Full Length Research Paper

ABSTRACT
There has been improvement in the control of HIV/AIDS in Nigeria. The 2018 national prevalence was 1.4%, a decline from previous surveys. The gains are however not uniform; a gap still exists in the response to key populations (KP) due to socio-cultural barriers and unfavourable legislative environment. The demographic correlates of HIV among KP in Nigeria were examined. Society for Family Health provided HIV Testing services for KP and data from the intervention between 2019 and 2020 was analysed using SPSS version 20. Total of 132,838 were tested, 88.4% were 20-39 years, 65.6% were females and 63.5% were female sex workers (FSW). HIV positive KP were 7,962 (6.0% prevalence), prevalence of HIV was high among those ≥40 years, KP identified as males and men who have sex with men (MSM; p<0.001). Old age (aOR=0.82, 95%CI=0.73 – 0.92), male KP (aOR=1.17, 95%CI=1.11 – 1.22), and MSM (aOR=0.64, 95%CI=0.61 – 0.67) were predictors of HIV positivity. Stakeholders should rethink priorities and strategies in addressing HIV epidemic in the country.
Key words: Key population, HIV testing services, HIV epidemic, female sex workers (FSW), men who have sex with men (MSM), global fund.
INTRODUCTION
Over the years, there has been significant response to the control of HIV/AIDS. Recent global HIV data have brought great optimism that controlling the HIV epidemic could become a reality (Wolf et al., 2018). In 2018, Nigeria, with the support of global community carried out a population-based survey, the Nigeria AIDS Indicator and Impact Survey (NAIIS). Based on findings from the NAIIS, the current national prevalence of HIV is estimated at 1.4% (Federal Ministry of Health, 2019; National Agency for the Control of AIDS [NACA], 2018), reflecting a decline compared to previous surveys (Federal Ministry of Health Nigeria, 2013; Ibiloye et al., 2018). However, despite the control measures being put in place for the control of the HIV/AIDS in the country, a huge gap still exists in the national response to key populations (KPs). This is due to socio-cultural barriers and unfavourable political and legislative environment. KP made up of Female Sex Workers (FSW), Men who have sex with Men (MSM), People who inject Drugs (PWID), Transgender (TG) and People in closed settings such as prisons have been said to be disproportionately affected by HIV (Awofala and Ogundele, 2016; Katbi et al., 2020). The gains in HIV epidemic control have thus not been uniform.
Globally, the proportion of new adult HIV infections globally among key populations and their sexual partners was 62% (UNAIDS, 2020). FSW, MSM and PWID aged 15 years and older were found to be 30, 26 and 29 times, respectively likely to acquire HIV infection when compared with the general population (UNAIDS, 2020). In sub-Saharan Africa, KPs account for about 25% of new HIV infections and in Nigeria, the prevalence among KP group’s ranges from 9.3 to 37.6% (Asuquo et al., 2014). The 2012 National HIV & AIDS and Reproductive Health Survey showed HIV prevalence among MSM to be 22.9%, and 19.4 and 8.6% among brothel-based FSW and non-brothel-based FSW, respectively (Federal Ministry of Health Nigeria, 2013). The prevalence of HIV among MSM in Nigeria has also been shown to be 4 to 10 times higher than the general population (Vu et al., 2013). Lack of proper planning with innovative approaches to reach and cater for KP can therefore make achieving HIV epidemic control an uphill task as they will continue to be a reservoir of new HIV infections. The Joint United Nations Programme on HIV/AIDS came up with an ambitious target of 90-90-90 to be achieved by the year 2020 in her bid to control HIV epidemic, and Nigeria has been part of the countries working towards achieving this target (UNAIDS, 2014). The Fast-Track targets which is to end the AIDS epidemic by 2030, has the next set of goals of 95-95-95 target to be reached by the year 2030. This requires that at least 95% of people living with HIV will know their HIV status, 95% of all people diagnosed with HIV infection will receive sustained antiretroviral therapy, and 95% of all people receiving antiretroviral therapy will have viral suppression. Even though many countries did not meet the year 2020 target, Nigeria inclusive; fast tracking an innovative HIV response which is robust, and data driven can help in achieving the 2030 target in Nigeria. The first 95 is a key entry point in the HIV control response. This study therefore examined the prevalence and demographic correlates of HIV among key population in 10 states in Nigeria. It is believed that findings from the study would inform strategies and overall approach in addressing the HIV epidemic in Nigeria.
METHODOLOGY
Study sites
The Society for Family Health (SFH) through the Global Fund support is one of the Principal Recipients for the HIV intervention grants for KP [Optimizing HIV Investment for Impact (OHII) grant] being implemented from July 2019 to December 2020 across 10 states in Nigeria. The states of intervention were selected based on resource availability and the national key population size estimate, the selected states spread across the different geographical regions of the country include: Abia, Anambra, Edo, Enugu, Imo and Oyo states located in the Southern region of the country, and Gombe, Kaduna, Kano and Taraba states located in the Northern region. SFH provides a comprehensive HIV prevention package including community HIV testing for KPs and linkage of identified KPs to HIV care. Details of the HIV prevention package provided are further explained in the following program intervention.
Program intervention
KP-led Community Based Organizations (CBOs) were used to identify peers in the communities. Staff members of the CBOs who are usually community members were trained as counsellor testers and peer educators.
Comprehensive prevention package
A peer educator designated as community facilitator carried out Interpersonal Communication (IPC) and taught identified KPs about HIV and STI prevention. Commodities to aid prevention such as male and female condoms and lubricants were also given to the KPs. Furthermore, the KPs were offered HIV counselling and testing services. The target was to test all KPs who had not had HIV Testing Services in the last 6 months prior to meeting the person as stipulated in the National Guidelines for HIV Testing Services (National AIDS/STI Control Programme, 2017).
Linkage to treatment
All HIV positive KP members (KPLHIV), newly diagnosed were provided with accompany referral by the CBOs’ case managers to be linked to care and treatment at the most convenient One Stop Shops (OSS) or health facility. OSS were facilities specifically designed for KPs to address their health challenges. The OSS model has been shown to effectively increase the uptake of HIV treatment as well as prevention-treatment linkage in a more conducive settings that protect the privacy of KPs (Onovo et al., 2016). Setting up and the running of the OSS was funded by global fund (GF), thus to enshrine sustainability, public and private health facilities were also trained to be KP friendly. Such facilities and the OSS were therefore termed GF-supported health facilities. However, newly identified KPLHIV may choose to access care in neither an OSS nor KP friendly facility but opt for a different health facility they are comfortable with even though such facility is not supported by GF (Non-GF supported Health facilities). The community case managers and designated case managers in the GF supported facilities (OSS and KP friendly facilities) continued to follow up with the clients afterwards to ensure they are kept in care.
Study design, study period and study population
The study is a retrospective analysis of program data of KP provided with HIV Testing Services (HTS) from July 2019 to June 2020. The KP were MSM, FSW, and PWID aged 15 years and above.
Data collection and analysis
The project aimed to saturate all the implementing states by providing intervention for all accessible and consenting KPs. Data of KPs reached and provided with HIV Testing Services were extracted from the Nigeria District Health Information System (DHIS) platform which was customized by the Society for Family Health for the grant. Statistical Package for Social Sciences version 20 was used to analyse the data set. Description of the sociodemographic characteristics of the KPs were presented as frequencies. The outcome of interest was the HIV status of the KP within the study period, and the extent of the influence of independent variable such as the sociodemographic characteristics of the KP on the outcome variables was analysed using Chi-square test. For variables which were statistically significant after the Chi-square test, such as age, gender and KP typology, they were further categorized into two and binary logistic regression was also carried out to determine the predictors of being HIV positive. P value was considered significant at levels equal to or less than 0.05 for all inferential analysis.
Ethical consideration
The National Agency for the Control of AIDS (NACA) approved the program implementation. As part of the program implementation criteria, all field staff were trained on the issue of confidentiality while providing services for clients. All services provided were voluntary and counselling ethics according to the National guideline on HIV Testing Services (National AIDS/STI Control Programme, 2017)were followed as clients gave informed consent before being provided with services. The researchers did not have access to the records of clients, they had access to only de-identified data. Unique codes referred to as enrolment ID were used to identify clients. All HIV positive clients were linked to either KP-friendly health facilities or OSS for commencement of Anti-Retroviral Therapy (ART) and other care as appropriate.
RESULTS
During the period under review (July 2019 to June 2020), a total of 132, 838 KPs were provided with HIV Testing Services across the ten implementation states. Majority of them [117,395 (88.4%)] were in the age group 20 to 39 years. Eighty-seven thousand, 158 (65.6%) were females, and 84,317 (63.5%) were Female Sex Workers. The state with most numbers of KPs was Kaduna State, it accounted for 20.8% (n= 27,656) of the population (Table 1).
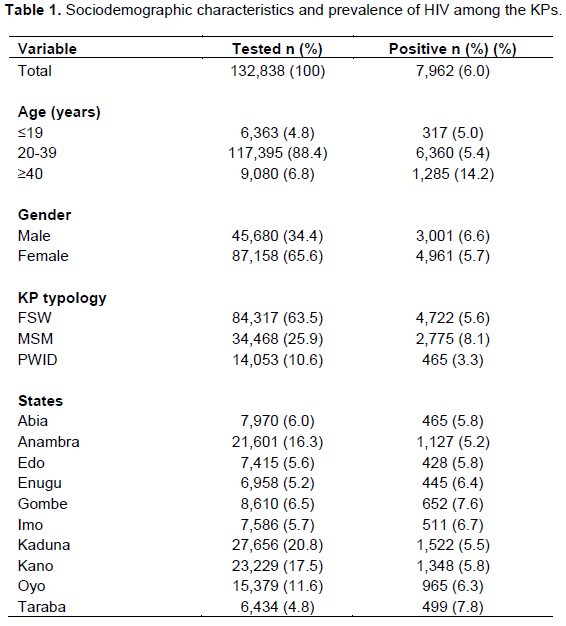
Out of the numbers tested, those that tested HIV positive were 7,962 given a HIV prevalence of 6.0%. The prevalence of HIV was high among those who were ≥ 40 years of age [1,285/9,080 (14.2%)], MSM [2,775/34,468 (8.1%)], and KPs that were resident in Taraba State [499/5,935 (7.8%)]. HIV prevalence was also found to be higher among males [3,001/45,680 (6.6%)] compared to the females [4,961/87,158 (5.7%)] (Table 1).
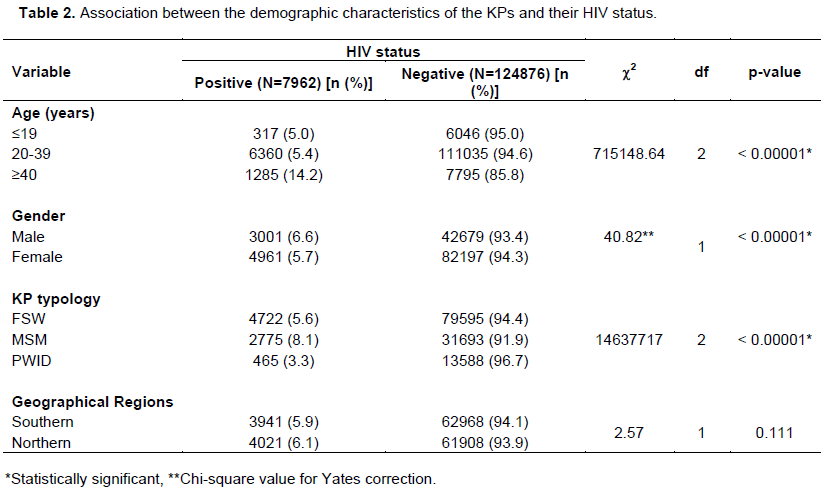
Table 2 shows the associations between the demographic characteristics of the KPs with their HIV status. The prevalence of HIV was significantly higher among KPs greater than or equal to 40 years of age (14.2%) compared to other age groups (c2 = 715148.64, p<0.001). The difference between the prevalence of HIV among the male (6.6%) and female (5.7%) KPs was also found to be statistically significantly (c2 = 40.97, p<0.001). More proportions of MSM (8.1%) were significantly found to be HIV positive compared to other KP typology (c2 = 14637717, p<0.001), however there was no statistically significant difference in the HIV prevalence among KPs across the Southern and Northern geographical zones (c2 = 2.57, p=0.111).
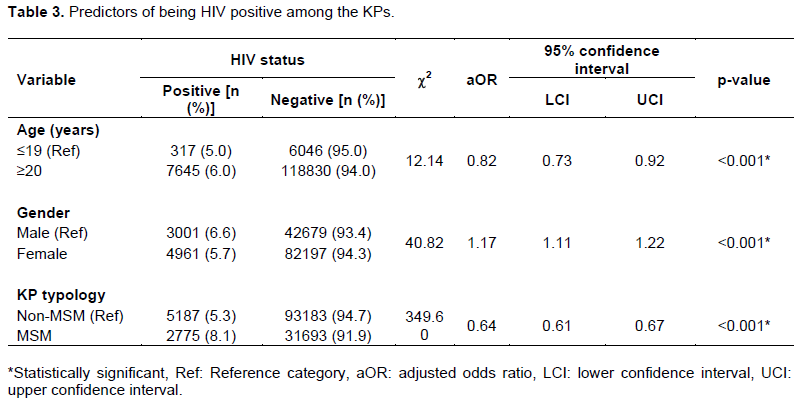
Further analysis in Table 3 using logistic regression showed the predictors of being HIV positive among KPs. KPs who are 20 years of age and above were 1.2 (1/0.82) times likely to be HIV positive compared to the lower age groups (aOR=0.82, 95%CI=0.73 – 0.92, p<0.001). In the same vein, the male KPs were 1.2 times more likely to be HIV positive compared to the female KPs (aOR=1.17, 95%CI=1.11 – 1.22, p<0.001), while the odds of being HIV positive among KPs that are non-MSM is lower compared to KPs that are MSM (aOR=0.64, 95%CI=0.61 – 0.67, p<0.001).
DISCUSSION
The HIV prevalence among the KPs in this study was 6.0%, a value much higher than the national HIV prevalence of 1.5% in Nigeria (Federal Ministry of Health, 2019). This value is also higher than that of the geopolitical zone with the highest prevalence in the country.(Federal Ministry of Health, 2019)It is therefore important that if HIV epidemic control would be truly attained in Nigeria, attention should be given to KPs as much as it is given to the general population. Several studies have also shown that KPs despite constituting a smaller proportion of the population in the country, they are responsible for a larger proportion of HIV infection (Afe et al., 2019; Okafor et al., 2017; Vu et al., 2013). Taraba State has the highest prevalence of HIV in the Northeastern part of Nigeria (National Agency for the Control of AIDS [NACA], 2018), and this study showed the state to have the highest numbers of KPs to be living with HIV in spite of the KP size lesser than other states. Further study may be conducted to see if there is a link between the HIV prevalence of KP and the general HIV prevalence in the state.
Among the KPs provided with HTS, about 8 out of 10 MSMs were found to be HIV positive; about half of FSWs and a third of the PWID were found to be HIV positive. This HIV seropositivity rates are similar to the ones obtained in a study carried out in Lagos State by Afe et al (2019). However, in another study conducted among MSM in Abuja, Lagos and Ibadan, the population-based estimates of HIV prevalence among MSM in the three cities were 35, 15.2, and 11.3%, respectively (Vu et al., 2013). This difference may be because the study with the higher prevalence was carried out only within the cities while our study focused on all the local government areas across all the 10 states of implementation, be it rural or urban. The high prevalence among MSM in these cities could indicate concentration of more MSM with high-risk sexual behaviours in urban dwellings where there may be better prospects of meeting other individuals with similar sexual orientation. This study further shows being MSM as a predictor of being HIV positive. While high HIV prevalence has been reported among KPs generally (Afe et al., 2019; National Agency for the Control of AIDS [NACA], 2018; Njab et al., 2018; Ochonye et al., 2019), a higher prevalence has been reported among the MSM sub-KP globally (Beyrer et al., 2012; Jansen et al., 2011; Morris and Little, 2011), and Nigeria is no exception (Afe et al., 2019; Eluwa et al., 2019; Vu et al., 2013). Interestingly, stigma, discrimination, homophobia and criminalization that these MSMs face has made them reluctant to access health care services (Allman et al., 2007; Vu et al., 2013). MSMs in Nigeria have been reported to live double lives of publicly engaging in heterosexual relationships and same-sex relationship secretly (Allman et al., 2007), many of them have also self-identified as bisexual (Vu et al., 2013)and will continue to serve as reservoir of HIV infection in the population without access to proper HIV prevention, treatment and care programs devoid of stigmatization, and policies that are non-restrictive.
Furthermore, about three out of five of the KPs in the older age group greater than or equals to twenty years of age were found to be HIV positive with older age group being a predictor of being HIV positive. Similar finding was also observed in a study that looked at the trends of HIV prevalence among MSM in the three rounds of integrated biological and behavioral surveillance survey (IBBS) of 2007, 2010 and 2014 (Eluwa et al., 2019)where older age was found to be one of the factors associated with HIV.
While the national prevalence of HIV among females between 15 and 64 years of age is higher than what obtains among the males, the findings among the KPs in this study showed a contrary finding, with the prevalence of HIV found to be higher among the males than the females. About 7 out of 10 females were found to be HIV positive, while about 6 out of 10 females were HIV positive in this survey. The reason for the males being the drivers of HIV epidemic among the KPs in this study is however not far-fetched. The reason is because the MSMs whose gender class are males have the highest HIV prevalence.
Another interesting finding in this study is the non-difference of HIV prevalence among the Northern and Southern geographical zones. While there is significant variation in the national HIV prevalence across the different geographical zones in Nigeria, this is not the case for the KPs, another pointer to show that there has been no significant difference in the intervention programs of HIV prevention, treatment, and care for KPs across all the zones in the country.
STUDY LIMITATIONS
The data from this study was from a HIV intervention program for KPs. Thus, analysis was based on the data available from the program. The study therefore did not consider other factors that may be predictors of acquiring HIV infection, such as use of alcohol, infection with other sexually transmitted diseases and perceived risk of contracting HIV among respondents.
CONCLUSIONS
This study has shown that KPs constitute a major reservoir of HIV infection in Nigeria with the MSM having the highest numbers of HIV prevalence. The odds of being HIV positive was found to be lesser among the non-MSM compared to the MSM. It also showed that HIV prevalence among the KPs across the different zones does not differ from each other. Without concerted efforts of the government at all levels, relevant stakeholders, and civil society organizations to provide holistic HIV prevention programs for KPs, the gains of HIV epidemic control recorded so far may be eroded. The high HIV prevalence among KPs is obviously a defining challenge which should spur the government to rethink her priorities and strategies in addressing HIV epidemic.
ACKNOWLEDGEMENT
The authors thank the KP-led community-based organizations that helped in providing HIV prevention packages for the key population
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Afe AJ, Onyema M, Ojoye AO, Iwuoha E (2019). Analysis of HIV Treatment Cascade Among Key Affected Population in Lagos, Nigeria. European Journal of Medical and Health Sciences 1(3):1-6. |
|
|
Allman D, Adebajo S, Myers T, Odumuye O, Ogunsola F (2007). Challenges for the sexual health and social acceptance of men who have sex with men in Nigeria. Cult Health Sex 9(2):153-168. |
|
|
Asuquo G, Owolabi D, Onoja A, Okoro U, Durueke F (2014). Community needs assessment of key populations-at-risk of HIV/AIDS in Nigeria's capital territory. BMC Infectious Diseases, 14(Suppl2), P29. |
|
|
Awofala AA, Ogundele OE (2016). HIV epidemiology in Nigeria. Saudi Journal of Biological Sciences 25(4):697-703 |
|
|
Beyrer C, Baral S, van Griensven F, Goodreau S, Chariyalertsak S, Wirtz A, Brookmeyer R (2012). Global epidemiology of HIV infection in men who have sex with men. Lancet, 380(9839)367-377. |
|
|
Eluwa G, Adebajo SB, Eluwa T, Ogbanufe O, Ilesanmi O, Nzelu C (2019). Rising HIV prevalence among men who have sex with men in Nigeria: a trend analysis. BMC Public Health 19(1):1-10. |
|
|
Federal Ministry of Health (2019). Nigeria HIV/AIDS Indicator and Impact Survey (NAIIS) - Fact Sheet. National Summary Fact Sheet, March, 1-5. |
|
|
Federal Ministry of Health Nigeria (2013). National HIV & AIDS and Reproductive Health Survey (NARHS Plus II, 2012. |
|
|
Ibiloye O, Decroo T, Eyona N, Eze P, Agada P (2018). Characteristics and early clinical outcomes of key populations attending comprehensive community-based HIV care: Experiences from Nasarawa State, Nigeria. PLoS One 13(12):1-13. |
|
|
Jansen I, Geskus R, Davidovich U, Jurriaans S, Coutinho R, Prins M, Stolte I (2011). Ongoing HIV-1 transmission among men who have sex with men in Amsterdam: a 25-year prospective cohort study. AIDS 25(4);493-501. |
|
|
Katbi M, Adedoyin AO, Bello M, Adegboye A, Adeoye O, Kalaiwo A, Klindera K, Faturiyele I, Alamu T, Swomen H, Russell M, Abubakar, A (2020). Virologic Response among Key Populations Living With HIV following a Switch to Dolutegravir-Based Regimen in Southern Nigeria. International Journal of Virology and AIDS, 7:069. |
|
|
Morris S, Little S (2011). MSM: resurgent epidemics. Curr Opin HIV AIDS, 6(4):326-332. |
|
|
National Agency for the Control of AIDS [NACA] (2018). REVISED NATIONAL HIV AND AIDS STRATEGIC FRAMEWORK 2019-2021. |
|
|
National AIDS/STI Control Programme (2017). National Guidelines for HIV Testing Services. |
|
|
Njab J, Adebajo S, Eluwa G, Shoyemi E, Osakwe P, Eke C, Offie D (2018). HIV Treatment Cascade Assessment of a Community-Based Test and Start Model for Key Populations in Lagos State Nigeria: Where Are the Gaps? World Journal of AIDS 8(3):105-117. |
|
|
Ochonye B, Folayan MO, Fatusi AO, Bello BM, Ajidagba B, Emmanuel G, Umoh P, Yusuf A, Jaiyebo T (2019). Sexual practices, sexual behavior and HIV risk profile of key populations in Nigeria. BMC Public Health 19(1):1210. |
|
|
Okafor UO, Crutzen R, Ifeanyi O, Adebajo S, Borne H (2017). HIV prevalence and high?risk behaviour of young brothel and non?brothel based female sex workers in Nigeria. BMC Research Notes 10(1):380. |
|
|
Onovo A, Kalaiwo A, Okechukwu E (2016). One-Stop Shop: A Community-Based Antiretroviral Therapy (ART) Clinic Model to Improve Human Immunodeficiency Virus (HIV) Prevention and Treatment Cascade for Key Populations in Nigeria. Open Forum Infectious Diseases, 3(suppl_1). |
|
|
UNAIDS (2014). 90-90-90 An ambitious treatment target to help end the AIDS epidemic. |
|
|
UNAIDS (2020). New HIV infections increasingly among key populations. |
|
|
Vu L, Adebajo S, Tun W, Sheehy M, Karlyn A, Njab J, Azeez A, Ahonsi B (2013). High HIV Prevalence Among Men Who Have Sex With Men in Nigeria: Implications for Combination Prevention. Journal of Acquired Immune Deficiency Syndrome 63(2):221-227. |
|
|
Wolf RC, Bingham T, Millett G, Wilcher R (2018). Building the evidence base to optimize the impact of key population programming across the HIV cascade. Journal of the International AIDS Society, 21(S5), e25146. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


