Full Length Research Paper

ABSTRACT
Lower levels of adherence to antiretroviral therapy (ART) among older adolescents as compared to adults are influenced by individual, psychosocial, and treatment-related factors. Successful transition of older adolescents into HIV adult care from paediatric & adolescent focused care requires an understanding of barriers to ART adherence. This study aimed at determining individual factors affecting ART adherence among older HIV positive adolescents transitioning to adult care. Between December 2018 and January 2019, we conducted a cross-sectional study among 82 perinatally infected adolescents aged 16-19 years in an HIV care and treatment clinic in Nairobi, Kenya. We used completed structured questionnaires and abstracted data from clinical charts. We performed multivariate logistic regression to identify factors independently associated >95% self-reported ART adherence (7-day recall). The study participants had a median age of 17 (IQR 16,18) on ART for a median duration of 11 years (IQR 7,13). Sixty-four per cent (52) of the adolescents reported optimal adherence was of >95%, and 15% reported missing doses for three or more months. Self -reported adherence had a high correlation with viral loads of <1000 copies ml (Kappa= 0.087). Adolescents with high self-efficacy were eight times more likely to report adherence of >95% [OR 8.1, 95% CI (2.31- 28.18)]. Once a day, dosing was also independently associated with adherence [OR 1.58, 95 %CI [0.62-4.08].
Conclusions: The reduction of ART pill burden and the inclusion of assessment of ART self –efficacy may contribute to transition preparedness among adolescents..
Key words: Transition, adolescents, HIV, adherence, antiretroviral therapy, self-efficacy.
INTRODUCTION
There are approximately 1.3 million adolescents (10-19 years) living with HIV (ALWHIV) in Eastern and Southern Africa (1)and nearly 300,000 adolescents and young adults (15-25 years) are living with HIV in Kenya majority of whom acquired HIV during the perinatal period (UNAIDS, 2016). To achieve the UNAIDS goal of ensuring 95% of people living with HIV (PLWHIV) achieve viral suppression, older adolescents must remain motivated to continue adherence to ART as they gain independence and begin to practice self-management (UNAIDS, Nations, & UN Joint Programme on HIV/AIDS (UNAIDS) 2014).
Psychosocial, socio-demographic, individual, and treatment-related factors, (Adejumo et al., 2015)influence optimal adherence and consequent virological suppression and decreased mortality. Conversely, poor adherence can lead to poor clinical outcomes, increased chances of transmission and a higher probability for the development of drug resistance (Haberer et al., 2011), (Slogrove et al., 2017). Globally, viral suppression, retention to care and adherence to antiretroviral therapy (ART) among older adolescents (15-19 years) is lower than that of adults and children (Lamb et al., 2014) (Carrizosa et al., 2014).
HIV care services in many subâ€Saharan African countries are distributed between specialised paediatric and adult clinics (Adejumo et al., 2015). A successful transition of the adolescent to adult care (defined as ‘the purposeful, planned movement of adolescents and young adults with chronic physical and medical conditions from childâ€centred to adultâ€oriented health care systems) (Carrizosa et al., 2014) often means that the adolescents must possess the motivation to continue to adhere to life-long ART.
Despite the large numbers of older adolescents living with HIV, compared to data on adults, there is a lack of data on adolescent patient factors, such as self-efficacy (Naar-King et al., 2006), medication-related factors (Biadgilign et al., 2009) (Adejumo et al., 2015), and social factors, such as social support and their influence on adherence (Reda and Biadgilign, 2012) (Van Dyke et al., 2002).
Understanding these modifiable individual clinical, psychosocial and socio-demographic factors could provide valuable insights during the development of interventions aimed at improving adherence among transitioning adolescents. This study aimed at determining the individual-level, socio-demographic, clinical and psychosocial factors affecting adherence to ART among older HIV positive adolescents transitioning to adult care.
METHODOLOGY
Study site and design
A cross-sectional study was conducted between December 2018 and January 2019 within a large urban HIV care and treatment outpatient clinic that currently provides treatment to approximately 300 adolescents. This facility was purposively selected as it provides HIV care to a large cohort of paediatrics who were in the process of transitioning to adult care.
This process of transition in this clinic includes the identification of adolescents between the ages of 16 and 19 years, followed by an assessment of their readiness by evaluating viral load measures in the past year and a psychosocial support counselling session. If considered ready, the adolescents progress from the adolescent clinic days to receiving clinical reviews on adult clinic days. The goal of the transition is that the adolescents should be able to navigate the pharmacy, phlebotomy and clinician interactions without the aid of a caregiver.
Inclusion criteria for the study were: a) Perinatal HIV infection, b) Ages 16-19 years, c) ART use for at least three years. Perinatal infection was confirmed through 1) review of clinic records for HIV DNA results within the postnatal and infancy period or 2) by using proxies such as duration of more than three years on ART and documented HIV status of the mother where available. Proxies were used to determine perinatal infection where documentation of infant PCR or child HIV antibody testing confirmation was lacking in the clinical notes.
Study procedure and data collection
140 adolescents were screened. Out of these, 18 adolescents did not fit the study criteria as there was no documentation of perinatal infection. An additional 40 could not be enrolled as their caregivers were unavailable for obtained consent. Therefore, 82 study participants who met the study inclusion criteria during their routine clinic appointments were identified. After enrolment to the study, data were collected through abstraction of patient hospital records, including lab results and questionnaires collected using computer-assisted self -interviewing. Blood samples of 5 ml were collected from adolescents who did not have a recent viral load result recorded in the previous three months in the patient records. Research assistants were non-clinical and had not interacted with the study participants before.
Data collection
Baseline demographic data and clinical data such as duration of ART use, duration of enrolment in care, self-reported adherence, viral load and age at disclosure were collected. Data on stigma experiences, perceived social support system, ART adherence self-efficacy and reported self-esteem were also collected. Demographic and psychosocial variables were collected using a structured computer-assisted self-interviewing survey and utilised through chart abstraction for clinical data collection. Viral load results were valid if measured three months prior to the interview date.
Measures
Adherence
A previously validated self-report adherence tool was used for adolescents and paediatric living with HIV previously used in the Paediatric AIDS Clinical Trials Group. (Van Dyke et al., 2002). This tool utilised the number of missed doses. An adherence level of ≥95% is recommended to achieve optimal viral suppression (World health organization, 2006). 95% adherence was computed as no more than one dose a month for those on a once a daily ART regimen and no more than three doses a month for those on twice a day regimens. For this study, a treatment break as a period of three months or more of not taking any ART was also defined.
ART adherence self-efficacy
Self-efficacy was measured using a previously validated HIV-Adherence self-efficacy assessment survey (HIV-ASES) tool consisting of a 12 item scale measuring the level of patient confidence to carry out relevant ART related behaviours (Johnson et al., 2007). Responses range was from 1 (cannot do it at all) to 10 (absolute can do it). HIV-ASES cut-off for this study was determined by assessing the performance (specificity and sensitivity) of different cut-off values using Receiver Operating Characteristics (ROC) analyses.
Self-esteem
Self-esteem was measured using the validated Rosenberg 10-point scale that measures global self-worth. All items are answered using a 4-point Likert scale format ranging from strongly agree to disagree (ROSENBERG SELF-ESTEEM SCALE, 1965). A score <25 indicated low self-esteem, whereas a score >35 indicates high self-esteem.
Perception of social support
Social support was measured using one question from the previously validated shortened social provisions scale. “Is there someone with whom you can discuss important decisions or challenges you face related to your HIV status?” (Perera, 2016), (Caron, 2013). The social provisions scale measures the level, type and perceived satisfaction with social support from one’s social network. This question was selected as it assesses the integration construct; an individual’s integration of their HIV status and treatment into social support circles which was an area of exploration in this study.
Stigma
Stigma was measured using the question, “Have you experienced stigma (people treated you differently) after learning of your HIV status?”. This is a question adapted from the 40-point HIV stigma scale. This question focuses on the assessment of experienced stigma, which was explored in this study.
Data analysis
Descriptive statistics were used to characterise study variables. Four factors associated with adherence were assessed and Chi-square was utilised for categorical variables and Kruskal Wallis test for difference in means during bivariate analysis. Regression analysis was then used for variables found to have a significance of p≤0.3 and regression models were used to examine the independent associations between self-reported adherence and 1) clinical (age at disclosure, frequency of ART regimen), 2) psychosocial (stigma, social support, adherence self-efficacy and self-esteem) and 3) socio-demographic (age, sex, schooling, caregiver status) variables. The Kappa statistic measure was used to examine agreement between self-reported adherence and viral load. For adherence of self-efficacy, area under ROC curve of 89.5 had a sensitivity of 74% and specificity of 67%. Therefore, a cut-off score of <90 was used to describe low self-efficacy. Cronbach’s alpha reliability coefficient was conducted to measure the internal consistency of the items (variables) in the HIV-ASES and Rosenberg self-esteem scales.
Regression analysis was used to determine independent associations between adherence and the clinical, psychosocial and demographic variables. All analyses were conducted using StataCorp. 2013. (Stata Statistical Software: Release 13. College Station, TX: StataCorp LP. Stata version 13).
RESULTS
Baseline characteristics
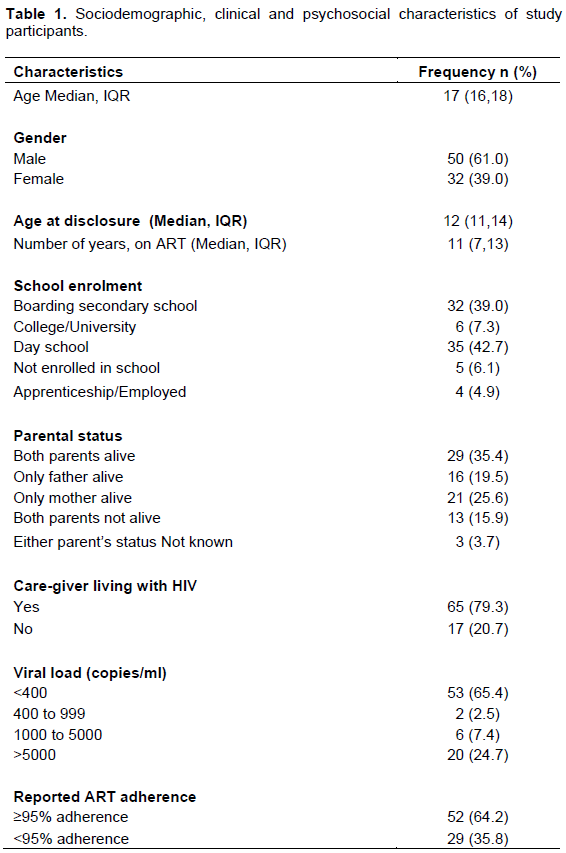
The adolescents in the study had a median age of 17 (IQR 11, 14) and 61% of them being male. Sixty-one per cent were male. Most adolescents had been on ART for a median of 11 years (IQR 7, 13) while the median age at disclosure was 12 years (IQR 11, 14). Almost 65% of the adolescents had lost one or both parents or did not know their whereabouts, and 39% attended a boarding school. Using a cut off >1000 viral copies/ml for viral suppression, 32% of the adolescents achieved viral suppression and 15% reported at least one treatment break. Self-reported adherence of ≥95% adherence was reported by 64% of the participants. Overall, 65% of the adolescents were on twice a day ART regimens compared to 34.6% (28) who were on once-a-day regimens (Table 1).
HIV treatment adherence self-efficacy score
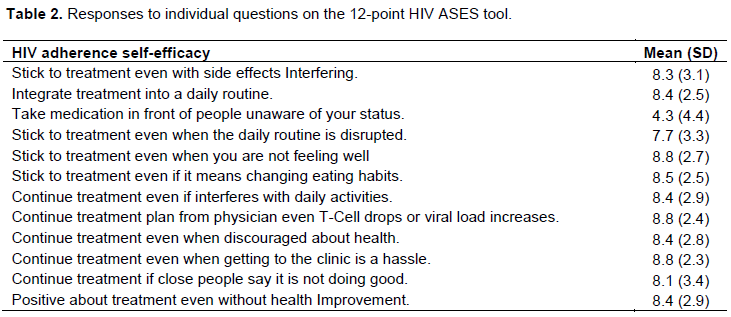
Overall, the study participants demonstrated high confidence in most of the areas related to the integration of treatment into their daily life, particularly on sticking to treatment even they were not feeling well or when the viral load increased (Table 2). The lowest score was self-reported efficacy on the use of medications in the presence of people unaware of their HIV status. Adolescents also scored low on ART adherence self-efficacy when their daily routine was disrupted. The composite score mean (SD) was 8.1 (1.8). Using computed ROC cut off (≥90), 68% of participants scored a high self-efficacy (Table 2). Cronbach’s alpha was 0.832, which indicates a high level of internal consistency (reliability) for the self-efficacy scale.
Self-esteem
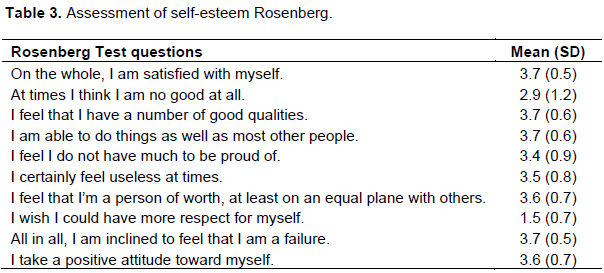
Most of the study participants demonstrated high confidence in most of the areas related to their adherence to ART, particularly on capability do things as well as most other people, inclination towards the feeling of being a failure and the perception of having a number of good qualities. The lowest score was related to the perception of respect for self (Table 3). a high internal consistency of the self-esteem items in the scale (Cronbach’s alpha= 0.714) was reported. Self-esteem composite mean (SD) was 3.4 (0.4).
Adherence
There was a high level of agreement (Kappa statistic = 0.087) between self-reported adherence and viral load (<1000 copies/ml). This high correlation indicated that self-report used in this study was a reliable measure of adherence.
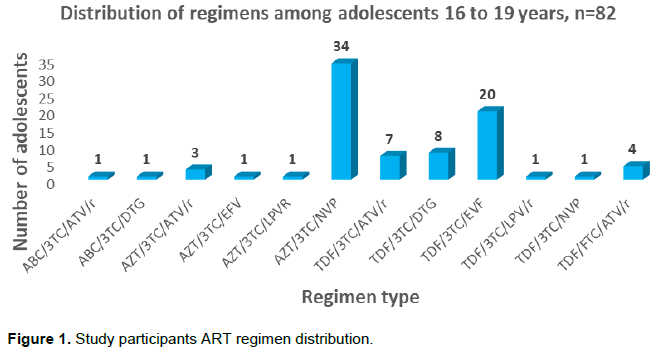
The most common regimen was Zidovudine/ Lamivudine/Nevirapine combination (41.4%), followed by Tenofovir/Lamivudine/Efavirenz at (24.3%) (Figure 1).
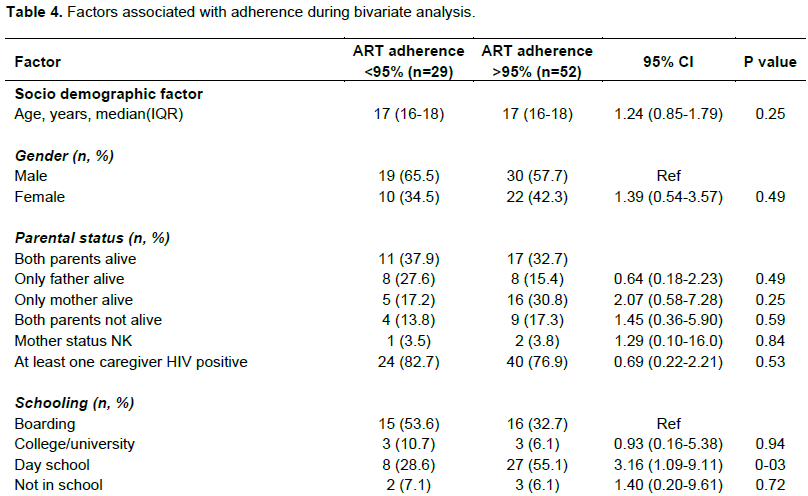
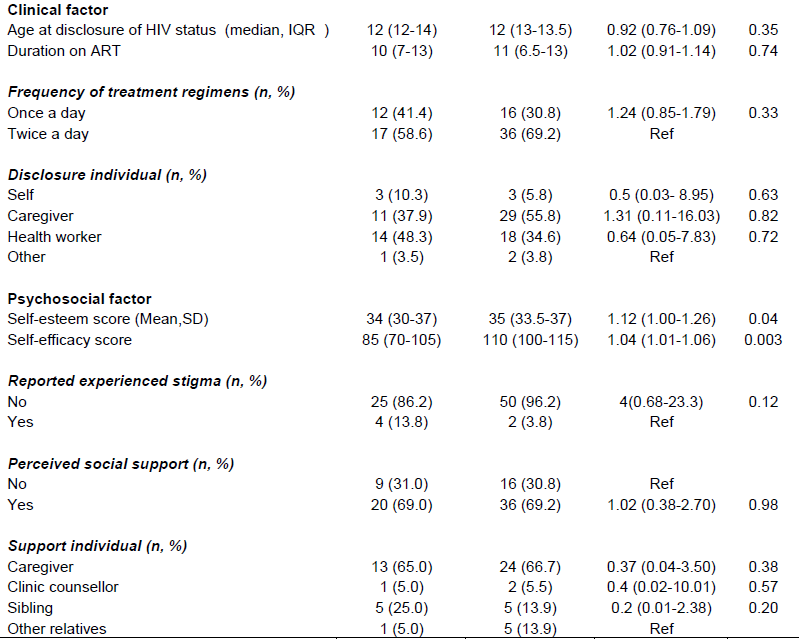
During bivariate analysis, factors significantly associated with self-reported of adherence of >95% were ART self-efficacy (p<0.01), self-esteem (p=0.04) and attending boarding school (p=0.03). There were no significant differences according to age or sex (Table 4).
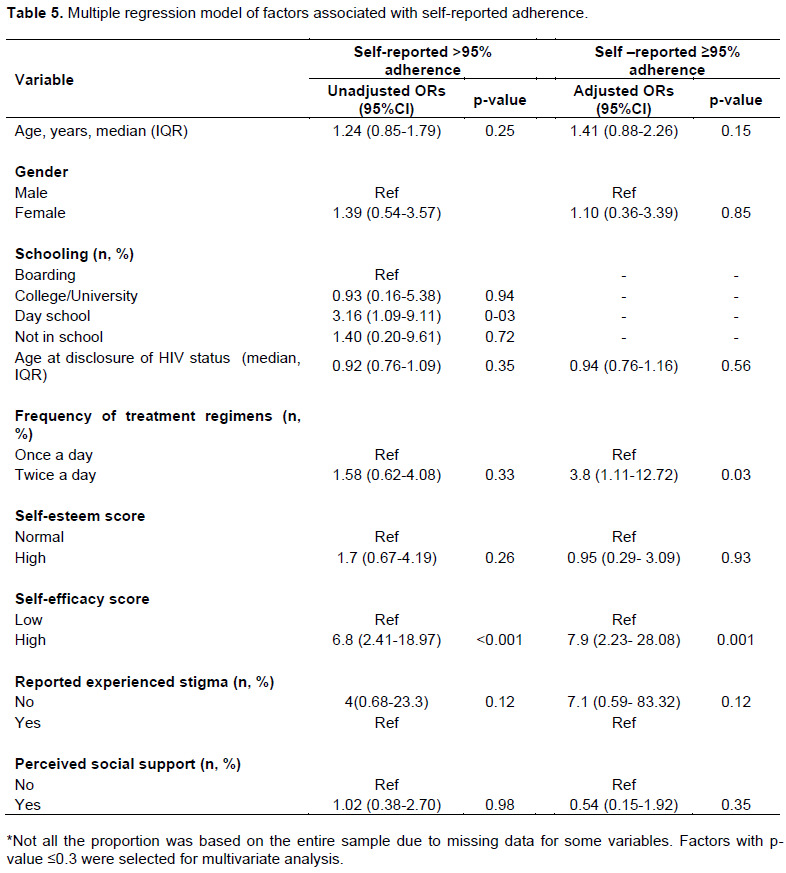
The multivariate model predicting self-reported adherence >95%
Older ALWHIV with high ART adherence self-efficacy were eight times more likely to report high adherence [OR 7.9, 95% CI (2.23-28.08)] and those on a twice a day ART regimen were almost four times more likely to report adherence [OR 3.8, 95% CI (1.11-12.72)]. Self-esteem, age, sex, schooling, perceived social support and experienced stigma were not found to be associated with adherence among these older adolescents (Table 5).
DISCUSSION
The findings indicate that reported adherence among older adolescents transitioning to adulthood is still suboptimal. In this study, high ART adherence self-efficacy and use of twice a day regimens were independently associated with high adherence. This is the first study to our knowledge that has explored modifiable psychosocial factors such as self-efficacy and self-esteem and their association to adherence among adolescents to sub-Saharan Africa.
Only a little over two-thirds of the adolescents reported adherence ≥95%. It was postulate that lack of privacy may have contributed to this finding and in particular, institutionalisation such as living in boarding schools. Lack of privacy is a strong determinant of non-adherence in other studies in this region ((MacCarthy et al., 2018) (Damulira et al., 2019). The data from the assessment of ART self-efficacy in our study supports this argument. Adolescents scored lowest during the assessment of their ability to adhere to ART in the presence of individuals who did not know their status.
Social support and particularly caregiver relationships is a significant contributor and influencer of health behaviours such as drug adherence ((Damulira et al., 2019). However, in our study, caregiver support was not significantly associated with better adherence. The study criteria of older adolescents in this study (16-19 years), compared to the broader age range in other studies (10-19 years) may have contributed to this difference as older adolescents often display a greater desire for autonomy and detachment from caregivers compared to younger adolescents (Daddis, n.d.). In this study, the number of doses was significantly associated with adherence. This is a finding supported by previous studies (World Health Organization - HIV and Adolescents from Guidance to Action,” n.d). Guidelines of transitioning of adolescents include switching to once a day regimens where possible. In this study, adolescents had been on ART for almost a decade, and factors such as adverse effects and ART resistance-associated treatment failure may have resulted in the reported twice a day dosing regimens (Purwaningsih et al. 2019), (Tyer-Viola et al., 2014). Additionally, this study was conducted before the introduction of once a day dosing regimens that incorporate newer integrase inhibitors such as Dolutegravir to the Kenyan national guideline for use in transitioning ALWHIV (National AIDS & STI Control, 2018).
Our findings that self-esteem was not associated with adherence were an exciting finding since in adolescence developmental stage, self-esteem is a critical component in decision making and behavioural outcomes Educación, et al., 2012). There are scarce data on self-esteem in HIV positive adolescents in sub-Saharan Africa. However, studies (Educación et al., 2012) in Indonesia (Purwaningsih et al., 2019), North America (Tyer-Viola et al., 2014) and Pakistan (Kurniawan and Fitrio 2019) have found associations. There is data indicating that self-esteem may be a mediator of non-health self-efficacy (Nader, 2014) and that both are components of self-concept this interplay may have led to this variable being knocked out in the multiple regression model.
There is a wealth of research (Profile et al., 2001, Nieuwkerk and Oort, 2005) indicating that self-efficacy (one’s sense of being able to adhere to ART and adhering to clinic appointments) is a significant contributor to improved adherence and better treatment outcomes in Adults living with HIV. (Aregbesola and Adeoye, 2018). The finding that ART self-efficacy was independently associated with self-reported adherence is significant. It indicates that this may be a key indicator to be considered in the readiness assessment of adolescents during the transition to adult care. Older adolescents require sufficient motivation to continue with self-care regardless of external factors/circumstance; hence the importance adherence of self-efficacy.
Prioritisation of the development of interventions that focus on promoting adherence self-efficacy and building self-esteem during the preparation of transition to adult care was recommended. This could potentially provide much needed psychosocial impetus and motivation required at an individual-level to maintain ART adherence into adulthood.
A limitation of this study was that it focused perinatally on infected adolescents in an urban setting. The findings may not be generalisable to adolescents with sexually acquired HIV infection or those in semi-urban and rural settings. Perinatal infection results in a longer duration of ART use (in this study the adolescents had been on ART for almost a decade) and exposure to psychosocial stressors, which makes this population distinct in clinical and psychosocial HIV care. Additionally, a vast majority of adolescents transitioning to adult care-acquired HIV in the perinatal period. Another limitation is that this study used self-reported adherence as an adherence measure which may lead to inaccurate reporting due to recall bias and social desirability. While the viral load is the goal standard of adherence, in many low resource settings, self-adherence is often used as a routine measure during clinic visits. In contrast, viral load measures are assessed periodically (usually twice a year). There was an acceptable level of agreement in this study between the viral suppression cut off and self-reported. However, there are studies including a systematic review (Dachew, et al., 2014) that report self-reported adherence to be an accurate adherence measure (Profile et al., 2001), mainly when short durations as the case in this study (Nieuwkerk and Oort, 2005).
CONCLUSIONS
Assessing and developing interventions focusing on individual-level modifiable factors associated with adherence such as self-efficacy may contribute to adherence self-efficacy and potentially promote a successful transition to adult care for ALWHIV.
ETHICAL CONSIDERATIONS
Written informed consent was obtained to participate and publish from adolescents above 18 years age, and for adolescents aged below 18 years. We obtained both assent and caregiver consent. The University of Nairobi-Kenyatta National Ethical and Research Committee granted ethical approval for this study.
DATA AVAILABILITY
All data generated or analysed during this study are included in this published article and its supplementary information files.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors thank the adolescents at Mbagathi Hospital who participated in this study and leadership and staff at Mbagathi Hospital, in particular, Lilian Abonyo. The UCSF global program team was acknowledged. Support for the data collection only for this project through a research fellowship award from the Fogarty International Centre of the National Institutes of Health (NIH) under Award Number D43TW009343 and the University of California Global Health Institute (UCGHI).
REFERENCES
|
Adejumo OA, Malee KM, Ryscavage P, Hunter SJ, Taiwo BO (2015) Contemporary issues on the epidemiology and antiretroviral adherence of HIV-infected adolescents in sub-Saharan Africa: A narrative review. Journal of the International AIDS Society 18(1): 20049. |
|
|
Aregbesola OH, Adeoye IA (2018). Self-efficacy and antiretroviral therapy adherence among HIV positive pregnant women in South-West Nigeria: a mixed-methods study. Tanzania Journal of Health Research 20(4). |
|
|
Biadgilign S, Deribew A, Amberbir A, Deribe K (2009). Barriers and facilitators to antiretroviral medication adherence among HIV-infected paediatric patients in Ethiopia: A qualitative study [Internet]. Journal of Social Aspects of HIV/AIDS Vol. 6. |
|
|
Caron J (2013). A validation of the Social Provisions Scale: the SPS-10 items. Sante Ment Que 38(1):297-318. |
|
|
Carrizosa J, An I, Appleton R, Camfield P, Von Moers (2014). A Models for transition clinics. Epilepsia 55:46-51. |
|
|
Dachew BA, Tesfahunegn TB, Birhanu AM (2014). Adherence to highly active antiretroviral therapy and associated factors among children at the University of Gondar Hospital and Gondar Poly Clinic, Northwest Ethiopia: a cross-sectional institutional based study. BMC Public Health 14(1):875. |
|
|
Daddis C. Desire for Increased Autonomy and Adolescents' Perceptions of Peer Autonomy: "Everyone Else Can; Why Can't I Child Development 82(4):1310-1326. |
|
|
Damulira C, Mukasa MN, Byansi W, Nabunya P, Kivumbi A, Namatovu P (2019). Examining the relationship of social support and family cohesion on ART adherence among HIV-positive adolescents in southern Uganda: baseline findings. Vulnerable children and youth studies 14(2):181-190. |
|
|
Educación FY, Falanga R, Elvira De Caroli M, Sagone E (2012). relationship between self-efficacy and self-concepts in university students. International Journal of Developmental and Educational Psychology 2(1):227-233. |
|
|
Firdu N, Enquselassie F, Jerene D (2017). HIV-infected adolescents have low adherence to antiretroviral therapy: A cross-sectional study in Addis Ababa, Ethiopia. Pan African Medical Journal 27(1):31. |
|
|
Haberer JE, Cook A, Walker AS, Ngambi M, Ferrier A, Mulenga V (2011). Excellent adherence to antiretrovirals in HIV+ Zambian children is compromised by disrupted routine, HIV Nondisclosure, and Paradoxical Income Effects. PLoS One 6(4):e18505 |
|
|
Johnson MO, Neilands TB, Dilworth SE, Morin SF, Remien RH, Chesney MA (2007). The role of self-efficacy in HIV treatment adherence: validation of the HIV Treatment Adherence Self-Efficacy Scale (HIV-ASES). Journal of behavioral medicine 30(5):359-70. |
|
|
Kurniawan D, Fitrio DRY (2019). Impact of HIV-Related Stigma: Self-Efficacy, Self-Esteem, and Social Isolation on ARV Medication Adherence among Persons Living With HIV in Turen, Malang Pakistan Journal of Medical and Health Sciences. |
|
|
Lamb MR, Fayorsey R, Nuwagaba-Biribonwoha H, Viola V, Mutabazi V, Alwar T, Casalini C, Elul B (2014). High attrition before and after ART initiation among youth (15-24 years of age) enrolled in HIV care. AIDS 28(4):559. |
|
|
MacCarthy S, Saya U, Samba C, Birungi J, Okoboi S, Linnemayr S (2018). "how am i going to live?": Exploring barriers to ART adherence among adolescents and young adults living with HIV in Uganda. BMC Public 18(1):1-11. |
|
|
Mutwa PR, Van Nuil JI, Asiimwe-Kateera B, Kestelyn E, Vyankandondera J, Pool R, Ruhirimbura J, Kanakuze C, Reiss P, Geelen S, van de Wijgert J (2013). Living Situation Affects Adherence to Combination Antiretroviral Therapy in HIV-Infected Adolescents in Rwanda: A Qualitative Study. PLoS One 8(4):e60073. |
|
|
Naar-King S, Templin T, Wright K, Frey M, Parsons JT, Lam P (2006). Psychosocial factors and medication adherence in HIV-positive youth. AIDS Patient Care STDS 20(1):44-7. |
|
|
Nader H (2020) Relationships Between Self-Efficacy, Self-Esteem and Procrastination in Undergraduate Psychology Students. Iranian journal of psychiatry and behavioral sciences 8(3):42. |
|
|
National AIDS & STI (2020). Control M of H. Guidelines on Use of Antiretroviral Drugs for Treating and Preventing HIV Infection in Kenya. |
|
|
Nieuwkerk PT, Oort FJ (2005). Self-Reported Adherence to Antiretroviral Therapy for HIV-1 Infection and Virologic Treatment Response. JAIDS JAIDS Journal of Acquired Immune Deficiency Syndromes 38(4):445-8. |
|
|
Perera HN (2020). Construct Validity of the Social Provisions Scale: A Bifactor Exploratory Structural Equation Modeling Approach. Assessment.23(6):720-33. |
|
|
Profile S, Hays RD, Maldonado T, Liu H, Golin CE, Miller LG, (2001). A Comparison of Multiple Measures of Adherence to HIV Protease Inhibitors A Comparison Study of Multiple Measures of Adherence to HIV Protease Inhibitors Background: Poor adherence to HIV protease inhibitors may]. annals.org. |
|
|
Purwaningsih P, Asmoro CP, Prastiwi YA (2019). Self-esteem and motivation with adherence of people living with HIV/AIDS (PLWHA) in Indonesia with antiretroviral therapy: A cross-sectional study. International Journal of Adolescent Medicine and Health 1. (ahead-of-print). |
|
|
Reda AA, Biadgilign S (2012). Determinants of adherence to antiretroviral therapy among HIV-infected patients in Africa. 2012. |
|
|
Slogrove AL, Mahy M, Armstrong A, Davies MA (2017). Living and dying to be counted: What we know about the epidemiology of the global adolescent HIV epidemic. Journal of the International AIDS Society 20:21520. |
|
|
Tyer-Viola LA, Corless IB, Webel A, Reid P, Sullivan KM, Nichols P (2014). Predictors of Medication Adherence Among HIV-Positive Women in North America. Journal of Obstetric, Gynecologic & Neonatal Nursing 43(2):168-178. |
|
|
UNAIDS (2016). Ending the AIDS epidemic for adolescents, with adolescents; |
|
|
UNAIDS (2016). Nations JU, UN Joint Programme on HIV/AIDS (UNAIDS). Fast-Track Targets [Internet]. 2014. |
|
|
Van Dyke RB, Van Dyke RB, Lee S, Johnson GM, Wiznia A, Mohan K, Stanley K, Morse EV, Krogstad PA, Nachman S (2002). Reported Adherence as a Determinant of Response to Highly Active Antiretroviral Therapy in Children Who Have Human Immunodeficiency Virus Infection. Pediatrics 109(4)e61-e61. |
|
|
World Health Organisation (2006). From Access to Adherence: The Challenges of Antiretroviral Treatment - Studies from Botswana, Tanzania and Uganda, Factors that facilitate or constrain adherence to antiretroviral therapy among adults in Uganda: a pre-intervention study: Chapter 3: [Internet]. 2006 [cited 2020 Mar 26]. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


