Full Length Research Paper

ABSTRACT
Socioeconomic factors have been identified as affecting all aspects of peoples’ lives; and it is intricately linked to the demographic process. They are strong predictors of infant and child health outcome in most developing countries. This paper examined socioeconomic determinants of under-five children health outcome with data from a sample of 609 women of childbearing age in rural and urban areas of Abia State. The study utilized explanatory study design involving survey research with a multi-stage sampling technique and a methodological triangulation of both quantitative and qualitative techniques was adopted in gathering the data. The respondents’ age was 32.6±5.8 years, 84.6% were married/living together, 55.0% had secondary education, while 42.7% were in paid/civil service jobs. Incidence of under-five mortality declined sharply as mother’s level of education increases. Urban respondents who were in paid or civil service jobs had more incidence of under-five mortality compared to their rural counterparts. The likelihood of experiencing under-five morbidity and mortality significantly reduced with higher levels of mother’s education (Odds-Ratio (OR): 0.08) and increased with paid/civil service and farming/petty trading jobs (OR: 2.35 and OR: 2.08, respectively). The outcome of an under-five child’s health depends on socio-economic factors. Maternal socioeconomic factors cannot be employed as a proxy for general social and economic change, but must be examined as important forces in their own rights.
Key words: Under-five health outcome, socioeconomic, childbearing mothers in Abia State.
INTRODUCTION
Infant and child mortality rates are sensitive indicators of health status of a community. This is because more than any other age-group, the survival of infants and children depends on the socio-economic conditions of their environment (Madise et al., 1999). It has also been observed that under-five children’s health outcome is vital for evaluation and planning of the public health strategies in a particular country (Park, 2005). They are composite indices reflecting environmental, social, economic, health care services and delivery situation, on the one hand, and maternal as well as family and community norms and practices on the other (Jamal Uddin et al., 2009). The importance of mother’s education for child health has been well demonstrated (Kabubo-Mariara et al., 2009; Ruel et al., 1992). According to Mosley and Chen (1984), maternal education affects children’s health and nutritional outcomes through its effect on improving women’s socioeconomic status. In turn higher socioeconomic status affects a set of “proximate determinants” of health that directly affect the health and nutritional outcomes of children.
Although, there has been a substantial reduction in infant and child mortality rates in most developing countries in the recent past, childhood mortality remains a major public health issue in developing countries where it is estimated that over 10 million preventable child deaths occur yearly (WHO, 2005). Progress in the reduction of infant and child mortality remains a problem facing sub-Saharan Africa in particular. With reference to Nigeria, available statistics suggest that infant and child mortality levels continue to be high, with wide geographic disparities (NPC, 1998; NPC, 2004).
Every day on average, more than 26,000 children under the age of five die around the world; and nearly all of them, live in developing countries (UNICEF, 2008). More than one-third of these children die during the first month of life, usually at home and without proper nutrition and basic commodities that might save their lives. In Nigeria, about one million children under-five die every year (DFID, 2009). The infant mortality rate was 69 per 1,000 live births for the five years preceding the 2013 NDHS, the child mortality rate was 64 per 1,000 children surviving to age 12 months, and the under-5 mortality rate was 128 per 1,000 live births. This implies that one in 15 Nigerian children die before their first birthday and one in eight die before their fifth birthday (NPC and ICF, 2014). Under-five mortality rate in the South-eastern part of the country was reported to be to be 103 per 1,000 live-births by FMOH (2009).
In spite of the high level of schooling in the southern part of Nigeria, under-5 mortality is relatively higher in the South-east, which includes Abia State, compared to South-south and South-west (NPC and ICF, 2014). This is far above the MDGs’ targets of 76 under-five deaths per 1,000 live births by 2015. Reducing these deaths is a crucial step to advancing Nigeria’s progress towards Millennium Development Goal 4. In spite of the fact that major childhood diseases have been identified and modern technology to combat them have been developed, Nigerian children still die in large numbers from these diseases. No fewer than 240,000 newborn babies die annually in the country as a result of poor nutrition (Ezeaka, 2014). Nigerian Health Policy recognizes the need to reduce the current high infant and childhood morbidity and mortality rates; but, mothers’ socioeconomic positions have not been adequately integrated into the health intervention programmes. It is evident that adequate social research attention has not been given to the issues of socioeconomic factors which play a vital role in a child’s health outcome in the South-eastern Nigeria. It is against this background that this work investigates socioeconomic determinants of under-five children health outcome in Abia State.
Brief literature review
Education has been identified as affecting all aspects of people’s lives; and, it is intricately linked to the demographic process (Isiugo-Abanihe, 2003). Other reports have shown that maternal education is a significant factor influencing child survival (Caldwell, 2009; Osonwa et al., 2012). Hossain et al. (2002) supported a direct causal relationship between mother’s education and child mortality. Waters et al. (2004) observed that mother’s education is positively associated with a number of measures of infant and child health and nutritional status. Mothers’ place of residence (urban-rural distinction) has been used in some developing countries as a proxy measure for living conditions to illustrate both public and medical health provisions (Suwal, 2001). Place of residence (rural/urban) and geographical location (region) may also affect the utilization of ANC services. Abor and Abekah-Nkrumah (2009) revealed that urban dwellers might be relatively closer to healthcare facilities than rural dwellers in most developing countries. The findings of UNIFEM (2000) conclude that economic empowerment of women comes with the courage to stand up against husbands and partners, parents and in-laws, to assert their rights to decide whether and when to have sex, to resist violence, to make household decisions, or bear and care for children. Studies have also shown that greater household income and assets directly raise the ability to purchase sufficient quantities of nutritious foods, clean water, clothing, adequately-ventilated housing, fuel for proper cooking, safe storage of food, personal hygiene items, and health services (Boyle et al., 2006; Hong et al., 2006). On the other hand, it has been shown that women’s employment may have at least one disadvantage: the survival of young children appears to be negatively affected if women work (Basu 1991; Kishor, 1992).
Studies have shown a remarkable difference in mortality rates by residence. In 2008 NDHS report, under-five mortality rate for the 10-year period, before the survey, in urban areas is 121 deaths per 1,000 live births compared to 191 in rural areas, while 2013 NDHS reported infant mortality is 43% higher in rural areas (86 deaths per 1,000 live births) than in urban areas (60 deaths per 1,000 live births). The urban rural difference is even more pronounced in the case of under-5 mortality (NPC and ICP Macro, 2009; NPC and ICF, 2014). In a study in Bangladesh, it has been shown that infant mortality is higher for boys than for girls but child mortality is lower for boys (Kabir and Chowdhury, 1992). Also earlier study has shown that for the first year of life mortality is higher for males than females (United Nations, 2006). It has been documented that children from poor households are more vulnerable to many avoidable environmental threats to health, compared with children born to better off families (WHO, 2000). They are at greater risk of severe diseases, and are more likely to suffer from more than one disease when ill. In most countries, they are less likely to have access and use preventive and curative interventions; and, those who do receive treatment are less likely to receive appropriate quality services (Wagstaff et al., 2004).
For the purpose of this research, the Mosley and Chen’s analytical framework and Socio-ecological model were adopted. As posited by them in the article, Mosley and Chen observed that so many proximate determinants may be directly influenced by a mother’s education to radically alter chances for child survival. According to Glanz et al. (1997), socio-ecological model provides a set of conceptual and methodological principles, drawn largely from systems theory, for organizing comprehensive, community-based health promotion initiatives. Ecological models specific to health promotion are multifaceted, targeting environmental, behavioural, and social policy changes that help individuals make health choices in their daily lives.
Methods of data collection and analysis
The study utilized explanatory study design involving survey research with a multi-stage sampling technique in selecting a sample size of 609 women drawn from the three Senatorial Districts of Abia State (Abia North, Abia Central and Abia South). In each of the Senatorial Districts, a total of 203 questionnaires were distributed. The procedures adopted in the selection of the respondents were as stated below:
Stage 1: The first stage involved the simple random selection of two Local Government Areas (LGAs) each from the three Senatorial Districts. The LGAs selected were Bende/Umunneochi, Umuahia North/South and Aba North/South.
Stage 2: This stage involved purposive selection of Umuahia North, Aba North and Aba South LGAs each form the three Senatorial Districts to represent urban areas, while Umuahia South, Bende and Umunneochi LGAs were selected to represent rural areas based on their ecological factors.
Stage 3: The third stage adopted the simple random sampling of six roads/streets each from the urban centres and three communities each from the rural areas, using the lists provided from each of the LGAs.
Stage 4: In the fourth stage, a systematic selection of ten buildings each from the eighteen selected roads/streets following the allotted building numbers by the state government, and a random selection of twenty buildings from the nine rural communities were employed.
Stage 5: The final stage of the procedure was the purposive selection, from a selected building, of a woman who had given birth to at least one child in the last five years that preceded the study. In each selected building, if more than one woman had given birth to at least a child, a simple random technique was employed to select one person for the study. The questionnaire was administered by face-to-face interview; this increased the response rate and ensured that all the questionnaires were returned.
In addition to the quantitative survey data, qualitative data were collected involving In-depth Interviews (IDIs) and Focus Group Discussions (FGDs). Participants were purposively selected through contact, and convenient dates to conduct the interview were agreed. A total of ten participants, who had experienced child birth in the last five years, from different socio-economic backgrounds with emphasis on their age categories were selected and interviewed in the IDIs sections from each of the selected urban and rural areas of the State. On the other hand, the FGDs conducted were carefully organised by selecting women within the reproductive age bracket of 15-49 years and of various age groups categorized as young, mid, and old women. An interview guide provided guidelines for the conducts of IDIs and FGDs. The language of the interview was either English language or Igbo language depending on the literacy level of the interviewee or the focus group. The sample size for the survey research was calculated using Cochran’s statistical formula for calculating minimum sample proportion. The minimum sample size needed to estimate the prevalence of under-five mortality to within 5% of the estimate of 157 per 1,000 (NPC and ICP Macro, 2009). At a 5% level of significance using the formula below:
N= (Zα)² × pq
d²
Where:
N = Minimum sample
Zα = Standard score: 1.96 (Assuming a level of error of 5%)
p = Prevalence of outcome measure: 0.157 (under-five mortality)
q = 1-p = 1-0.157 = 0.843
d = Absolute deviation: 5% = 0.05 (this mean that the estimate for under-five mortality is within 5% from the assumed true rate). Assuming a prevalence rate of 50%
N = 203 × 100
50 N = 406.
The sample size for the study was increased by 50% (N= 609) to allow for statistical analysis of different variables and direct estimation of mortality in the study area. The study population comprised women within the child bearing age range of 15-49, that had given birth to at least one child in the last five years irrespective of socioeconomic background. A methodological triangulation of both quantitative and qualitative techniques was adopted in gathering the data. This comprised the utilization of documentary sources, structured interviews (questionnaires), 20 IDIs and 6 FGDs with minimum of 7 participants each. Statistical Package for Social Sciences (SPSS) version 21.0 was used for quantitative data analysis at univariate, bivarite and multivate levels. Logistic regression model was used to predict the influence of infant nutrition on under-five health outcome. As regards the qualitative data, thematic manual content analysis was used for data collected from the in-depth interviews and FGDs by sorting and codifying the major themes as well as the use of verbatim quotation. The reason was to understand holistically the generated results from quantitative assessment.
Ethical approval was obtained from the Review Committee of the Federal Medical Centre (FMC), Umuahia which reviewed the proposal, questionnaire, and consent form before providing the clearance. All study subjects participated voluntarily and gave informed consent; no participant suffered physical or emotional harm as a result of the study; the study did not disclose participants’ names or addresses.
RESULTS
Socio-demographic characteristics of the respondents by residence
The socio-demographic characteristics of the respondents are displayed in Table 1. The mean age of the respondents was 32.6 ± 5.8 years. There was no much difference between the mean ages of the respondents from rural and urban areas, with 32.4 ± 6.3 and 32.6 ± 5.3 years, respectively. This indicates that most women in the sample were in the prime child bearing age. As regards the marital status of the respondents, the majority of the respondents (84.6%) were married and living together with their spouses. Data on educational attainment revealed that the largest proportion (55.0%) had secondary education followed by 29.9% with tertiary education. Nearly the same scenario was observed for their husbands’ educational attainment. There was a disparity in educational attainment by placeof residence, with 61.3% of rural respondents having received secondary education relative to about 49% of urban respondents; while 39% of urban women had tertiary education; only 21% of rural women had tertiary education.
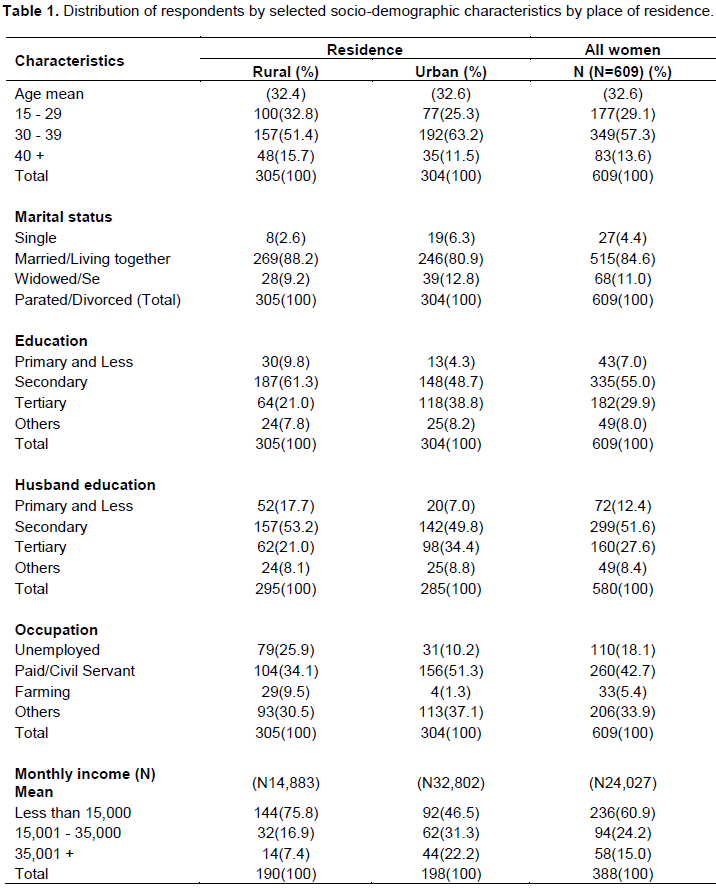
Data on occupation of the respondents revealed that the largest proportion (42.7%) of them were in paid/civil service jobs with disparity between urban and rural areas as the majority (51.3%) of urban residents were in paid/civil service jobs compared to 34.1% of rural respondents; 25.9% of rural respondents were unemployed compared to 10.2% urban respondents. Only 5.4% of the respondents were engaged in farming (9.5% in rural area and 1.3% in urban area) an indication that the zeal for farming has declined in the area, which is not unconnected with the high level of educational attainment in Abia State. In all, the mean monthly income was N24,027, N14,883 in rural area and N32,802 in urban area. The disparity in the mean monthly income of the respondents in the areas is expected as a result of the gap in educational attainment and occupation of urban and rural respondents.
Respondents’ previous under-five mortality experience
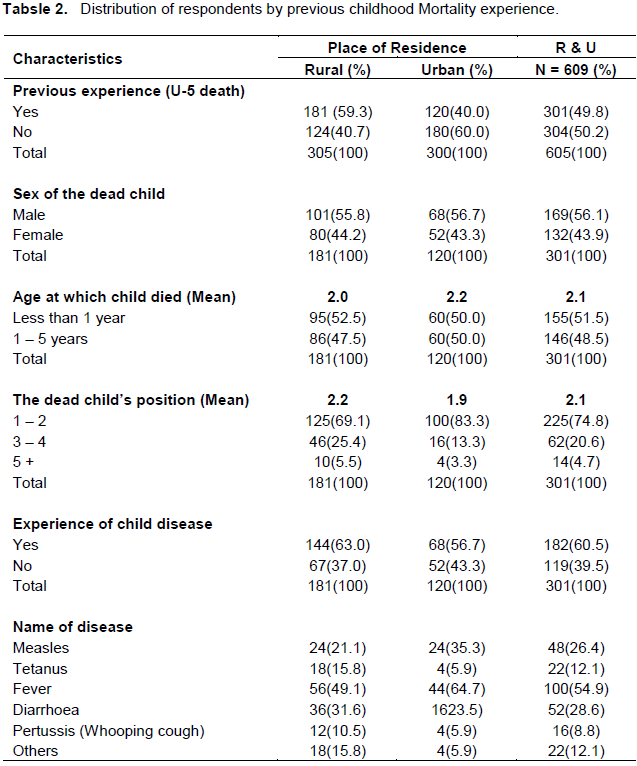
Table 2 shows previous experience of under-five mortality of the respondents. The result showed that the mean number of children born alive was 3.1 ± 1.5 children. There was little difference in the mean number of children between urban and rural respondents (3.0 and 3.2, respectively). About one-half of the respondents (50%) had experienced under-five mortality in the study area with substantial difference between rural (59.3%) than urban (40.0%) areas. The majority (56.1%) of under-five mortality recorded were male children. A little above half of the respondents (51.5%) experienced infant mortality, with little differences between urban and rural areas. Data on the dead child’s position is an indication that the complications and strange experiences related to first-two pregnancies could be contributory factor to childhood mortality. This is line with some respondents’ opinions that first pregnancy experience was excruciatingly painful and uncomfortable. Some of the respondents put their opinions their way:
I resorted to personal remedies to strange development in my husband’s absence during my first pregnancy. At a time, l was fed up with the pregnancy until l finally gave birth to the child, though he passed away after some months (Urban FGD, respondent aged 27, Umuahia North LGA).
Another respondent posited that;
... it is not easy to be a woman. This was my comment the first time l was pregnant for my dead child. In fact, both my husband and I became confused at a point. I thank God for saving my life because it was totally as if l was in another realm during that period (Rural IDI, respondent aged 26, Umunnaochi LGA).
On the experience of babies’ ailments, Table 2 shows that majority (60.5%) of the under-five mortality involved a particular disease before the eventual death of the child. Similar situation was observed for urban and rural locations in this regard. Among the children who had some ailments, the majority (54.9%) had fever, followed by 28.6% that had diarrhoea and 26.4% that had measles. A large proportion of urban (64.7%) relative to rural (49.1%) under-five deaths was associated with fever before their deaths.
Distribution of respondents who have experienced under-five mortality by some selected demographic characteristics
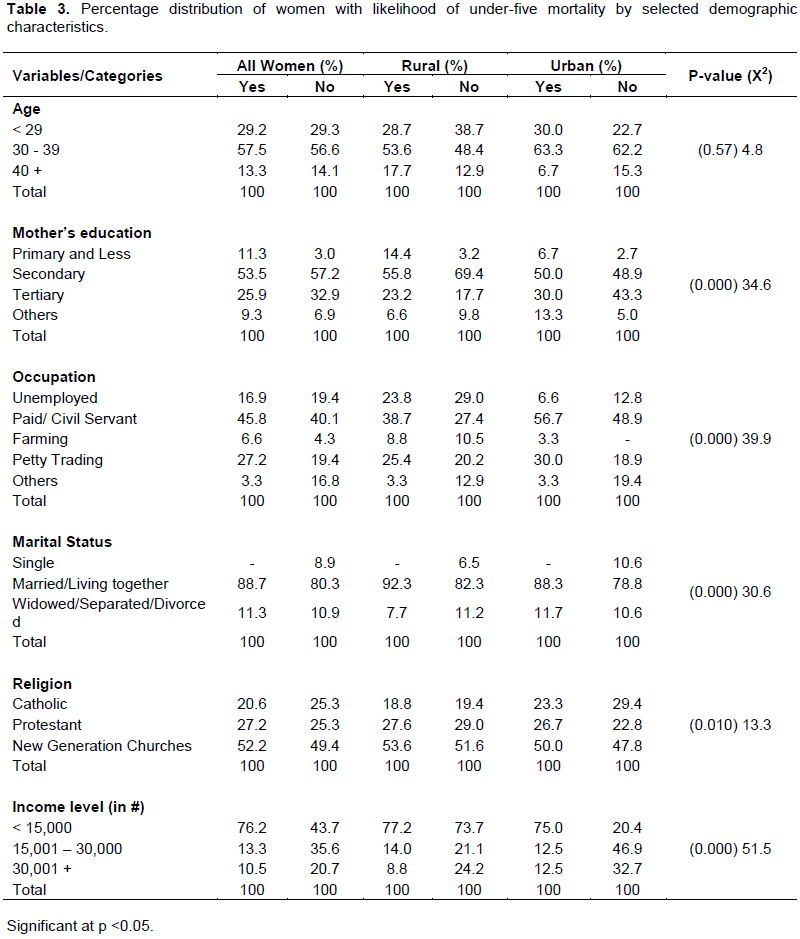
From Table 3, it is observed that incidence of under-five mortality was high among women aged 30 to 39 years in the area. It is worth mentioning that the result is expected considering the mean age (32.5 years) of respondents for the study. Higher levels of educational attainment are generally associated with lower mortality rate. Table 3 further shows that respondents with primary and less education had higher incidence of under-five mortality compared with those that reported not to have had such experience. About 33% of the respondents with tertiary education did not experience under-five mortality compared to about 26% with such incidence. Non incidence of under-five mortality differed substantially between urban and rural areas; and it was in urban areas than in rural areas for all categories. More urban (13.3%) than rural (6.6%) women who had vocational and informal education experienced childhood mortality. The result aforementioned could probably be attributed to economic hardship associated with urban areas. It is not surprising that the result revealed that mothers’ occupation have a significant (p<0.000) influence on infant and child mortality. Regarding the occupation of the respondents at present, the incidence of under-five mortality was slightly lower among women for unemployed category. For these women, the help received from their husbands and extended family members could be a function of the low experience of under-five mortality. Some respondents who were unemployed maintained that their family members sometimes shower them with gift items for their babies’ upkeep. Some of the assertions are couched this way:
...my husband and extended family members were of immense help to me when l was nursing my baby. Since l do not have any job for now, my husband, mother, mother-in-law, siblings, etc. make sure that l do not lack anything. I was even advised to always breastfeed mybaby since there was enough food for me (Urban FDG, respondent aged 28, Umuahia North LGA).
Another respondent posited that:
It is really good to have a husband and family members that have that understanding spirit. I got married immediately after my university education without working for money. My sweetheart (husband) and family members have always been there for me anytime (Rural FGD, respondent aged 35, Umuahia South LGA).
A larger proportion of the respondents (45.8%) in paid/civil service jobs had incidence of under-five mortality. Though, the results differ substantially between urban and rural areas, as the majority of urban respondents (56.7%) compared with about 39% of their rural counterparts for the same category had incidence of under-five mortality. The implication is that paid/civil service jobs place higher demands on their workers that they become resilient. This is supported by the submission made by an urban respondent during an in-depth interview:
I make sure that my baby is breastfed in the morning before I leave for my office and my mother takes care of the baby till I return from work. I would have loved to breastfeed my baby all the time, but the situation that I am faced with could not allow me (Urban IDI, respondent aged 43, Aba North LGA).
There is a significant relationship (p<0.00) between mothers’ marital status and incidence of under-five mortality. The case of under-five mortality was higher amongst respondents who were married/living together and widowed/separated/divorced in the area study. The little difference amongst the women by place of residence could be a function of economic pressure faced by urban single parents to cater well for their children and other household needs which invariably affect the health statuses of family members. On the other hand, the respondents who reported to be single never experienced incidence of under-five mortality. The Table further reveals that the majority of New Generation Churches’ members (52.2%) had incidence of under-five mortality in the last five years compared with their counterparts in other religious groups in the study area. The chi-square analysis in the Table shows that there is a significant relationship between mothers’ religion and under-five mortality. There was no much variation by residence on the experience of under-five mortality by religion. The high childhood mortality rates associated with members of New Generation Churches might be attributed to their level of fanaticism in the area. It validates the consensus submission made by rural and urban women during one of the FGDs that:
It is clear that without strong faith in God, individuals could not depend on their own thoughts for survival. I leave some of my household problems to God for His pre-eminence. In most cases, when my children are sick, I commit them into God’s hands since they may not know the problems they are having’ (Rural FGD, respondent aged 39, Umunnaochi LGA).
Another informant from the rural area stated that:
The bible has made us to understand that by His strip we are healed. So, l see no reason why l should be afraid in the face of my children’s ailment. Remember that the same bible told us that whatever we believe comes to us. To me, the first thing l do as a believer when my children are sick is to hand their sickness over to God and believe that they are strong (Urban FGD, respondent aged 35, Umuahia North LGA).
Under-five mortality experience was high amongst households into the lowest wealth quintile and reduces as households’ income increases. Over two-thirds of the respondents with the lowest wealth quintile, that is, less than N10,000, reported having incidence of under-five mortality. It is not surprising that the chi-square analysis showed a significant relationship between mothers’ income and child’s health outcome.
Multivariate analysis of selected socio-demographic factors influencing incidence of under-five mortality
Logistic regression is appropriate in this case since the dependent variable is dichotomous (binary) as a respondent either had a child that died before age 5 years or not. Having dead under-five is coded 1, else equal to 0. This design therefore, makes the model probabilistic and the interest was to predict the likelihood (odd) of under-five mortality most suitable for logit regressions. In order to ease interpretations, some reclassifications were made to reduce the number of categories of some responses especially when the numbers of respondents that chose such options are very few. Also, the parameter estimates are reported in the odd ratio format so that the percentage by which each of the factor categories contributes to the likelihood of under-five mortality can easily be ascertained.
The incidence of under-five mortality as the dependent variable was examined within the respondents’ socio-demographic factors including age, marital status, educational attainment, occupation, number of children, and residence through multivariate analysis involving logistic regression.
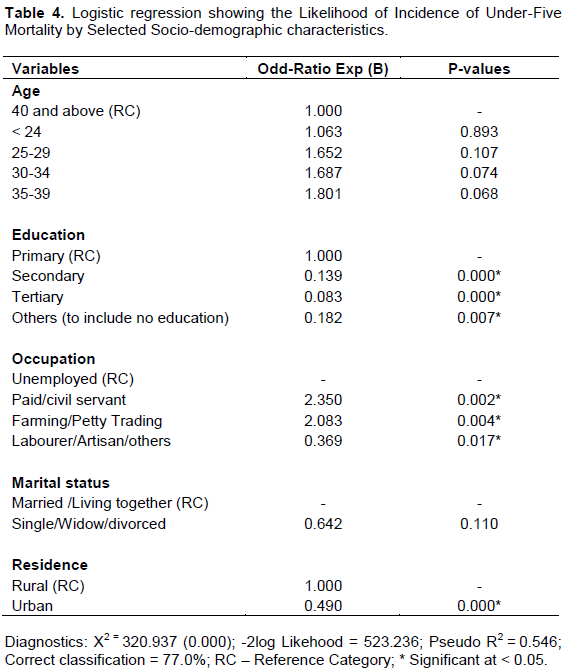
Table 4 showed the results of the logistic regression analysis of the influence of socio-demographic factors on the incidence of under-five mortality. The finding shows the influence of age on the experience of under-five mortality. The respondents aged less than 40 years were more likely to experience under-five mortality than their counterparts in the age group 40 and above. Level of education also influenced the incidence of under-five mortality in the study areas. Those with secondary, tertiary and ‘other’ category education were less likely to have experienced of under-five mortality than those with primary education (the reference category). Also, women with tertiary education are less likely to have experienced under-five mortality relative to those with secondary education. Results on occupation of the respondents showed no relationship between their type of jobs and under-five mortality. The single/widowed/ divorced respondents were 0.642 times less likely to experience infant mortality than those who are married/living together (the reference category). The relationship between the respondents’ place of residence and incidence of under-five mortality conformed to expectations. Those that resided in urban areas were 0.490 times less likely to have under-five mortality than their rural counterparts (the reference category). However, the possibility of having the experience of under-five mortality may decline as negative consequences for the health and welfare of children in rural area are adequately tackled.
DISCUSSION OF FINDINGS
The study reveals that most women in the sample were in the prime child bearing age. The fact that a few respondents were single reflects the high value the Igbo place on marriage and the social stigma associated with having children outside wedlock. There is a high level of educational attainment among the respondents and their partners, which may be partly responsible for the low rate of separation and divorce, and the stability of marital union in Abia State. There was a disparity in educational attainment and monthly income by place of residence. The largest proportion of the respondents were in paid/civil service jobs, a function of the high level of educational attainment in Abia State, which has given rise to the neglect of farming activities.
Incidence of mortality was high in the area with a substantial difference between rural than urban areas. The result validated the findings that revealed a higher under-five mortality in rural than urban areas (NPC and ICP Macro, 2009; NPC and ICF, 2014). The incidence of childhood disease before the eventual death of the child was high in the study area. More than half of these children who died before age 5 died at 2 years and were males. This is in line with earlier studies which show that for the first year of life mortality is higher for males than females (United Nations, 2006; Kabir and Chowdhury, 1992). It was revealed that the mean age at birth of the said children by the women in the sample was high. There is relatively a low number of children ever born to all women.
The study revealed a non-significant association between respondents’ age and incidence of under-five mortality. Incidence of under-five mortality declined sharply as mother’s level of education increases. The result buttresses the studies of Waters et al. (2004) and Boyle et al. (2006) that mother’s education is positively associated with a number of measures of infant and child health and nutritional status. Also, the above finding may be explained by Isiugo-Abanihe’s (2003) in observation that education has been identified as affecting all aspects of people’s lives and it is intricately linked with the demographic process. The effect of occupation by residence on under-five children’s health was interesting. Urban respondents who were in paid or civil service jobs had more incidence of under-five mortality compared to their rural counterparts. This finding implies that empowering women through wage work takes them outside their homes. Women’s employment may have at least one disadvantage: the survival of young children appears to be negatively affected if women work (Basu, 1991; Kishor, 1992). The qualitative results revealed that the slightly lower incidence of under-five mortality among women for unemployed category was contingent upon the help received from their husbands and extended family members. This is in line with submission of Boyle et al. (2006) and Hong et al. (2006) that greater household income and assets directly raise the ability to purchase sufficient quantities of nutritious foods, clean water, clothing, adequately-ventilated housing, fuel for proper cooking, safe storage of food, personal hygiene items, and health services. More urban than rural women who had vocational and informal education experienced childhood mortality could probably be attributed to economic hardship in associated with urban areas. The incidence of under-five mortality was slightly lower among women for unemployed category. For these women, the help received from their husbands and extended family members could be a function of the low experience of under-five mortality.
Both the quantitative and qualitative results revealed that a low level of income among poorer families with many children obviously leads to inadequate nutrition and/or food availability, which perpetuates malnutrition. This, in turn, accelerates high levels of infant morbidity and mortality. The aforementioned result could be explained by Abor and Abekah-Nkrumah’s (2009) that wealth is expected to have a positive relationship with ANC since the use of the service is associated with the cost of consultation and the purchase of recommended medication alongside other indirect costs such as transportation cost which could affect both maternal and child’s health. The relationship between the respondents’ place of residence and incidence of under-five mortality conformed to expectations. Those that resided in urban areas were less likely to have under-five mortality than their rural counterparts. This finding conforms with the fact that mothers’ place of residence (urban-rural distinction) has been used in some developing countries as a proxy for living conditions to illustrate both public and medical health provisions (Suwal, 2001).
Childhood mortality is a touchy issue to mothers themselves, who usually feel out of place due to the emotional trauma caused by such deaths. The major limitations encountered during the conduct of this research were the unwillingness and reluctance of some respondents to open up by giving all necessary information. However, a major bias was the failure to incorporate men in the study, considering their influence on the utilization of maternal and child health care utilization, and under-five mortality. As a result, there is need for a thorough exploration for both comprehensive quantitative and qualitative studies that will incorporate men to elicit needed information on the roles of men.
CONCLUSION AND RECOMMENDATIONS
The study revealed a high incidence of under-five mortality with rural respondents 19.3% more likely than those that are resident in urban areas to lose their children before age 5. This is attributed to imbalance in the distribution of health facilities in Abia State. The mean age of the dead child is 2 years. In all, male under-five children recorded higher prevalence of death compared to their female counterparts. Generally, it was established that under-five health outcome among people of Southern Abia State, Nigeria is invariably tied to child bearing women’s socioeconomic factors which was corroborated by the qualitative findings. There is need for government to embark on a comprehensive package that caters for both pregnant women and under-five children. However, economic depression besetting much of the nursing mothers in the study area and the country at large must not be allowed to decelerate or reverse the progress that has been made towards reducing under-five mortality. Increasing women’s participation in key decision-making processes in employment and political life is also critical to improving maternal and newborn’s health. Improving economic status can be vital to enhancing women’s participation in decision-making, with attendant implications for the health of their children.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interest.
ACKNOWLEDGEMENTS
The authors acknowledged the Ethical Review Committee of the Federal Medical Centre (FMC), Umuahia which reviewed the proposal, questionnaire, and consent form before providing the clearance to conduct the research. We also thank our research assistants who assisted us in the collection of data. We also appreciate and thank all the women who participated in the study.
REFERENCES
|
Abor J, Abekah-Nkrumah G (2009). The socio-economic determinants of maternal health care utilization in Ghana; Submitted to African Economic Research Consortium. |
|
|
Basu AM, Basu K (1991). Women's economic role and child survival: The case of India. Health Transition Rev. 1(1):83-103. |
|
|
Boyle M, Racine Y, Georgiades K, Snelling D, Hong S, Omariba W, Hurley P, Rao-Melacini P (2006). "The Influence of Economic Development Level, Household Wealth and Maternal Education on Child Health in the Developing World." Social Sci. Medicine 63:2242–54. |
|
|
Caldwell JC (2009). Education as a Factor in Mortality Decline: An Examination of Nigerian Data. Population Studies, vol. 33(3):395-414. |
|
|
Ezeaka C (2014). In Maternal and Infant Nutrition. The Nation. |
|
|
Federal Ministry of Health (FMOH). (2009). Saving newborn lives in Nigeria: Newborn health in the context of the Integrated Maternal, Newborn and Child Health Strategy. Abuja. |
|
|
Glanz K, Lewis ML, Rimer BK (1997). Health behaviour and health education. San Francisco, CA: Jossey- Bass. |
|
|
Hong R, Banta J, Betancourt J (2006). Relationship between Household Wealth Inequality and Chronic Childhood Under-nutrition in Bangladesh. International Journal for Equity in Health, 5:15. |
|
|
Hossain MZ, Yadva KNS, Hossain MK (2002). Determinants of Infant and Child Mortality in Bangladesh, J. Statistical Stud. 22:1-12. |
|
|
Isiugo-Abanihe UC (2003). Male Role and Responsibility in Fertility and Reproductive Health in Nigeria. Ibadan: Centre for Population Activities and Education for Development (CEPAED). |
|
|
Jamal Uddin MD, Zakir Hossain MD, Ullah MO (2009). Child Mortality in a Developing Country: A Statistical Analysis, J. Appl. Quantitative Methods, 4(3):270-283. |
|
|
Kabir M, Chowdhury RI (1992). Infant and child mortality levels and trends Secondary analysis of the 1989 BFS data. National Institute of Population Research and Training. Dhaka, Bangladesh. |
|
|
Kabubo-Mariara J, Ndenge GK, Mwabu DK (2009). "Determinants of Children's Nutritional Status in Kenya: Evidence from Demographic and Health Surveys." J. Afr. Econ. 18(3):363–87. |
|
|
Kishor S (1992). All 'Devis' but not all wanted: A district-level analysis of female discrimination in India, 1961–81. Paper presented at the 1992 annual meeting of the Population Association of America, Denver, Colorado. |
|
|
Madise NJ, Matthews Z, Margetts B (1999). Heterogeneity in Child nutritional status between households: a comparison of six sub-Saharan African countries. Population Stud. 53:331-343. |
|
|
Mosley WH, Chen LC (1984). "An Analytical Framework for the Study of Child Survival in Developing Countries." Population and Development Review 10(Supplement): 25-45. |
|
|
National Population Commission (NPC) and ICF Macro. (2009). Nigeria Demographic and Health Survey 2008: Key Findings. Calverton, Maryland, USA: NPC and ICP Macro. |
|
|
National Population Commission (NPC) [Nigeria]. (1998). 1991 Population Census of the Federal Republic of Nigeria: Analytical Report at the National Level. Lagos, Nigeria: National Population Commission. |
|
|
National Population Commission (NPC) [Nigeria]. (2004). National Policy on Population for Sustainable Development. Abuja: Nigeria: National Population Commission. |
|
|
National Population Commission (NPC) [Nigeria] and ICF International. (2014). Nigeria Demographic and Health Survey 2013. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF International. |
|
|
Osonwa OK, Iyam MA, Osonwa RH (2012). Under-Five Mortality in Nigeria: Perception and Attitudes of the IKWERRES in Rivers State towards the Existence of "OGBA – NJE". J. Sociological Res. 3(2):1948-5468. |
|
|
Park K (2005). Preventive Medicine in Obstetrics, Paediatrics and Geriatrics, In PARK'S textbook of preventive and social medicine, (18th edition) India: BHANOT. |
|
|
Ruel MT, Habicht JP, Pinstrup-Andersen P, Grohn Y (1992). "The Mediating Effect of Maternal Nutrition Knowledge on the Association between Maternal Schooling and Child Nutritional Status in Lesotho." Am. J. Epidemiol. 135(8):904-14. |
|
|
Suwal JV (2001). "The Main Determinants of Infant Mortality in Nepal." Social Sci. Medicine, 53:1667-1681. |
|
|
United Nations (UN). (2006). "Sex Differentials in Life Expectancy and Mortality in Developed Countries: An Analysis by Age Groups and Causes of Death from Recent and Historical Data." Population Bulletin of the United Nations 25:65–106. |
|
|
United Nations Children's Fund (UNICEF). (2008). The State of the World's Children. New York: UNICEF. |
|
|
United Nations Development Fund for Women (2000). Progress of the World's Women 2000 UNIFEM Biennial Report. New York. |
|
|
Waters H, Saadah F, Surbakti S, Heywood P (2004). "Weight-for-age Malnutrition in Indonesian Children, 1992–1999." Int. J. Epidemiol. 33(3):589–95. |
|
|
Wagstaff A, Bustreo F, Bryce J, Cleason M (2004). Child health: reaching the poor. Am. J. Public Health. 94:726-736. |
|
|
World Health Organization (2000). Health inequalities and the health of the poor: What do we know? What can we do? Bull WHO 2000, 78:3-17. |
|
|
World Health Organization (WHO) (2005). World Health Report: Make every mother and child counts. Geneva: The World Health Organization. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


