ABSTRACT
This study examined the possible relationship and predictive impact of psychological distress on the quality of life among school personnel. 112 personnel employed in a private school in Caloocan City, Philippines, who participated in the study and completed the Depression Anxiety Stress Scale (DASS 21) and World Health Organization Quality of Life (WHOQOL-BREF) survey. The occurrence of severe to extremely severe level of depression, anxiety, and stress were 28.58, 17.85, and 8.93%, respectively, thus the school personnel obtained a satisfied rating in all the domains of quality of life. Correlations between the quality of life dimensions and psychological distress facets are significant at the 0.05 level of significance except for the correlation between social mean score and total anxiety score. The respondents in terms of their gender experienced the same level of psychological distress and quality of life while single employees appeared to have higher levels of depression and stress symptoms compared to married ones. Furthermore, a regression analysis demonstrated that a significant variance of 44.7% (psychological), 40.2% (physical), 8.9% (social), and 26.9% (environmental) factors of quality of life can be accounted for by psychological distress. In addition, depression and stress symptoms are found to be significant predictors of psychological and physical health, while stress is a significant predictor of social relationships and environmental domain. Therefore, the results highlight the implications for an intervention program in relieving the psychological distress and improving the quality of life among school personnel.
Key words: Depression, anxiety, stress, quality of life.
The first Mental Health Act or Republic Act 11036 has been passed in the Philippines and has a goal to create an access to comprehensive and incorporated psychological health services while protecting the rights of an individual suffering from mental health disorders as well as the members of his family (Lally et al., 2019). According to the World Health Organization and Department of Health (2012), there is only 1 doctor for every 80,000 Filipinos and one of the explanations for this scarcity of trained professionals is the emigration to English speaking countries and this shortage is magnified in the field of psychiatry wherein there is an estimated over 500 psychiatrists in practice (Lally et al., 2019), thus the ratio for mental health workers in the Philippines is 2
to 3 per 100,000 population (WHO and Department of Health, 2006). Given this scarcity of mental health professionals, more research is needed to understand the association between employees’ mental health and quality of life so that the schools can continually evaluate the needs of their employees, as well as review and improve the efficiency of their existing mental health programs.
School personnel have many life’s experiences, and their mental health is one of the determinants that may affect their working condition, hence affecting their life’s satisfaction.
Mental health is defined by the World Health Organization as an individuals’ state of well-being where an individual realizes his potential, able to work productively and fruitfully, can cope with the normal stresses of life, and has the capacity to contribute to the community (WHO, 2014). Thus, mental health should be given importance because it has a great impact on an individual’s physical health (Ohrnberger et al., 2017). The health of the mind is as essential as the health of the body. Furthermore, psychological distress is generally referred to depression, anxiety, stress, and mental health related problems (Dyrbye et al., 2010) which had been acknowledge as a vital outcome measure in several working environments (Bennett et al., 2004). In particular, stress is an inescapable part of an employees’ working life. Stress in work is a risk factor to a personnel’s health which also affects their motivation and productivity. Working conditions that are poor are crucial precursor to stress and may lead to depression or anxiety (Plaisier et al., 2007).
The working environment, changes on how the work should be done, and the mechanism of organizational behavior would definitely intensify the level of job stress among workers that could affect their physical and mental health (Dollard et al., 2003). There are many studies done especially in the education setting, that support staff, lecturers, and administration personnel have experienced job stress from moderate to high level (Jing, 2008). Also, teaching has been widely acknowledged as a profession susceptible to stress and teachers are suffering from stress related illnesses such as anxiety and depression. Stress is defined by Tripathi and Sharma (2013) as a state of psychological and physiological disparity between situational requirement and the individual's ability to meet those requirements. This comprises not only the work pressure that exceeds a person’s capability to cope but also unutilized individual’s knowledge and abilities which can transpire in a wide variety of work circumstances, but often gets worse, when there is little support from supervisors and colleagues being felt by personnel and having little or control over work and how they can cope with its pressures and demands (Ahsan et al., 2009).
Likewise, academic staffs face more problems in their work because of an increasing competition among other schools that cause an increase in duties, demands, work overload that could lead to more stress and affect their physical or mental health as well as satisfaction (Ahsan et al., 2009). Stress at work takes place when there is an imbalance between the demands of work and the individual’s capacity to carry out the said demands (Kaur, 2011). It was also found that stress is a predictor of mental health (Toussaint et al., 2016). In addition, there is an evidence of the significance of stress in the development of anxiety and depression symptoms (Hammen et al., 2009) where stress increases anxiety which in turn heightens depression (Ghorbani et al., 2008). This implies that psychological distress-namely depression, anxiety, and stress-are closely associated to each other (de Rooij et al., 2010).
Researchers have found out that stress in the academe can have a positive and negative effect if not properly managed (Smith, 2002 as cited in Ukwayi et al., 2013). In terms of work performance, career stress has a negative impact on the person and organizational commitment and individuals may be sick because of their unhealthy lifestyle (Cartwright and Cooper, 2002). A high level of stress is also related to relationships, resources, communication, control, job security (Tytherleigh, et al., 2005), overload and work life imbalance (Association of University Teachers, 2003). Furthermore, work life is one of the important parts of the daily lives of an employee which also causes a great deal of stress. A study conducted by Ofoegbu and Nwadiani (2006) found that sources of stress among non-academic staff include irregular salary payment, school interruptions and strikes, lack of instructional facilities, high cost of living, office accommodation, campus militancy, underfunding education, and lack of annual leaves.
Meanwhile, depression is a common mental disorder that manifests the general symptoms: depressed mood, disturbed sleep, loss of interest, feelings of guilt, low energy, and poor concentration (WHO, 2009) that negatively affect how an individual think, feel and also act (Parekh, 2017). An individual with depression might also present symptoms of anxiety which is a form of psychological and physiological problems that stimulate the fight or flight sensation as a right response to fear (Joshi, 2013) and this feeling of tension is combined with worries thoughts and physical changes (American Psychological Association, 2019).
In addition, another factor that is related to mental health is the quality of life. According to the World Health Organization, quality of life refers to an individual’s perception of their position in life in the context of value systems and culture in which they live and in relation to their standards, expectation, goals and concerns (WHO, 1998). The quality of life is not only limited to the psychological and physical health but also environmental and social status which can considerably contribute to the function of a person (Barcaccia et al., 2013). Studies showed that those individuals who are having lower quality of life are those who are suffering with mental health concerns (Connell et al., 2012). The following are the factors experienced by those individuals with mental health problems that contributed in lowering their quality of life: low self-esteem and confidence, lack of control, diminished activity, sense of hopelessness, demoralization, sense of not being part of society, distress, choice, and autonomy (Connell et al., 2012).
Quality of life and mental health problems of school personnel are concerns that need to be addressed since it is crucial for the learning of their students. It should be given a priority since their profession is very challenging and difficult one. They cannot do their task well if they have poor mental health. These can have an adverse effect in their life especially with their overall well-being, which includes their everyday physical, behavioral, emotional, and cognitive functioning. There are three theoretical anchorage of this study, namely Aaron Beck’s cognitive theory and model of depression, Michael Eysenck’s theory of anxiety and Hans Selye’s stress general adaptation syndrome. The present research concentration is anchored on the premise that reducing psychological distress can improve quality of life. With these, we hypothesized that faculty members have a higher prevalence of psychological distress than support staffs. On the other hand, support staffs have a higher occurrence of quality of life compared to faculty members. Also, we hypothesized that there is a negative relationship between psychological distress and quality of life among school personnel and depression, anxiety and stress predict the respondents’ quality of life.
There is dearth of local literature that focuses on the psychological distress of personnel because the studies were focused on the students’ mental health and their psychological well-being and seldom school personnel were considered priority. The result of this present research would enable to provide a thorough literature on the mental health and quality of life that would allow institutions to provide mental health programs for employees as a preventive measure to reduce further mental health issues and concerns. Furthermore, the findings will serve as a framework in proposing an intervention program for school personnel.
Research design
This study make used of a descriptive correlational design. The relationship between psychological distress-anxiety, stress, and depression and quality of life was ascertained. Further, we explored the predictive-value between psychological distress and quality of life among Filipino school personnel.
Participants
Convenience sampling was used in the study and a total of 112 out of 143 employees in a private school in Caloocan City voluntarily participated in the study wherein more than half of which are females (58.93%) and close to half are males (41.07%) with mean age of 31.40 (SD = 10.04). Close to three-quarters of them (68.75%) are faculty members and a third are staffs (31.25), while three-quarters of them are single (68.75%) and only a third (31.25%) are married. In consideration of educational attainment, majority of the participants finished tertiary education (75%), only one employee finished secondary education (.89%), less than a quarter obtained Masters Degrees (22.32%) and a small percentage of faculty members acquired PhD degrees (1.79%).
Instruments
The Depression Anxiety Stress Scales (DASS 21) is a standardized tool that has 21 items. It is a self-report questionnaire (Lovibond, 2004) that will measure the severity of core symptoms of depression, anxiety and stress; and often used in many countries (Sinclair et al., 2012). The DASS 21 contains depression scale with items related to low positive effect, hopelessness, devaluation of life, self-deprecation and inertia. The anxiety scale includes items, such as automatic arousal, feelings of fear, physiological hyperarousal, and panic attacks; and stress scale contains items like: tension, impatience, difficulty in relaxing, irritability, agitation, and over reactivity to stressful events (Gomez et al., 2014). Answers are reported using a four point Likert scale (0-3) wherein a score of 0 indicated an item “did not apply to them”, and a score of 3 which means the item “apply most of the time” (Beiter et al., 2015). A measure of general distress and three orthogonal dimensions -depression, anxiety and stress- means there is a good stability of measure, internal consistency, convergent, divergent validity, and good criterion oriented validity (Bottesi et al., 2015). The internal consistencies (Cronbach’s alpha) were high, an overall scale ranging from 0.70 and stress subscale ranging to 0.88. Meanwhile the scores on each of the three sub-scales, and the combinations of two or three of them were able to detect the common psychological distress such as depression and anxiety, with a sensitivity of 79.1% and a specificity of 77.0% at the optimal cut off of >33 (Tran et al., 2013). The DASS 21 has a clearer structure than the original version (Ronk et al., 2013), has the same factorial structure with clinical and non-clinical samples (Mahmoud et al., 2010; Sinclair et al., 2012) and the psychometric properties meet across different cultures (Oei et al., 2013; Taouk, 2001). Moreover, it is suitable for 18 years old and above (Mahmoud et al., 2010). In the present study, DASS 21 has a high level of internal consistency with the Cronbach alphas of 0.89 (depression), 0.81 (anxiety), 0.82 (stress) and 0.93 for the total scale.
World Health Organization Quality of Life (WHOQOL-BREF)
The 2nd portion of the survey is a shortened version of WHOQOL-100 and widely used for generating quality of life profile. It is a self-report questionnaire that contains 26 items categorized in four domain scores wherein each scored from 5 point likert scale. The domain scores are not averages; they are the sum total score for each question within the domain. There are seven items for physical domain (e.g., “How satisfied are you with your capacity to work?”), six items for psychological (e.g., “How often do you have negative feelings such as blue mood, despair, anxiety or depression?”), three items for social relations (e.g., “How satisfied are you with the support you get from your friends?”), eight items for environmental domain (To what extent do you have the opportunity for leisure activities?”) and there are two general questions that evaluate the overall quality of life and physical health.
Meanwhile, there are also two items that are examined separately: question 1 asks about an individual’s overall perception of quality of life and question 2 asks about an individual’s overall perception of his or her health. Also, there are three questions (3, 4 and 26) that are negatively phrased and are scored reversely. The domain scores are scaled in a positive direction wherein the higher the scores signify a higher quality of life (WHO, 1998). Multiplying the mean by 4 is used to transform the WHOQOL-BREF scores into longer form WHOQOL-100. For the analysis done, mean score for the domains are used. Transformation to a 0-100 scale was not done since comparison to WHOQOL-100 is not needed. Mean score is used so that comparison between the domains are done, removing the effect of unequal number of items per domain when using the sum. The Cronbach’s alpha in a study conducted by Teles et al. (2014) was 0.82 which can be interpreted as high which is consistent with the result of the current study wherein it acquired a high internal consistency for the total domain with the Cronbach’s alpha of 0.91 which is beyond the acceptable level. The scale for interpreting the computed mean scores of the WHOQOL-BREF was adapted from Sunga, 2019. Also, the WHOQOL-BREF domains has an acceptable level of internal consistency with the Cronbach alphas of 0.77 (psychological), 0.72 (physical), 0.60 (social), while environmental acquired 0.82 which can be interpreted as very good level of internal consistency. According to Ursachi et al. (2015), a general accepted rule is that α of 0.6-0.7 signifies an acceptable level of reliability while 0.8 or greater implies a very good level.
Procedure
A letter was sent to the school administrator, stating the request to conduct a study among school personnel. Permissions were obtained from the school personnel working in a private school to take part in the research, and it was inquired through a request letter. A total of 112 out of 143 respondents participated in the study. They were informed about the nature, purpose, and benefits of the study. Informed consent was also secured prior to data collection. Likewise, voluntary participation was considered in this research study and the principles of confidentiality of the information of the respondents were employed. Moreover, it was made certain that no harm was inflicted to the participants. The data gathered were used for research and academic purposes only. After everyone filled out the form, the first test, which was DASS 21 questionnaire, was distributed. They had 15 minutes to answer the first test. Participants were reminded to take their time in answering the test, and that there were no wrong or right answers. Next, they were asked to answer the second survey test, the WHOQOL-BREF. They were given another 15 minutes to finish the test. The data was analyzed using SPSS 21.
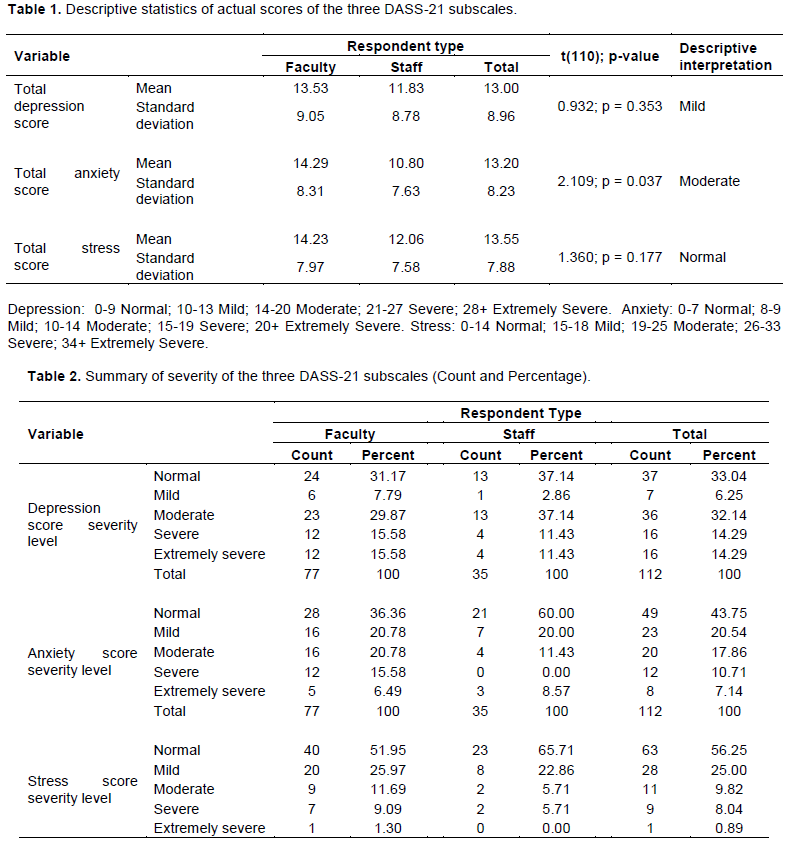
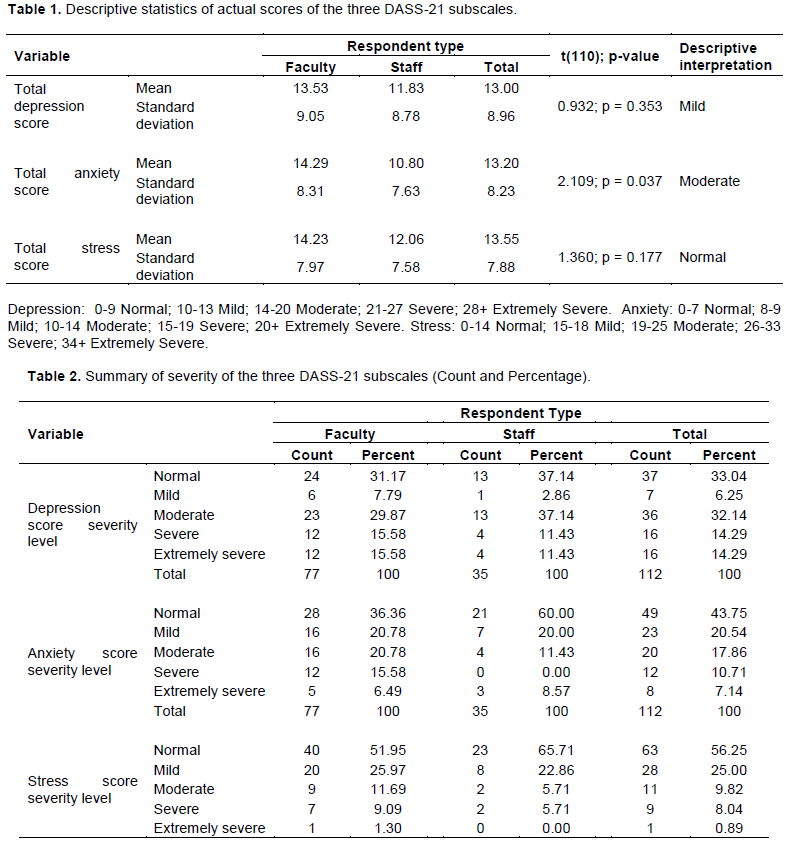
Each research question was answered using statistical analyses. A 0.05-level of significance was used for all analysis, unless otherwise stated. Table 1 shows the mean and standard deviation of the scores from the three DASS-21 subscales. In particular, faculty members garnered a higher mean score on depression, anxiety and stress compared to the support staffs. Generally, the mean score in the stress subscale is slightly higher than the two other subscales, and at the same time, scores are less dispersed under the said subscale having the smallest standard deviation. Depression (M= 13.00; SD = 8.96) fall under mild severity level, anxiety (M= 13.20; SD = 8.23) fall under moderate severity level while and stress (M= 13.55; SD = 7.88) fall under normal severity level.
To supplement the summary statistics previously discussed, the counts of the severity among faculty and staffs for each subscale are tabulated. In particular, faculty members are classified having severe to extremely severe symptoms of depression (31.16%), anxiety (22.07%) and stress (10.39%) subscale while the staff garnered 22.86% for depression, 8.57% for anxiety and 5.71% for stress. The faculty members acquired higher scores in psychological distress compared to staffs.
Generally, in the depression subscale, more than a quarter of the respondents are categorized as being Normal (33.04%), Mild (6.25%), Moderate (32.14%), Severe (14.29%) and Extremely Severe (14.29%) severity rating. Furthermore, anxiety subscale results revealed that less than a half of them falling as Normal (43.75%), Mild (20.54%), Moderate (17.86%), Severe (10.71%) and Extremely Severe (7.14%). Moreover, stress subscale results indicated that more than a half of the respondents are categorized as Normal (56.25%), Mild (25.00%), Moderate (9.82%), Severe (8.04%) and Extremely Severe rating (0.89%) (Table 2).
Table 3 shows the significant difference between the average physical mean scores of faculty and staff is observed at the 0.05 level of significance t(110)=-2.133,p=0.035). Psychological, social and environmental mean scores are found to be comparable across respondent type. For all respondents, the highest mean score observed is for the psychological domain while the lowest mean score observed is for the environmental domain. It is also noteworthy that the faculty members are satisfied with their psychological health (M=3.70: SD=0.60), physical health (M=3.50: SD=0.55), social relationships (M=3.76: SD=0.79), while the environmental factor (M=3.49: SD=0.60) garnered the lowest mean score among all the domains which can be interpreted moderately satisfied. Meanwhile, the staffs are satisfied in all the domains of the quality of life namely psychological health (M=3.86, SD=0.50), physical health (M=3.73, SD=0.49), social relationships (M=3.67, SD=0.56), and environmental (M=3.50, SD=0.49). In general, the respondents are satisfied with their psychological health (M=3.75, SD=0.57), physical health (M=3.57, SD=0.54), social relationships (M=3.73, SD=0.72), and environmental domain (M=3.50, SD=0.57).An independent sample t-test was performed in order to determine if there was a significant difference in the level and intensity of experience of the variables, namely, depression, anxiety, and stress as components of psychological distress and psychological, physical, social and environmental factors as components of quality life among the participants when grouped according to gender and civil status. No statistically significant difference was found between male and female personnel in psychological distress factors as presented in Table 4. Also, when it comes to quality of life, there is no significant difference between males and females observed for the average mean scores of the quality of life domains. For female respondents, the highest average mean score observed is for the social domain while the lowest average mean score is for the environmental domain. For male respondents, the highest average mean score observed is for the psychological domain while the lowest is still for the environmental score.

Comparing by marital status, a significant difference between the average total depression score and the average stress score of married and single individuals is observed. Average total anxiety score is found to be comparable in terms of marital status. Table 5 shows that on average, those who are single have higher levels of depression (M = 14.23, SD = 9.08) than those who are married (M = 10.29, SD = 8.19). This difference was significant, t (110) = -2.197, p < 0.05; the effect is medium-size (d = 0.46). Similarly, those who are single are more stressed (M = 14.57, SD = 8.15) than those who are married (M= 11.31, SD = 6.84). This difference is also significant, t (110) = -2.057, p < 0.05, and the effect is medium-size (d = -0.42). Thus, no significant difference is observed for the average mean scores of the four quality of life domains when compared with marital status. For married respondents, the highest average mean score observed is for the social domain while the lowest average mean score observed is for the environmental domain. For single respondents, the highest average mean score observed is for the psychological domain while the lowest average mean score is still for the environmental domain.
Correlation analyses were used to examine the relationship between psychological distress factors and aspects of quality of life. As hypothesized with the current study, the results of the analysis yielded a significantly negative correlation between psychological distress and quality of life as shown in Table 6.
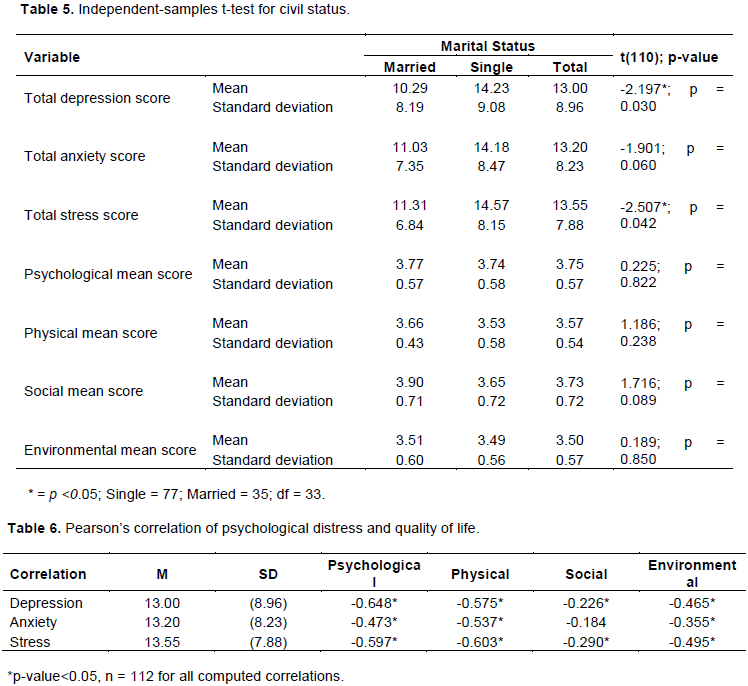
Furthermore, depression, a psychological distress factor, has a strong negative relationship for both psychological (r = -0.648, p <0.05) and physical health (r = -0.575, p< 0.05) which means that as depression levels increased, employee’s psychological and also physical health decreased. Unlike the first two domains of quality of life, the environment (r = -0.467, p<0.05) showed a moderate negative association with depression. Comparably, as depression levels increased, environmental interactions decrease, as well. However, for social relationships, a weak negative correlation was obtained (r = -0.226, p<0.05). This entails that being dissatisfied with the social relationships of employees is linked to the occurrence of depression symptoms.
Anxiety, another factor of psychological distress also has a negative correlation with different aspects of quality of life. The negative relationship between anxiety and two domains of quality of life such as psychological health (r = -0.473, p <0.05) and environmental (r = -0.355, p <0.05) were moderate. Similar to results with the depression factor, the negative association between anxiety and physical health was strong (r = -0.537, p <0.05). The results signify that the more anxious the employees are, the more that their quality of life decreases.
Moreover, scores on stress were also negatively correlated with scores on quality of life. The findings showed a strong negative relationship between stress and psychological scores (r = -0.597, p <0.05) and physical health (r = -0.603, p <0.05). Consistent with the results of depression and anxiety scores on social relationships, there is a weak negative correlation between stress and social relationships (r = -0.290, p <0.05). Inverse relationships between stress scores and environmental scores were also moderate (r = -0.495, p <0.05).
Multiple linear regression analysis was done to explore the predictive capability of the psychological distress facets scores in relation to the quality of life domain (mean) scores. Furthermore, using the enter method, it was found that depression, anxiety and stress explained a significant amount of variance in the following values of the psychological health (F(3, 108) = 29.054, p < 0.05, R2 = 0.447), physical health (F(3, 108) = 24.171, p < 0.05, R2 = 0.402), social relationships (F(3, 108) = 3.537, p < 0.05, R2 = 0.089), and environmental factor (F(3, 108) = 13.273, p < 0.05, R2 = 0.269).
Table 7 reveals that the total depression score (β =-0.030, t=-4.208, p < 0.05) and total stress score (β =-0.021, t=-2.049, p< 0.05) are found to be significant predictors of psychological mean score. In predicting physical mean score, total depression score (β =-0.016, t=-2.273, p < 0.05) and total stress score (β =-0.021, t=-2.092, p < 0.05) are found to be significant predictors while only the total stress score (β =-0.034, t=-2.067, p < 0.05) is found to be a significant predictor of social mean score. Likewise, only total stress score (β =-0.030, t=-2.665, p < 0.05) is found to be a significant predictor of environmental mean score. The fitted model has an R-squared value of 0.269, which means that 26.9% of the variability observed in social mean score is accounted for by the fitted model. Although this is better than the model for social mean score in terms of explained variability, it still lags behind the model for physical mean score and psychological mean score.
The findings of the study confirm the hypothesis that there is a significant negative relationship between psychological distress and quality of life. The results of the study revealed the factors of psychological distress that predict the quality of life of school personnel in Caloocan City specifically depression symptoms predict psychological and physical health while stress symptom predicts all the domains of quality of life. In the area of industrial-organizational psychology, work stress is a response to stimuli in a job that leads to negative effect to the people who are exposed to them (Muchinsky, 2007). The psychosomatic and mental disorders are prevalent among teachers as well as tension, fatigue, headache, and exhaustion (Scheuch et al., 2015). Teachers can develop depression (Shetageri and Gopalakrishnan, 2016) as psychological consequence of stressors at work (Chen et al., 2015). Further, there is a high level of psychological distress during professional careers (Samaranayake et al., 2014).
The prevalence of severe to extremely severe depression, anxiety and stress were 28.58, 17.85, and 8.93%, respectively among Filipino personnel. Likewise, the psychological distress such as depression, anxiety and stress are not clinical indicators of any asymptomatic disorders but these were from the normal school personnel. Psychological distress is not only limited to the Filipino personnel. For instance, Leung et al. (2009) found out that there is a prevalence of psychological distress among Hong Kong teachers, the rate in terms of severe to extremely severe symptoms of depression, anxiety and stress were 12.3, 30.3, and 38.6% correspondingly, while Bannai et al. (2015) reported that 47.8% among male and 57.8% female teachers in Japan are experiencing psychological distress.
Based on the quality of life, the present study showed that the faculty members and staffs are satisfied with all the domains of the quality of life except for the environmental factor wherein the faculty members acquired a moderately satisfied rating. Generally, the school personnel obtained a satisfied rating in all the domains. The results gathered revealed a higher satisfaction rating compared to the local study investigated by Sunga (2019). Both male and female commonly experience the same level of psychological distress and quality of life and showed that there is no significant difference in the experience of psychological distress among school personnel based on gender. Studies carried by Ofoegbu and Nwadiani (2006) and Ismail and Noor (2016) showed that stress level is significantly experience by lecturers and academician irrespective of their gender. This is mostly attributable to the fact that Filipino personnel including faculty members and staffs work under the same environmental conditions and there are no exemptions of roles in terms of work or task assignments.
Meanwhile, the major stress symptoms among academic staff are poor concentration, tiredness, headaches and career stress symptoms, which causes job satisfaction and anxiety (Ukwayi et al., 2013). The psychosomatic and mental disorders are prevalent among teachers as well as tension, fatigue, headache, and exhaustion (Scheuch et al., 2015). The teaching profession appeared to have increased risk of poorer mental health that could lead to mental health problems as compared to other jobs (Kidger et al., 2016).
The numerous responsibilities and roles played by the school’s personnel leads to increase in the significant level of stress. Also, the teaching profession is not only physically challenging but also mentally, as the teacher utilizes a great deal of energy in everyday work in the classroom in addition to his family and personal commitments (Kaur, 2011). It was found out that teaching was one of the most stressful professions in a study conducted to assess occupational stress across 26 occupations (Cooper et al., 2005). This occupational stress is ascribed to teachers work load such as planning of lessons, developing curriculum, organizing activities, managing extra-curricular activities, providing information, supervising classes, maintaining discipline and records, administering time tables, covering for teachers absences and shortages, evaluating and assessing students’ performance, motivating students in terms of actions and words (Mehta, 2013) that reduces quality of life and overall physical and mental well-being (Kaur, 2011), risk factor for depression and anxiety (Ferguson et al., 2012; Yang et al., 2011) which harm the teacher’s capacity to function at work (Borrelli et al, 2014).
As regards to marital status, those who are single appeared to have higher levels of depression and stress symptoms compared to married ones. The result is consistent with the reports presented by Mayo Clinic (2008) which indicates that unmarried women showed at a greater risk for depression. Married individuals have significantly better mental health than unmarried individuals (Palner and Mittelmark, 2002).
Researchers have found out the following factors that contributed to the stressors of the faculty members: decreased job satisfaction (Reevy and Deason, 2014), work-life imbalance (Rafeeq et al, 2015), work overload and lack of school funding and support from administration and colleague (Gupta et al., 2015), increased number of students to teach (Jamison and Enrera, 2015) which contributed increased anxiety and depression (Veena et al., 2016), feelings of inefficiency to work, and career growth dissatisfaction (Bulatevych, 2017). Furthermore, the stress that being experienced by teachers can also be linked with their work performance. It also revealed that stress can be one of the factors that affect a teacher, particularly in terms of teaching performance to their students (Zekaj, 2015).
This current study showed that psychological distress is inversely correlated with quality of life except for the correlation between social mean score and total anxiety score which acquired the same results in the study investigated by Rusli et al. (2008). This means that an increase in the psychological distress leads to the decrease of quality of life among the respondents on the following factors: social relationships, physical health, psychological and environmental domains. Specifically, depression and anxiety in the workplace are frequently linked with stress and studies showed that psychological distress are related also to poor quality of life (Chen et al., 2006; Diehr et al., 2006).
Correlations between the quality of life dimensions and psychological distress facets are significant at the 0.05 level of significance except for the correlation between social mean score and total anxiety score. Worth noting is that all variables exhibited a negative linear correlation that ranges in magnitude between moderately weak to moderately strong. This connotes that being dissatisfied with the quality of life domains is associated to the occurrence of psychological distress.
There are also studies that revealed the association between quality of life and mental health. In terms of physical health, fatigue was correlated with depression (Shetageri and Gopalakrishnan, 2016) and poor physical health was associated with depression (Besse et al., 2015) while good physical health was linked to good mental health (Bogaert et al, 2014). Quality of life implies how individual needs are met, the extent of satisfaction or dissatisfaction in several aspects of life (Costanza et al., 2007), and considered as a compound and multi-dimensional concept (Theofilou, 2013) which embedded in social, physical and cultural context (Naz et al., 2016).
Moreover, the depression and stress are found to be significant predictors of psychological and physical health, while stress is a significant predictor of social relationships and environmental domain. The results of the study agree with the findings of Rusli et al. (2008) which exposed that lower stress predicts higher perception of the quality of life. A study among teachers revealed that they relate their quality of life with professional and personal satisfaction. The following are the needs that teachers viewed to have a quality of life: stable relationship, good salary, owned a house but also meeting the needs in the workplace, accessibility, peace in the family and finances, security and physical health (Hunger et al., 2016). Further, many of these literatures acknowledge the attention from institution and school administrators to monitor and evaluate the needs of their personnel. The present research study conforms with the findings of the existing studies on the relationship between psychological distress and quality of life which strengthens the recommendation for an intervention program for school personnel for them to have a sound mental health for better quality of the life as well as good work performance.
CONCLUSION AND RECOMMENDATION
The main purpose in undertaking the correlation research study is to develop an intervention program in order to address the adverse effects of psychological distress to quality of life among school personnel. Based on the results, the researchers concluded that a negative correlation between psychological distress and quality of life was noted which explicates that as the level of psychological distress namely depression, anxiety and stress increases the quality of life specifically psychological health, social relationships, physical health and environmental domain decreases.
It is recommended that an intervention program will be provided among school personnel by focusing on equipping their knowledge and skills in battling the distress such as depression, anxiety and stress. With the said intervention program, the perceived psychological distress is reduced and the school personnel quality of life in terms of physical, social, psychological and environmental factors will be expected to improve. Mental health is a global issue, it is experienced by developed and developing country, traditional or modern country and no community is immune with this kind of problem. There is also a paucity of publish researches among Filipino personnel, thus it calls for further investigation and urges the need for an intervention program to mitigate the mental health problems among school personnel.
This study is not without limitations even though it had found out the correlation and predictive-value of psychological distress to quality of life among teachers and support staffs. The main limitation is that our respondents are limited from a private school only. The study was conducted in a single institution; hence, findings of the study would only be applied to them as well as the recommendation. Generalizability of the findings may not be evident to larger groups of school personnel. The researcher acknowledges the need for larger participants that may come from different schools or a nationwide study, if possible, may also be executed for a larger scope and to allow school personnel from different regions to have an equal representation of their current conditions. Thus, personnel living in urban areas might have different responses on the variables as compared to those personnel living in the rural areas.
The authors have not declared any conflict of interests.
The authors thank all the respondents in the study.
REFERENCES
|
Ahsan N, Abdullah Z, Fie DYG, Alam SS (2009). A study of job stress on job satisfaction among university staff in Malaysia: Empirical study. European Journal of Social Sciences 8(1):121-131.
|
|
|
|
American Psychological Association. Anxiety.
|
|
|
|
|
Association of University Teachers (2003). Survey of members. London: AUT.
|
|
|
|
|
Bannai A, Ukawa S, Tamakoshi A (2015). Long working hours and psychological distress among school teachers in Japan. Journal of Occupational Health 57(1):20-27.
Crossref
|
|
|
|
|
Barcaccia B, Esposito G, Matarese M, Bertolaso M, Elvira M, De Marinis M (2013). Defining quality of life: A wild-goose chase? Europe's Journal of Psychology 9(1):185-203.
Crossref
|
|
|
|
|
Beiter R, Nash R, McCrady M, Rhoades D, Linscomb M, Clarahan M, Sammut S (2015). The prevalence and correlates of depression, anxiety, and stress in a sample of college students. Journal of affective disorders 173:90-96.
Crossref
|
|
|
|
|
Bennett P, Williams Y, Page N, Hood K, Woollard M (2004). Levels of mental health problems among UK emergency ambulance workers. Emergency Medicine Journal 21(2):235-236.
Crossref
|
|
|
|
|
Borrelli I, Benevene P, Fiorilli C, D'amelio F, Pozzi G (2014). Working conditions and mental health in teachers: A preliminary study. Occupational Medicine 64(7):530-532.
Crossref
|
|
|
|
|
Besse R, Howard K, Gonzalez S, Howard J (2015). Major depressive disorder and public school teachers: Evaluating occupational and health predictors and outcomes. Journal of Applied Bio Behavioral Research 20(2):71-83.
Crossref
|
|
|
|
|
Bogaert I, Martelaer KD, Deforche B, Clarys P, Zinzen E (2014). Associations between different types of physical activity and teachers' perceived mental, physical, and work-related health. BMC Public Health 14 (1):1-9.
Crossref
|
|
|
|
|
Bottesi G, Ghisi M, Altoè G, Conforti E, Melli G, Sica C (2015). The Italian version of the Depression Anxiety Stress Scales-21: Factor structure and psychometric properties on community and clinical samples. Comprehensive Psychiatry 60:170-181.
Crossref
|
|
|
|
|
Bulatevych N (2017). Teacher's burnout syndrome: The phenomenologyof the process. Polish Journal of Public Health 127(2):62-66.
Crossref
|
|
|
|
|
Cartwright S, Cooper CL (2002). Asset: An organizational stress screening Tool- The management guide. Manchester, UK: RCL Ltd.
|
|
|
|
|
Chen HC, Chou FHC, Chen C, Su SF, Wang SY, Feng WW, Tsai TC (2006). A survey of quality of life and depression for police officers in Kaohsiung, Taiwan. Quality of Life Research 15(5):925-932.
Crossref
|
|
|
|
|
Chen R, Li HM, Chen DC, Gong Y, Zhu SY, Tian YL, Zhang J (2015). Prevalence and risk factors of major depression disorders in local teachers three months after lushan earthquake. Sichuan da xue xue bao. Yi xue ban= Journal of Sichuan University. Medical Science Edition 46(3):440-443.
|
|
|
|
|
Connell J, Brazier J, O'Cathain A, Lloyd-Jones M, Paisley S (2012). Quality of life of people with mental health problems: A synthesis of qualitative research. Health and Quality of Life Outcomes 10(1):138.
Crossref
|
|
|
|
|
Cooper JS, Cartwright C, Donald S, Taylor I, Millet C (2005). The experience of work related stress across occupations. Journal of Managerial Psychology 20(2):178-187.
Crossref
|
|
|
|
|
de Rooij S, Schene A, Phillips D, Rooseboom T (2010). Depression and anxiety: Associations with biological perceived stress reactivity to a psychological stress protocol in a middle-aged population. Psychoneuroendocrinology 35:866-877.
Crossref
|
|
|
|
|
Diehr PH, Derleth AM, McKenna SP, Martin ML, Bushnell DM, Simon G, Patrick DL (2006). Synchrony of change in depressive symptoms, health status, and quality of life in persons with clinical depression. Health and Quality of Life Outcomes 4(1):27.
Crossref
|
|
|
|
|
Dollard M, Winefield HR, Winefield AH (Eds.). (2003). Occupational stress in the service professions. CRC Press.
Crossref
|
|
|
|
|
Dyrbye LN, Szydlo DW, Downing SM, Sloan JA, Shanafelt TD (2010). Development and preliminary psychometric properties of a well-being index for medical students. BMC Medical Education 10(1):8.
Crossref
|
|
|
|
|
Ferguson K, Frost L, Hall D (2012). Predicting teacher anxiety, depression, and job satisfaction. Journal of Teaching and Learning 8(1).
Crossref
|
|
|
|
|
Ghorbani N, Krauss SW, Watson PJ, LeBreton D (2008) Relationship of perceived stress with depression: Complete mediation by perceived control and anxiety in Iran and the United States. International Journal of Psychology 43(6):958-968.
Crossref
|
|
|
|
|
Gomez R, Summers M, Summers A, Wolf A, Summers J (2014). Depression Anxiety Stress Scales-21: Measurement and structural invariance across ratings of men and women. Assessment 21(4):418-26.
Crossref
|
|
|
|
|
Gupta V, Rao E, Mukherjee R (2015). Occupational stress amongst faculty members: A review of literature. International Journal of Research and Development-A Management Review 4(2):18-27.
|
|
|
|
|
Hammen C, Kim EY, Eberhart NK, Brennan PA (2009). Chronic and acute stress and the prediction of major depression in women. Depression and Anxiety 26(8):718-723.
Crossref
|
|
|
|
|
Hunger MB, Morosini MC, Stobaus CD (2016). Teacher quality of life: Perspectives about their welfare. Creative Education 7(16):2363-2379.
Crossref
|
|
|
|
|
Ismail NH, Noor A (2016). Occupational stress and its associated factors among academician in a research university, Malaysia. Malaysian Journal of Public Health Medicine 16(1):81-91.
|
|
|
|
|
Jamison MR, Enrera JA (2015). Factors affecting work productivity among the female Faculty of Allied Medical Health Colleges of University of Hail, Saudi Arabia. IOSR Journal of Nursing and Health Science 4(6):25-39.
|
|
|
|
|
Jing L (2008). Faculty's job stress and performance in the undergraduate education assessment in China: A mixed-methods study. Educational Research and Reviews 3(9):294.
|
|
|
|
|
Joshi R (2013). Stress and anxiety among college going first year male and female students. Indian Journal of Health and Wellbeing 4(8):1537.
|
|
|
|
|
Kaur S (2011). Comparative study of occupational stress among teachers of private and govt. schools in relation to their age, gender and teaching experience. International Journal of Educational Planning and Administration 1(2):151-160.
|
|
|
|
|
Kidger J, Brockman R, Tilling K, Campbell R, Ford T, Araya R, Gunnell D (2016). Teachers' wellbeing and depressive symptoms, and associated risk factors: A large cross sectional study in English secondary schools. Journal of Affective Disorders 192:76-82.
Crossref
|
|
|
|
|
Lally J, Tully J, Samaniego R (2019). Mental health services in the Philippines. BJPsych International 16(3):62-64.
Crossref
|
|
|
|
|
Leung SS, WahMak Y, Yu Chui Y, Chiang VC, Lee AC (2009), Occupational stress, mental health status and stress management behaviors among secondary teachers in Hong Kong. Health Education Journal 68(4):328-343.
Crossref
|
|
|
|
|
Lovibond PF (2004). Cognitive processes in extinction. Learning and Memory 11(5):495-500.
Crossref
|
|
|
|
|
Mahmoud J, Hall LA, Staten RS (2010). The psychometric properties of the 21 Item Depression Anxiety and Stress Scale (DASS 21) among a sample of young adults. South Online Journal of Nursing Research 10:21-34.
|
|
|
|
|
Mayo Clinic (2008, June 11). Rural, Unmarried Women At Higher Risk For Depression, Study Suggests. Science Daily. Retrieved March 15, 2020 from
View
|
|
|
|
|
Mehta A (2013). A study of how emotional intelligence reduces occupational stress among teachers. International Monthly Refereed Journal of Research in Management and Technology 2:19-28..
|
|
|
|
|
Muchinsky PM (2007). Psychology applied to work (8th ed.). Belmont, CA: Wadsworth.
|
|
|
|
|
Naz S, Hashmi AM, Asf A (2016). Burnout and quality of life in nurses of a tertiary care hospital in Pakistan. Journal of Pakistan Medical Association 66(5):532-536
|
|
|
|
|
Palner J, Mittelmark MB (2002). Differences between married and unmarried men and women in the relationship between perceived physical health and perceived mental health. Norsk Epidemiologi 12(1).
Crossref
|
|
|
|
|
Oei TP, Sawang S, Goh YW, Mukhtar F (2013). Using the depression anxiety stress scale 21 (DASS-21) across cultures. International Journal of Psychology 48(6):1018-1029.
Crossref
|
|
|
|
|
Ohrnberger J, Fichera E, Suttona M (2017). The relationship between physical and mental health: A mediation analysis. Social Science and Medicine 195:42-49.
Crossref
|
|
|
|
|
Ofoegbu F, Nwadiani M (2006). Level of perceived Stress Among Lectures in Nigerian Universities. Journal of instructional Psuychology 33(1).
|
|
|
|
|
Parekh R (2017). What is depression. American Psychiatric Association.
|
|
|
|
|
Plaisier I, de Bruijn JG, de Graaf R, ten Have M, Beekman AT, Penninx BW (2007). The contribution of working conditions and social support to the onset of depressive and anxiety disorders among male and female employees. Social Science Medicine 64(2):401-410.
Crossref
|
|
|
|
|
Rafeeq M, Harish P, Shariff MI (2015). Reward management: Employee Engagement and Employee Retention are Achieved Through Motivation and Reward Factors. International Journal in Management and Social Science 3(7):294-311.
|
|
|
|
|
Reevy GM, Deason G (2014). Predictors of depression, stress, and anxiety among non-tenure track faculty. Frontiers in Psychology 5:701.
Crossref
|
|
|
|
|
Ronk FR, Korman JR, Hooke GR, Page AC (2013). Assessing clinical significance of treatment outcomes using the DASS-21. Psychological assessment 25(4):1103.
Crossref
|
|
|
|
|
Rusli BN, Edimansyah, B A, Naing L (2008). Working conditions, self-perceived stress, anxiety, depression and quality of life: A structural equation modelling approach. BMC Public Health 8(1):48.
Crossref
|
|
|
|
|
Samaranayake C, Arroll B, Fernando A (2014). Sleep disorders, depression, anxiety and satisfaction with life among young adults: A survey of university students in Auckland, New Zealand. The New Zealand Medical Journal 127 (1399):1175-8716.
|
|
|
|
|
Scheuch K, Haufe E, Seibt R (2015). Teachers' health. Deutsches Ärzteblatt International 112(20):347.
Crossref
|
|
|
|
|
Shetageri VN, Gopalakrishnan G (2016). A cross-sectional study of depression and stress levels among school teachers of Bangalore. IOSR Journal of Dental and Medical Sciences15(3):21-27.
|
|
|
|
|
Sinclair SJ, Siefert CJ, Slavin-Mulford JM, Stein MB, Renna M, Blais MA (2012). Psychometric evaluation and normative data for the Depression, Anxiety, and Stress Scales-21(DASS-21in a nonclinical sample of U.S. adults. Evaluation and Health Professions 35:259-79.
Crossref
|
|
|
|
|
Sunga A (2019). Quality of life and stress as correlate to mental health among teachers: Basis for a wellness program. Asian Journal of Multidisplinary Studies 2(1):17-30.
|
|
|
|
|
Teles MAB, Barbosa MR, Vargas AMD, Gomes VE, e Ferreira EF, de Barros Lima AME, Ferreira RC (2014). Psychosocial work conditions and quality of life among primary health care employees: A cross sectional study. Health and Quality of Life Outcomes 12(1).
Crossref
|
|
|
|
|
Theofilou P (2013). Quality of Life: Definition and Measurement. Europe's Journal of Psychology 9(1).
Crossref
|
|
|
|
|
Toussaint L, Shields GS, Dorn G, Slavich GM (2016). Effects of lifetime stress exposure on mental and physical health in young adulthood: How stress degrades and forgiveness protects health. Journal of Health Psychology 21(6):1004-1014.
Crossref
|
|
|
|
|
Tran TD, Tran T, Fisher J (2013). Validation of the depression anxiety stress scales (DASS) 21 as a screening instrument for depression and anxiety in a rural community-based cohort of northern Vietnamese women. BMC Psychiatry 13(1):24.
Crossref
|
|
|
|
|
Tripathi K, Sharma K (2013). Causes of academic stress among college students and its managements. Indian Journal of Health and Wellbeing 4(5):1161.
|
|
|
|
|
Tytherleigh MY, Webb C, Cooper CL, Ricketts C (2005). Occupational stress in UK higher education institutions: A comparative study of all staff categories. Higher Education Research and Development 1:41-61.
Crossref
|
|
|
|
|
Ukwayi JK, Uko ES, Udida LA (2013). A critical analysis of career stress among academic staff of tertiary institutions in Cross River State. Journal of Educational and Social Research 3(2):15.
Crossref
|
|
|
|
|
Ursachi G, Horodnic IA, Zait A (2015). How reliable are measurement scales? External factors with indirect influence on reliability estimators. Procedia Economics and Finance 20(15):679-686.
Crossref
|
|
|
|
|
Veena G, Pushpalatha K, Mallaiah TY (2016). Professional stress among faculty members of Mangalore University: A study. International Journal of Scientific Research and Management 4 4279-4286.
|
|
|
|
|
World Health Organization (WHO) (2014). Mental health: A state of well-being.
|
|
|
|
|
World Health Organization (WHO) (1998). Programme for mental health:WHOQOL user manual, 2012 revision. Division of Mental Health and Prevention of Substance Abuse.
|
|
|
|
|
World Health Organization (WHO) (2006). The world health report 2006: working together for health. World Health Organization.
|
|
|
|
|
World Health Organization (WHO) (2009). World Health Organization constitution: basic documents; Geneva: Available at:
View
|
|
|
|
|
Yang X, Wang L, Ge C, Hu B, Chi T (2011). Factors associated with occupational strain among Chinese teachers: A cross sectional study. Public Health 125(2):106-113.
Crossref
|
|
|
|
|
Zekaj X (2015). Impact of stress on teachers' productivity as an important factor in the increase of educational quality. Mediterranean Journal of Social Sciences 6(2S2):245.
Crossref
|
|