteria in 28.3% of deliveries pre-intervention and in 40.4% post-intervention (RR=1.43, CI: 0.82 - 2.48) (Table 2). CS due to suspected asphyxia that met the criteria increased from 25.0 to 28.6% (RR=1.00, CI: 0.52 - 1.93) (Table 3).
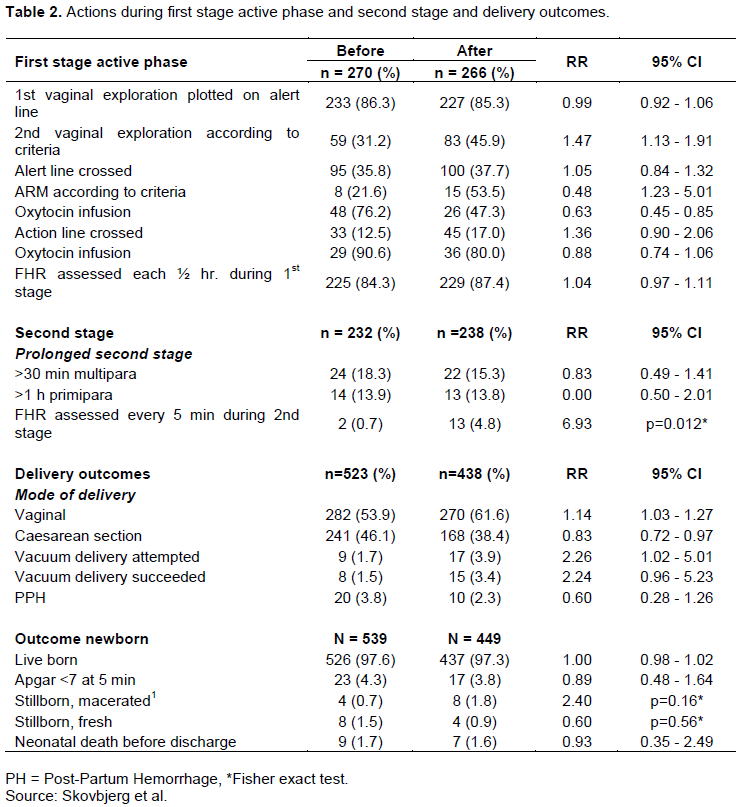
Before the intervention, artificial rupture of membranes when crossing the alert line increase from 21.6 to 53.5% (RR=2.48, CI: 1.23 - 5.01), while the use of oxytocin when crossing the alert line decreased from 76.2 to 47.3% (RR=0.63, CI: 0.45 - 0.85). Monitoring of fetal heart rate every 5 min in the second stage increased from 0.7 to 4.8% (RR= 6.93, p=0.012) (Table 2).
Attempted VE increased from 1.7 to 3.9% (RR=2.26, CI: 1.02 - 5.01). Regarding the training session and the Objective Structured Assessment of Technical Skills of the staff, mean scores for the partograph test increased from 15.7 to 19.5 (CI: 2.74 - 4.89) (maximum 26 points). In the skills test for VE the mean score increased from 8.39 to 12.06 (CI: 2.25 - 5.10) (maximum score 25 points). The mean score for confidence during VE increased from 3.7 to 4.4 (p=0.001, five= maximum score).
DISCUSSION
The use of CBA in the study demonstrated that CBA can be a usefull tool to map suboptimal care and improve outcome in low-income areas. Although the effectiveness of CBA has been reported elsewhere, it is still mainly conducted as part of research projects, in low-resource countries. (Maaloe et al., 2012a). Thus, more research is needed to explore strategies to disseminate the use of CBA, and assess its long-term effects and feasibility (Maaloe et al., 2012a). The presentation and discussion of baseline results, coupled with short training, significantly reduced the rate of CS, and CS were more often performed with an indication in accordance with the agreed audit criteria. The very high rate of CS prior to the initiation of the study can be problematic, especially as a high proportion of the performed surgeries could not be justified. The World Health Organization (WHO), states that a population-based CS rate above 10% is not associated with a decreased maternal and newborn mortality (Kabore et al., 2016). In low income settings the risk of adverse outcomes to surgery is high, as adequate staff is not available (Cavallaro et al., 2018). One explanation for he observation of a high frequency of CS may be the domino effect, as repeated CS is more likely if women had a previous CS (Vogel et al., 2015). Other documented reasons for the increasing CS rate are fear of labor pain, the impression that CS is safer than vaginal delivery, and concerns of perineal trauma (Betran et al., 2016). In this hospital based study, it was observed that many CS were performed without a sustained indication, which is consistent with other studies conducted in sub-Saharan Africa (Maaloe et al., 2012b; Kabore et al., 2016).
VE is considered a basic emergency obstetric care signal function (Ameh and Weeks, 2009) used sensibly. It can reduce CS rates and be lifesaving to newborn in second stage of labor (Ghidini et al., 2017). The proportion of vacuum deliveries in this study before intervention was similar to other observations in sub-Saharan Africa which may even be below 1% of all deliveries (Maaloe et al., 2012b, 2016). However, the training session improved the skills and use of VE significantly and contributed to the reduced CS rate. The use of oxytocin decreased following training, and artificial rupture of membranes was performed more often.
The frequent use of oxytocin without an indication has been reported by others, where 59% were given oxytocin before crossing the alert line (Maaloe et al., 2016). On the contrary, in a study from north-western Tanzania only 9% of the women with prolonged labor received oxytocin because of fear of complications (Maaloe et al., 2012b) that underlines the need to know the baseline management before planning interventions, which is met by the CBA intervention.
The WHO partograph has been questioned for its effectiveness in reducing maternal and neonatal morbi-dity and mortality (Maaloe et al., 2016), but it is still considered a central tool for monitoring progress of labor and decision-making. However, recently WHO has changed their recommendations regarding the 1 cm/h cervical dilatation due to an inaccurate way to identify women at risk of adverse birth outcomes and is therefore not recommended anymore. However, these changes were not published at the start of the study and therefore it could not be included in the inclusion criteria (Library, 2018).
Similar to these findings, other studies have investigated its use and reported substandard recording in the partograph (Maaloe et al., 2012b; Sorensen et al., 2012; Housseine et al., 2016) delayed management and interventions for example, CS done without a sustained indication (Maaloe et al., 2012a; Maaloe et al., 2016). In this study, the staff’s skills in filling the partograph, tested through a standardized test improved. However, a systematic review on the effect of training in emergency obstetric care in low-income countries suggested that knowledge and skill changes after a training session, do not necessarily result in changes in clinical performance and outcomes (van Lonkhuijzen et al., 2010).
A strength of the study was that criteria were established in cooporation with staff, making them more likely to be achievable in practice. The criteria were clear and unambiguous, minimizing the risk of bias from a subjective assessment. The data collection did not rely on obstetric specialists because the partograph was the basis for most of the data. Another strength was the low risk of selection bias since only two of the eligible women were excluded in first data collection and one woman in the second data collection.
The limitations of the study may be information bias due to underreporting, mismanagement and not documenting care given. This may have influenced the data. Secondly, it is a risk that staff in research context wants to act up to standard during the data collection period, the so-called Hawthorne effect (Graham, 2009) and the improvements are not longlasting. Thirdly, skills and confidence tests were unblinded, and performed by the investigators, which may have resulted in more positive assessment following the intervention, even though structured observation lists were used. After the intervention, we observed significantly more frequent birthweight above 4000 g and more women referred from other health facilities. This could have reduced the effect of the intervention as these parameters are correlated to higher rates of CS. Fouthly, whether the improvements may be sustained after the second data collection is unknown. But this may be crucial for such studies, and in the future, it is important to include assessment of sustainability.
CONCLUSION
The CBA including a short training session may play a positive role in improving labour management. In this study a decrease in the rates of CS and oxytocin use was demonstrated. Findings should however, be taken cautiously as other contextual factors and efforts are probably crucial for success and for long term sustainability.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Ameh CA, Weeks AD (2009). The role of instrumental vaginal delivery in low resource settings. BJOG: An internation Journal of Obstetrics and Gynaecology 116(Suppl. 1):22-25. |
|
|
Azzopardi D, Strohm B, Marlow N, Brocklehurst P, Deierl A, Eddama O, Goodwin J, Halliday HL, Juszczak E, Kapellou O, Levene M, Linsell L, Omar O, Thoresen M, Tusor N, Whitelaw A, Edwards AD (2014). "Effects of hypothermia for perinatal asphyxia on childhood outcomes. The New England Journal of Medicine 371(2):140-149. |
|
|
Bailey PE, van Roosmalen J, Mola G, Evans C, de Bernis L, Dao B (2017). Assisted vaginal delivery in low and middle income countries: an overview. BJOG: An internation Journal of Obstetrics and Gynaecology 124(9):1335-1344. |
|
|
Betran AP, Ye J, Moller AB, Zhang J, Gulmezoglu AM, Torloni MR (2016). The Increasing Trend in Caesarean Section Rates: Global, Regional and National Estimates: 1990-2014. PLoS One 11(2):e0148343. |
|
|
Brown HC, Paranjothy S, Dowswell T, Thomas J (2013). Package of care for active management in labour for reducing caesarean section rates in low-risk women. The Cochrane Database of Systematic Reviews 9:Cd004907. |
|
|
Cavallaro FL, Pembe AB, Campbell O, Hanson C, Tripathi V, Wong KL, Radovich E, Benova L (2018). Caesarean section provision and readiness in Tanzania: Analysis of cross-sectional surveys of women and health facilities over time. British Medical Journal Open 8(9):e024216. |
|
|
Ghidini A, Stewart D, Pezzullo JC, Locatelli A (2017). Neonatal complications in vacuum-assisted vaginal delivery: Are they associated with number of pulls, cup detachments, and duration of vacuum application? Archives of Gynecology and Obstetrics 295(1):67-73. |
|
|
Graham WJ (2009). Criterion-based clinical audit in obstetrics: bridging the quality gap? Best Practice and Research: Clinical Obstetrics and Gynaecology 23(3):375-388. |
|
|
Hailu D, Berhe H (2014). Knowledge about obstetric danger signs and associated factors among mothers in Tsegedie district, Tigray region, Ethiopia 2013: Community based cross-sectional study. PLoS One 9(2):e83459. |
|
|
Harrison MS, Pasha O, Saleem S, Ali S, Chomba E, Carlo WA, Garces AL, Krebs NF, Hambidge KM, Goudar SS, Kodkany B, Dhaded S, Derman RJ, Patel A, Hibberd PL, Esamai F, Liechty EA, Moore JL, Wallace D, McClure EM, Miodovnik M, Koso-Thomas M, Belizan J, Tshefu AK, Bauserman M, Goldenberg RL (2017). "A prospective study of maternal, fetal and neonatal outcomes in the setting of cesarean section in low- and middle-income countries." Acta Obstetricia et Gynecologica Scandinavica 96(4):410-420. |
|
|
Kabore C, Ridde V, Kouanda S, Agier I, Queuille L, Dumont A (2016). "Determinants of non-medically indicated cesarean deliveries in Burkina Faso. International Journal of Gynaecology and Obstetrics 135(Suppl. 1):S58-s63. |
|
|
Library WRH (2018). WHO recommendation on diagnostic test accuracy of a 1-cm/hour cervical dilatation rate threshold. February 2018. |
|
|
Mathai M, Sanghvi H, Guidotti RJ (2003). Managing complications in pregnancy and childbirth: A guide for midwives and doctors. Geneva, World Health Organization, Department of Reproductive H, Research. |
|
|
Maagaard M, Oestergaard J, Johansen M, Andersen LL, Ringsted C, Ottesen B, Sorensen JL (2012). Vacuum extraction: Development and test of a procedure-specific rating scale. Acta Obstetricia et Gynecologica Scandinavica 91(12):1453-1459. |
|
|
Maaloe N, Bygbjerg IC, Onesmo R, Secher NJ, Sorensen BL (2012a). Disclosing doubtful indications for emergency cesarean sections in rural hospitals in Tanzania: A retrospective criterion-based audit. Acta Obstetricia et Gynecologica Scandinavica 91(9):1069-1076. |
|
|
Maaloe N, Sorensen BL, Onesmo R, Secher NJ, Bygbjerg IC (2012b). "Prolonged labour as indication for emergency caesarean section: a quality assurance analysis by criterion-based audit at two Tanzanian rural hospitals." BJOG: An internation Journal of Obstetrics and Gynaecology 119(5):605-613. |
|
|
Maaloe N, Housseine N, Bygbjerg IC, Meguid T, Khamis RS, Mohamed AG, Nielsen BB, van Roosmalen J (2016). Stillbirths and quality of care during labour at the low resource referral hospital of Zanzibar: A case-control study. BioMed Central Pregnancy and Childbirth 16(1):351. |
|
|
Nolens B, Capelle M, van Roosmalen J, Mola G, Byamugisha J, Lule J, Faye A, van den Akker T (2019). Use of assisted vaginal birth to reduce unnecessary caesarean sections and improve maternal and perinatal outcomes. The Lancet Global Health 7(4):e408-e409. |
|
|
Sorensen BL, Rasch V, Massawe S, Nyakina J, Elsass P Nielsen BB (2010). Impact of ALSO training on the management of prolonged labor and neonatal care at Kagera Regional Hospital, Tanzania. International Journal of Gynaecology and Obstetrics 111(1):8-12. |
|
|
Suleiman MB, Mokuolu OA (2014). Perinatal Mortality in a Northwestern Nigerian City: A Wake up Call. Frontiers in Pediatrics 2:105. |
|
|
van Lonkhuijzen L, Dijkman A, van Roosmalen J, Zeeman G, Scherpbier A (2010). A systematic review of the effectiveness of training in emergency obstetric care in low-resource environments. BJOG: An internation Journal of Obstetrics and Gynaecology 117(7):777-787. |
|
|
Vogel JP, Betran AP, Vindevoghel N, Souza JP, Torloni MR, Zhang J, Tuncalp O, Mori R, Morisaki N, Ortiz-Panozo E, Hernandez B, Perez-Cuevas R, Qureshi Z, Gulmezoglu AM, Temmerman M (2015). Use of the Robson classification to assess caesarean section trends in 21 countries: A secondary analysis of two WHO multicountry surveys. The Lancet Global Health 3(5):e260-270. |
|
|
Welfare T. U. R. o. T. M. o. H. a. S. (2015). Emergency Obstetric and Newborn Care Job Aid. |
|
|
Yisma E, Dessalegn B, Astatkie A, Fesseha N (2013). "Knowledge and utilization of partograph among obstetric care givers in public health institutions of Addis Ababa, Ethiopia. BioMed Central Pregnancy and Childbirth 13:17. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


