Full Length Research Paper

ABSTRACT
Viral suppression assesses the success of HIV/AIDS treatment and can avert or reduce transmission of infection. Several factors contribute to viral suppression and may vary in different settings and age groups, hence the need to study the associated factors in different populations. The aim of the research was to study the level of viral suppression and its predictors among adolescents living with HIV (ALHIV), who knew their status, at the paediatric infectious diseases unit of a tertiary hospital in Nigeria. This was a descriptive cross-sectional study of 50 consecutive ALHIV who had full disclosure of their HIV diagnosis. There were 29 females with a female to male ratio of 1.38:1. Age range was 10 to 19 years. Mean age was 15.06 ± 2.26 years. A pretested questionnaire was used together with information retrieved from case notes. Socio-demographic data and responses to possible factors affecting viral suppression were obtained and recorded in a proforma. Viral load ranged from <40 to 522,244 HIV RNA copies/ml of blood. Viral suppression rate was 82.00 with 22.00% in those aged 10 to 14 years and 60.00% in those between 15 and 19 years. Factors significantly associated with viral suppression were: Parents being alive (p=0.035), caregivers being on routine medications (p=0.003), missing medications (p=0.0001), number of missed doses of antiretroviral medications (p=0.001), and the current regimen of antiretroviral therapy (p=0.034). In conclusion, viral suppression is approaching UNAIDS target for 2020 and factors related to good adherence to antiretroviral regimens were significant associations.
Key words: Viral suppression, disclosed adolescents, HIV, antiretroviral therapy.
INTRODUCTION
There are many potential benefits to maintaining undetected or in the least, low viral load in people living with HIV (PLHIV). Those with undetected viral load, which is the ultimate goal of treatment, are generally more likely to be healthier than those with high viral load and are less likely to transmit the infection to their sexual partners (and in the case of females to their babies). Viral suppression which results from good adherence to combined antiretroviral therapy (cART) is a principle that drives the prevention of transmission of human immunodeficiency virus (HIV). ALHIV constitute about 5% of all HIV global infections and those between 15 and 19 years account for 16% of new adult global infections (UNAIDS, 2018). Sub-Saharan Africa and south Asia account for the highest number of ALHIV with about 1.6 million cases (89%) of global adolescent infections (Global HIV and AIDS Statistics, 2019; UNAIDS, 2017).
Nigeria, the second largest HIV prevalence after South Africa, with only 26% of infected children receiving cART as at 2017 and only 24% viral suppression in 2016 (Global HIV and AIDS statistics, 2019; UNAIDS, 2017). Ekweme et al. (2018) reported viral suppression rates of 69.1 and 64.8% among 10-14 and 15-19 years old ALHIV respectively (P<0.001), in a study involving 10 states in Nigeria. World Bank (2017) reported that Nigeria has the largest population of youths in the world. It is also the only country with rising mortality of HIV infected adolescents between the ages of 10 and 14 years (NBS and UNICEF, 2017).
After the introduction of highly active antiretroviral therapy (HAART), potential barriers to optimal adherence must be eliminated or at worst reduced to maximise the likelihood of achieving sustained viral suppression (Zanoni, 2019). Irrespective of disease duration and mode of transmission, efforts need be made towards retaining adolescents in care to improve and maintain their health for the long term.
Adolescent HIV/AIDS is regarded as a separate epidemic in terms of the distinctive requirements for managing them as it differs from the adult counterpart (Naswa et al., 2010). One of the issues in managing adolescent HIV cases is the disclosure of their sero-status, which has been reported to improve adherence (Montalto et al., 2017; Phiri et al., 2015; Mburu et al., 2014; Midtbø et al., 2012). Viral suppression, which is achievable through the provisions of HAART by donor agencies, because the government is yet to take over the programme, need to be studied in different localities to know the gaps that must be filled towards achieving the ambitious target of ending the global HIV/AIDS epidemic in 2030. There is paucity of data on viral suppression among Nigerian adolescents living with HIV, especially those who are aware of their HIV diagnosis. Many adolescents started treatment in infancy and their care-givers still do not accept disclosure, opting for disclosure when they are older than 15 years. Newly enrolled adolescents have disclosure done before introduction of HAART. Available data (Ekweme et al., 2018) shows that adolescent viral suppression rates are still lower than the Sustainable Development Goals of vision 90-90-90 by 2020: UNAIDS, 2017) which demands that 90% of those on treatment should achieve viral suppression. This has to be achieved before moving to the latest target of 95-95-95 (Avert, 2019)
This study seeks to document the viral suppression rates of disclosed ALHVI at the University Teaching Hospital, Uyo and to find out any factors that may be associated with the viral suppression in our environment.
METHODS
This cross-sectional study was done at the Paediatrics’ Infectious Diseases Unit of University of Uyo Teaching Hospital, Uyo, Nigeria. The unit caters for 206 paediatric HIV patients of which 140 are adolescents aged between 10 and 19 years. All eligible and consenting subjects were recruited consecutively. Inclusion criteria were: Adolescents who have had full disclosure of their HIV diagnosis for about 6 months and have been on HAART for same duration or longer, have had at least one viral load result, and whose parent(s) or legal guardians gave informed consent and themselves assented to participate. Fifty adolescents met these criteria and were recruited consecutively into the study. A pretested semi-structured self-administered questionnaire was used to obtain the biodata, information on schooling, parentage, clinic appointment visits, adherence to HAART, treatment partner, observation and monitoring of medications, any missed doses and reasons, whether or not the caregivers were on routine medications. The treatment regimens, duration on HAART, viral load results, confirmation on keeping clinic appointments were obtained from the case notes.
The social class of each participant was determined using Oyedeji’s social class scoring system (Oyedeji, 1985) which uses the educational level and occupation of parents/caregivers of the adolescent. The educational level is scored on a scale of five, with 1 being the most educated, degree holders and equivalent and 5 being those without formal education or those who can just read and write. Occupation is also on a scale of five with category 1 being senior civil servants, chief executive officer and contractors, while 5 consist of the unemployed, full time house-wives or students. The sum of the educational and occupation scores of each parent is divided by 4 and the answer to the nearest whole number represents the social class which is also from 1 to 5. Social class 1 is the highest.
Viral suppression was taken as less than 1000 RNA copies/ml of blood based on the World Health Organisation (WHO) consolidated guidelines (WHO, 2015) and those who were stable on HAART as having less than 40 copies/ml of blood. Viral load of 1,000 copies/ml of blood or more constituted the virally unsuppressed group.
Data obtained were inputted and analysed using the Statistical Package for Social Sciences (SPSS), version 25. Simple frequencies were obtained and proportions compared using Chi-Square test with significance established at P<0.005.
RESULTS
Fifty-eight of the 206 paediatric clients on follow-up care for HIV/AIDS in the unit have had full disclosure of their HIV diagnosis. There are a total of 140 clients aged 10-19 years but 82 are yet to have full disclosure as many parents/caregivers still insist that disclosure should not be made to perinatally infected children who are now adolescents till after 15 years of age, and their opinion has to be respected while educating them on the need for disclosure and its benefits. Fifty out of 58 disclosed adolescents participated in the study for having at least one viral load test result on record. Forty-one (82%) of the 50 participants had achieved viral suppression based on the WHO recommendation of less than 1,000 HIV RNA copies/ml of blood (WHO, 2015). Viral suppression rates were 11(22%) for 10 to 14 years and 30(60%) for 15 to 19 years age bracket respectively, p=0.254 (Fisher’s Exact Test). There were 29 (58.00%) females and the female to male ratio was 1.38:1. Mean age was 15.06 ± 2.26 years while the median was 15.00 years. The mean duration on HAART was 9.10 ± 4.03 years with the minimum being 7 months and the maximum 16.00 years. The viral load ranged from <20 to 522,244 HIV RNA copies/ml of blood.
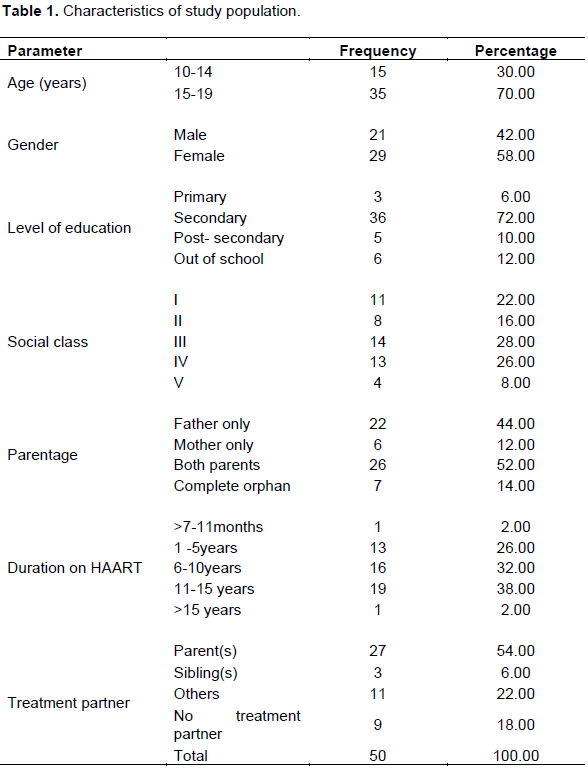
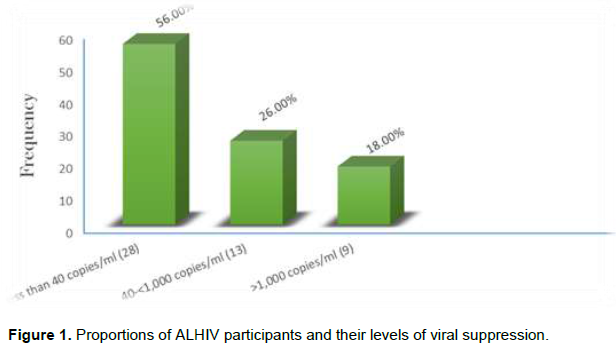
Table 1 shows the characteristics of the study population: There were 29(58.00%) females and 21(42.00%) males, 36(72.00%) of the participants were in secondary school, the largest social class was class III with 14 (28.00%) participants, 36 (52.00%) of the adolescents had both parents alive but 7(14.00%) were complete orphans. Nineteen (38.00%) of the participants had been on HAART for 11 to 15 years and only 1 (2.00%) had antiretroviral therapy for less than a year. Parents were treatment partners for 27 (54.00%) of the respondents but 9 (18.00%) had no treatment partner. Figure 1 shows that 28(56.00%) of the participants had achieved viral suppression at the level of <40 HIV RNA copies/ml of blood and another 13(26.00%) at 40 to <1000 HIV RNA copies/ml of blood. However 9(18.00%) were yet to achieve viral suppression. The figure shows the proportion of viral suppression: 28 (56%) respondents had <40 HIV RNA copies/ml of blood, and 13 (26%) had 40≤1,000 HIV RNA copies/ml of blood but 9 (18%) had over 1,000 HIV RNA copies/ml of blood.
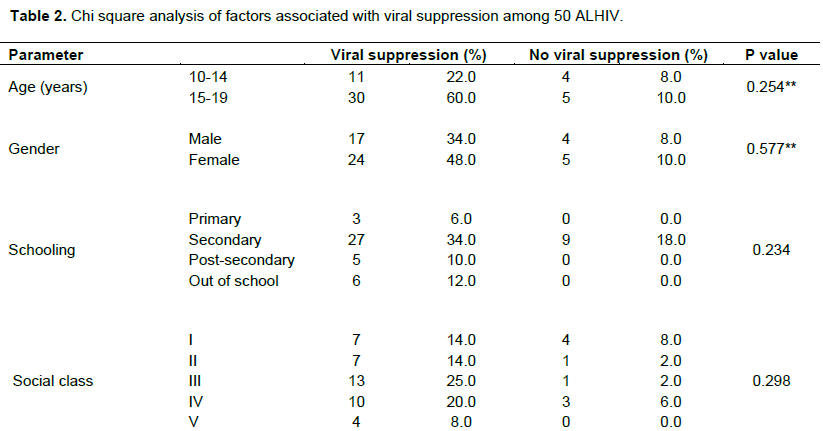
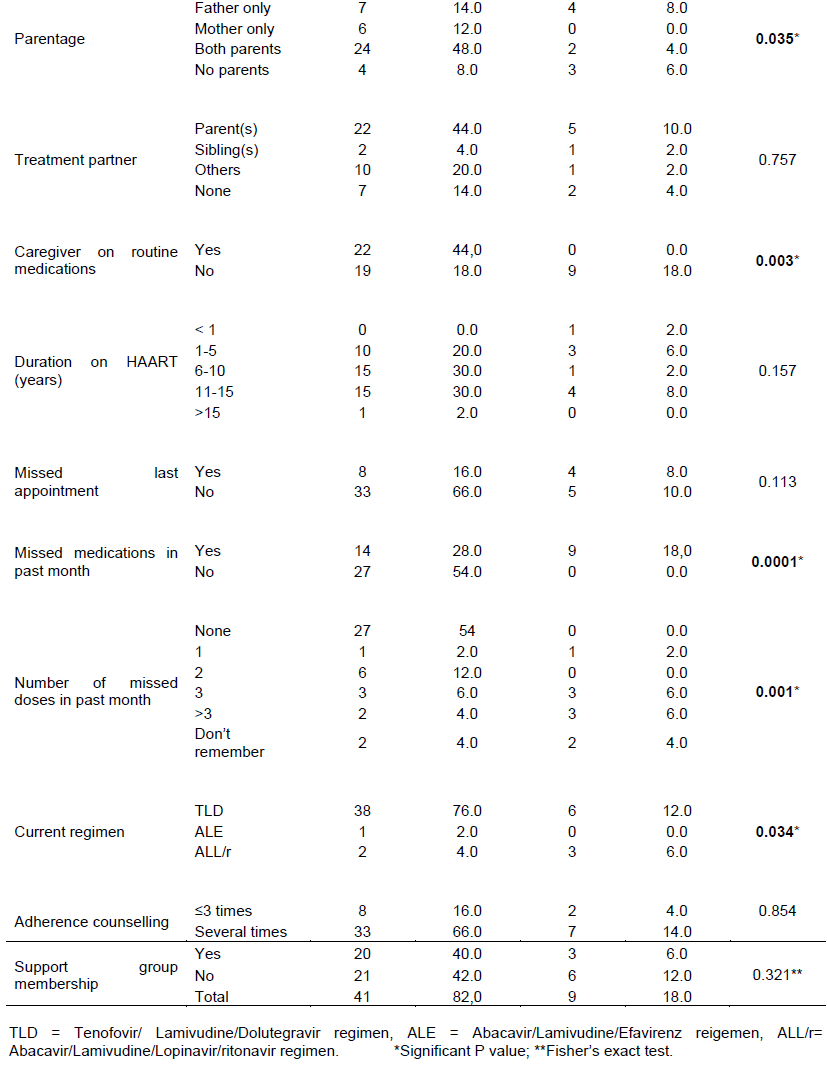
From Table 2, the Chi square test analysis of factors associated with viral suppression in 50 ALHIV shows that viral suppression was significantly associated with parentage, p=0.035, as adolescents with both parents alive were more likely to achieve viral suppression; caregivers being on routine medications was also a positive factor (p=0.003), not missing medications in the past month (p=0.0001), and no missed doses of medications in the past month (p=0.001). Also the adolescents who were currently taking the fixed dose medication of Tenofovir, Lamivudine and Abacavir regimen of medications were more likely to achieve viral suppression (p=0.034). There was no significant association with the age (p=0.254), gender (0.577), level of education (p=0.234) and social class (p=0.298) of the respondents. Having a treatment partner, the duration on HAART, missing clinic appointment, and the number of adherence counselling received were also of no statistical significance (p=0.757, p=0.157, p=0.113 and p=0.854, respectively). Membership of the adolescent support group was also not a statistically significant factor (p=0.321).
DISCUSSION
The viral suppression rate of 82% which is below the UNAIDS 2020 Fast Track Targets (UNAIDS, 2017) but higher than 69.1 and 64.8% reported by Ekweme et al (2018) in adolescents aged 10-14 years and 15-19 years respectively in 10 ten states in Nigeria with a large sample size of 8498 children and adolescents. The suppression rate of 22% in adolescents aged 10-14 years is however very low compared to 69.1% of the previous study (Ekweme et al., 2018) though the sample size is remarkably lower. The relatively lower suppression rate in younger adolescents may not be unconnected with their level of understanding of the importance and benefits of good adherence towards the achievement of viral suppression. Adolescents who have not achieved viral suppression are receiving intensive adherence counselling for further viral load monitoring. A comparative study of adolescents and young adults in South Africa reported a similar viral suppression of 80% from the standard paediatrics clinic and 91% from adolescent friendly clinic (p=0.028) and the participants in that study were relatively older, between 13 and 24 years (Zanoni, 2019).
Adolescent viral suppression is relatively lower than that of adults in many communities. For instance, Kapogrannis et al. (2020) reported 35% viral suppression in adolescents and young adults aged 12 to 24 years though it was within a short duration of 5 months.
There were slightly more females than males (female: male ratio=1.38:1) in the study population but the reason for this is not clear since majority of the adolescents have been on treatment for over 10 years suggesting that they had vertical transmission. However some female might have had sexual transmission as was reported by Ikpeme et al. (2016) from the same centre where some females were told their diagnosis as part of their being managed as cases of sexual transmission.
The mean duration on HAART of 9.00 ± 4.03 years is comparable to 7±3.7 years reported from a Brazilian multicentre study of children and ALHIV (Cruz et al., 2014). This is likely because many adolescents started treatment at an early age from early detection as vertically infected children. Majority of the respondents were in secondary schools and this is understandable considering their age range.
About 56.00% viral suppression was at the level of <40 HIV RNA copies/ml of viral suppression which is close to the desirable undetected viral suppression that is needed for non-transmission of HIV infection in any population. This is slightly higher than 49% reported among ALHIV in Brazil which is a resource-rich country and their viral load was <50 HIV RNA copies/ml. This shows a comparable stance as the striving towards the UNAIDS ambitious target of ending the global HIV/AIDS epidemic in 2030 (Avert, 2019).
Parents being alive were a significant association with viral suppression, and this could be due to positive parental support. Knodel et al. (2010) reported that family members, including parents, commonly remind patients to take their antiretroviral medications, especially if co-resident, also those parents often reminded the patients to get resupplies and sometimes accompanied them to the clinic for appointments. Also parents/caregivers being on routine medications was significantly associated with viral suppression (p=0.003). While there are no previous findings to compare with, it may be inferred that parents/caregivers on routine medications may encourage their children/wards to achieve good adherence leading to viral suppression. Not missing medications expectedly had a significant association with viral suppression (p=0.0001). Additionally, in terms of number of missed doses, those who self-reported missing three or more doses per month were significantly less likely to achieve viral suppression (p=0.001) (Table 2). Trials have traditionally considered adherence thresholds of greater than 95% as optimal (Paterson et al., 2000). With a once daily regimen, it takes missing as low as two doses to fall short of this optimal adherence.
The regimen of fixed dose combination of Tenofovir/Lamivudine/Dolutegravir was significantly associated with viral suppression compared to those on Abacavir/Lamivudine/Efavirenz or Lopinovir. This could be due to the bulk of the study population are currently on this regimen. There was no significant association between viral suppression and clinic attendance (Table 2) even though ALHIV who missed clinic appointments were less likely to be virally suppressed. The small sample size might have affected this finding. This also contrasts with the findings of Lokpo et al. (2020) where regular clinic attendance was significantly associated with viral suppression (p=0.0001). This could be due to the practice of giving a week’s medication in excess of appointment which makes clients miss appointment dates when they have medications at home. Several other parameters were also not significantly associated with viral suppression including: clients’ age and gender, level of education, social class, having a treatment partner, duration of antiretroviral therapy, number of adherence counselling sessions received or membership of the adolescent support group.
CONCLUSION
Viral suppression among disclosed adolescents is close to the UNAIDS target for 2020 and factors related to good adherence to Tenofovir/Lamivudine/Dolutegravir regimen are significantly associated with viral suppression of ALHIV in our locale.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
AVERT (2019), Global HIV Targets, AVERT, Brighton, UK, 2019. |
|
|
Cruz MLS, Cardoso CAA, Darmont MQ, Souza E, Andrade SD, D'Al Fabbro MM, Fonseca R, Bellido JG, Monteiro SS, Bastos FI (2014). Viral suppression and adherence among HIV-infected children and adolescents on antiretroviral therapy: Results of a multicentre study. Journal de Pediatria (Rio J) 90(6):563-571. |
|
|
Ekweme C, Torbonde N, Anaba UC, Makplang M, Ekong E, Sam-Agudu NA (2018). The Third 90: Viral Suppression among HIV- Positive Children and Adolescents in 10 Nigerian States. 2018. |
|
|
Global HIV & AIDS statistics (2019). fact sheet. |
|
|
Ikpeme E, Dixon-Umo OT (2016). Disclosure of HIV diagnosis to infected children receiving care in University of Uyo Teaching Hospital, Uyo, Nigeria. Journal of AIDS and HIV Research 8(7):93-99. |
|
|
Kapogrannis BG, Koenig LJ, Xu J, Mayer KH, Mayer, KH, Loeb J, Greenberg L, Monte D, Banks-Shields M, Fortenberry JD, Adolescent Medicine Trials Network for HIV/AIDS Interventions (2020). The HIV continuum of care for adolescents and young adults attending 13 urban US HIV Care centers of the NICHD-ATN-CDC-HRSA SMILE Collaborative. Journal of Acquired Immune Deficiency Syndrome 84(1):92-100. |
|
|
Knodel J, Kespichayattana J, Saengtienchai C, Wiwatwanich S (2010). The role of parents and family in ART treatment adherence: Evidence from Thailand. Research on Ageing 32(1):19-39. |
|
|
Lokpo SY, Ofori-Attah P Jnr, Ameke LS, Obirikorang C, Orish VN, Kpene GE, Agboli E, Kye-Duodu G, Deku JG, Awadzi BK, Noagbe M, Quarshie ST (2020). Viral suppression and Its Associated Factors in HIV Patients on Highly Active Antiretroviral Therapy (HAART): A Retrospective Study in Ho Municipality, Ghana. Hindawi AIDS Research and Treatment Volume 2020, Article ID 9247451, 7 pages. |
|
|
Mburu G, Hodgson I, Kalibala S, Haamujompa C, Cataldo F, Lowenthal ED, Ross DA (2014). Adolescent HIV disclosure in Zambia: Barriers, facilitators and outcomes. Journal of the International AIDS Society 17(1):18866. |
|
|
Midtbø V, Shirima V, Skovdal M, Marguerite D (2012). How disclosure and antiretroviral therapy help HIV infected adolescents in sub- Saharan Africa cope with stigma. African Journal of Aids Research. 11(3):261-271. |
|
|
Montalto GJ, Sawe FK, Miruka A, Maswai J, Kiptoo J, Aoko A, Oreyo C, Obiero E, Korir S, Bii SK, Song KX, Kunz AN (2017). Diagnosis disclosure to adolescents living with HIV in rural Kenya improves antiretroviral adherence and immunologic outcomes: A retrospective cohort study. PLoS ONE 12(10):e0183180.]. |
|
|
Naswa S, Marfatia YS. Adolescent HIV/AIDS: Issues and Challenges (2010). Indian Journal of Sexually Transmitted Diseases and AIDS 31(1):1-10. |
|
|
National Bureau of statistics (NBS) and United Nation's Children Fund (UNICEF) (2017). Multiple Indicator Cluster Survey 2016-2017. Survey Findings Report. |
|
|
Oyedeji GA (1985). Socio-economic and cultural background of hospitalized children in Ilesha. Nigerian Journal of Paediatrics 12:111-117. |
|
|
Paterson DL, Swindells S, Mohr J, Brester M, Vergis EN, Squier CL, Wagener MM, Singh N (2000). Adherence to Protease Inhibitor Therapy Outcome in Patients with HIV Infection. Annals of Internal Medicine 133(1):21-30. |
|
|
Phiri C, Chilemba E (2015). Benefits and Risks of Disclosing Human Immunodeficiency Virus Diagnosis to Perinatally Infected Children: A Critical Review of the Literature. Journal of Nursing Care 4(260):2167-1168. |
|
|
UNAIDS (2017). Ending AIDS Progress Towards the 90-90-90 targets. Geneva. Switzerland: UNAIDS; 2017.UNAIDS/JC2900E. |
|
|
UNAIDS data (2018). |
|
|
WHO (2015). Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection in Clinical Guidelines: Antiretroviral Therapy, WHO, Geneva. Switzerland. 2015. |
|
|
World Bank (2017). Nigeria at a glance. The World Bank in Nigeria. |
|
|
Zanoni BC, Sibaya T, Cairns C, Haberer JE (2019). Barriers to retention in care are overcome by adolescent-friendly services for adolescents living with HIV in South Africa: A qualitative analysis. AIDS and Behaviour 23(4):957-965. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


