Full Length Research Paper
ABSTRACT
This study investigated the economic effects of malaria on cocoa farmers in Ondo State, Nigeria using the ordinary least square regression technique. Descriptive statistics were used to identify strategies to reduce malaria infection among cocoa farmers. The sample frame for the study was derived from secondary data obtained from records of Ondo State Ministry of Health on registered cocoa farmers who had malaria during the production season in 2015. Multi-stage, systematic and purposive samplings were used to select 180 respondents for the study. Some of the variables measured include: annual income of farmers, direct cost of malaria treatment, number of days of incapacitation and additional labour cost incurred by the farmers during periods of incapacitation. Results from the study showed that the mean annual income estimate was ₦524,096. It was revealed that the cost of malaria treatment and additional labour cost incurred had a significant effect on the income of the farmers, however; the number of days of incapacitation had no significant effect on the income of cocoa farmers.
Key words: Malaria, income, ordinary least squares regression and cocoa.
INTRODUCTION
Economic growth and development are achievable in any nation with a viable agricultural sector. Most developed nations of the world are characterized by technology-driven farm production activities. This has enhanced self-sufficiency in feeding their populace. In developing countries, on the other hand, farm production activities depend largely on people in the rural areas using manual labour. Owing to the physical nature of farming activities, the health of farmers could be adversely affected by diseases including malaria if they have little or no medical attention. Medical issues have been observed to impact negatively on agricultural productivity in Nigeria and malaria has been a major contributor to ill health in Africa (Breman et al., 2006). According to Kwadwo et al. (2009), human activities, including agriculture has been recognized as one of the reasons for increased intensity of malaria around the world, because it supports the breeding of mosquitoes that carries the parasite. Mohammed et al. (2018) posited that a greater percentage of small-scale farmers in Nigeria leave (sic) in the rural areas. A typical rural village in the country is characterized with an indecent environment, poor housing, bushy surroundings, and exposed water in wells and gutters. These aforementioned characteristics are reproducing grounds for mosquitoes that in turn inject malaria parasites on the rural people. Malaria as a life-threatening disease is caused by parasites that are transmitted to people through the bites of infected female Anopheles mosquitoes (World Health Organization, 2016).
Despite being a preventable and treatable disease, malaria accounts for about 212 million of cases and 429,000 deaths globally in 2015 alone (World Health Organization, 2016). More than 80% of the estimated malaria deaths in 2012 occurred in just 17 countries, and 80% of cases occur in 18 countries, with the Democratic Republic of Congo and Nigeria together accounting for 40% of the estimated global total (World Health Organization, 2012; National Population Commission et al., 2012).
The recurrent nature of malaria and a coincidence of malaria peak season with harvesting season accentuated the burden for the rural poor who are already dependent on subsistence farming and with limited coping options (Adhanom et al., 2006; Chuma et al., 2006). Thus, malaria is expected to affect the income of farmers in the farming season. Evidence on the economic burden of malaria is important for prioritization of prevention and treatment service at the national and sub-national levels and facilitates better resource allocation in the health care system (McIntyre et al., 2006; Larg and Moss, 2011). Comparing evidence of economic burden of malaria from different settings, time periods, patient groups, and epidemiological profiles is challenging (Drummond, 2015), hence traditionally, studies that have attempted to estimate the economic burden of malaria have focused on the private and non-private medical costs associated with the disease, as well as some measure of the income that is forgone as a result of malaria morbidity and mortality (Jefferey and Pia, 2002).
There are no empirical evidence to investigate the effect of malaria on income of cocoa farmers, although there have been studies that addressed malaria effects on crop farmers in general. There have also been studies that focused on how sickness generally affect cocoa farmers; however, there is no study that focused on the economic effects of malaria on cocoa farmers. An intensified and increased commitment and financial allocation for malaria prevention and control measures have reduced the burden of malaria mortality rate among under-five children by 29% globally within five years since 2010 (World Health Organization, 2016), hence a little insight into the challenges posed by malaria on cocoa farmers will help policy makers especially non-governmental organizations interested in boosting cocoa exportation among developing countries, in formulating the right policies aimed at reducing malaria incidence among cocoa farmers.
MATERIALS AND METHODS
Area and scope of study
The study was carried out in Ondo State. It is situated between longitude 04° 15’ E and 06° 00’ E of the Greenwich Meridian and Latitude 5° 45’ N of the equator. The State has 18 LGAs with a population of about 3,440,000 of which the rural population constitutes about 1,700,000 people. Its land area is about 14,606 km2 (National Population Commission, 2006). In Nigeria, cocoa is mostly grown in the southwestern states with Ondo State being the leading producer with an average production of about 77,000 tonnes annually.
Sampling procedure and data collection
Multi-stage and proportionate sampling were used for data collection. At the first stage, three local governments noted for cocoa production were purposively chosen: Idanre, Ile-Oluji/Oke- Igbo and Owo. At the second stage, two villages were randomly selected from each of the chosen Local Government Areas. The villages were Alade-Idanre and Atoshin-Idanre from Idanre LGA, Bankemo farm settlement and Odotu farm settlement from Ile-Oluji/Oke-Igbo LGA and Iyere and Isuada from Owo LGA. At the third stage, proportionate sampling techniques was used : 35 cocoa farmers were randomly selected from each of the selected villages in Idanre, 30 cocoa farmers from each of the selected villages in Ile-Oluji/Oke-Igbo and 25 cocoa farmers from each of the selected villages in Owo. Finally, 70 cocoa farmers were proportionately and randomly selected from Idanre, 60 cocoa farmers from Ile-Oluji/Oke-Igbo and 50 cocoa farmers from Owo. From the sSampling frame of cocoa farmers in each of the LGAs, Idanre had the highest registered number of cocoa farmers with the Cocoa Farmers Association of Nigeria in Ondo State, followed by Ile-Oluji/Oke-Igbo and Owo, hence the use of proportionate sampling technique.
The sampling frame for the selection of the study units was obtained from records of the Ondo State Ministry of Health on cocoa farmers who visited local clinics and hospitals in the selected LGAs for malaria treatment in 2015. Only cocoa farmers whose names were on the records of the Ondo State Ministry of Health were identified to be in the sampling frame of the study. These names were later selected from the list of registered cocoa farmers in Ondo State, to form the sampling frame of the study. The names and addresses of these farmers were then used to locate them. To avoid duplication of respondents, the names of cocoa farmers visited were noted and a village was visited at a time before another village was visited until all respondents in each village selected for the study had been contacted to collect data for the study. Data obtained from the study had been examined for normality, multicollinearity and heteroscedasticity. STATA 10 software was then used for analyzing the data of the study.
Measurement and standardization of variables
Ordinary Least Square (OLS) estimator and the Maximum Likelihood (ML) estimator are suitable to investigate effects of independent variables on a dependent variable. However data with a normal distribution and one that is void of multicollinearity and heteroscedasticity is best suited for OLS regression technique. Maximum Likelihood estimator of error terms is suited for data in which variance of error terms is not constant. According to Gujarati (2013), “Maximum Likelihood (ML) estimators and the OLS estimators of the regression coefficients of the two-variable model are identical. This equality extends to models containing any number of variables. However, this is not true of the estimator of variance.” This is so because of differences in computation of variance. Gujarati (2013) stated that OLS estimator of variance takes into account the number of degrees of freedom whereas the ML estimator does not. Therefore, OLS gives more reliable estimate of variance than MLS and this informed the choice of OLS regression technique for estimation of model parameters.
The OLS regression model used to examine the effects of malaria infection on cocoa farmers’ income is represented thus:
Yi=f(X) + e. Where Yi , is the vector of endogenous variable and it representsed farmers’ annual income in Naira; X is a vector of independent variables and the independent variables included in the model were:
TDC= Total Direct cost of malaria treatment (in Naira);
NDY= Number of days of incapacitation caused by malaria (in the production season);
LAB= Additional labour cost incurred during the incapacitation period (in Naira);
OM= Orthodox method of malaria treatment (Yes=l, No=0);
TM= Traditional method of malaria treatment; (Yes=l, No=0);
FI= Frequency of visit to healthcare facility for malaria treatment (in number)
DI=Distance covered to visit health care facility from farmer’s’' home (in kilometres), where e represents the random error term capturing unexplained variables.
Descriptive statistics such as frequency distribution, means and percentages were used to identify strategies to reduce malaria infection among cocoa farmers.
RESULTS
Table 1 showed that 43.3% of the respondents earned below ₦300,000,.,. 11.2% earned between ₦301,000-600,000, 37.3% earned between ₦601,000-900,000 and 8.2% earned above ₦900,000. The average annual income of the respondents was ₦524,096. This finding is similar to a report by Oluyole et al. (2011) that the mean annual farm income of cocoa farmers in Nigeria was ₦578,250. The implication is that they may have enough money to spend to prevent or control malaria infection. Ajani and Ashagidigbi, (2008), reported that the average farm income of crop farmers in Oyo State was ₦ 9,974.17. This could signify that cocoa farming being principally export oriented in Nigeria is a high earning enterprise as compared with many other crop farming ventures.
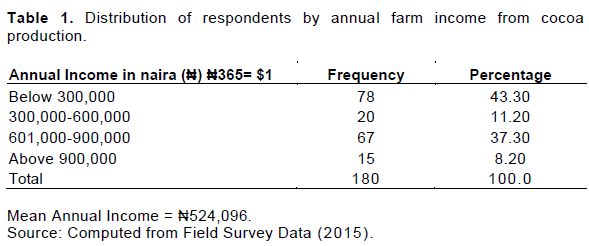
Table 2 presents the results of analysis on malaria factors which could affect the income of cocoa farmers. It showed that additional labour costs incurred by farmers during periods of incapacitation caused by malaria infection, the total direct cost of malaria treatment, the frequency of visits to medical centers, orthodox and traditional methods of malaria treatment had a significant effect on the income of the farmers..
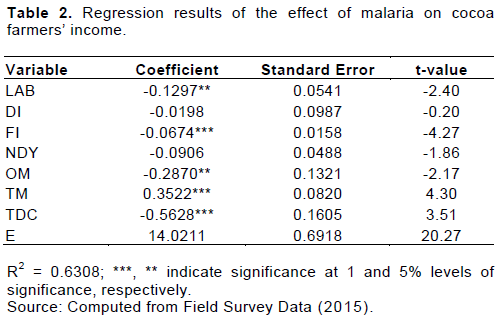
The number of days of incapacitation caused by malaria and distance covered to visit medical center had no significant effect on the income of the farmers.
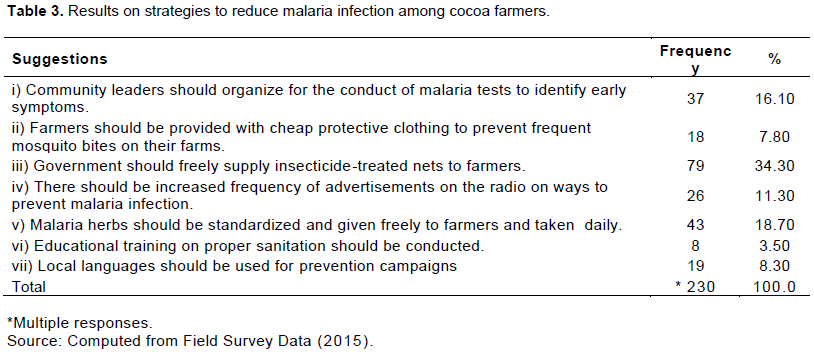
From Table 3, 16.1% of the respondents suggested that community leaders should arrange for periodic conduct of a malaria test to identify early symptoms among the cocoa fanners. This they believed would significantly reduce the time of absenteeism and thus farmers would not incur extra costs which could reduce their income. 7.8% of the respondents were of the opinion that fanners should be provided with cheap protective clothing against excessive mosquito bites on the farm. 34.3% of the respondents believed that insecticide treated nets should be made available by the government to the farmers and that farmers should be trained by health professionals on how to identify malaria symptoms early. 11.3% of the respondents were of the opinion that there should be increased frequency of advertisement on radio on strategies to prevent malaria and there should be house-to-house visits and sensitization on measures to prevent malaria. 18.7% of the respondents believed that malaria herbs should be standardized, packaged and given freely to the farmers. They also opined that it should be taken daily to destroy potential malaria parasites in the body. 3.5% of the respondents believed that community members should be educated on proper environmental sanitation to prevent malaria and 8.3% of the respondents opined that malaria prevention promotional campaigns should be undertaken in local languages and dialect.
DISCUSSION
The main focus of the study was to analyze the effect of malaria on income of cocoa farmers in Ondo State. Linear functional form gave the best fit among the various functional forms. The value of R2 is 0.631. This implies that 63.1% of the variations observed in farmers’ income were explained by the independent variables.
All the factors which could affect the income of farmers fit a priori expectations except for the traditional method of malaria treatment. From the results, there is a positive relationship between cocoa farmers’ income and the traditional method used by farmers for malaria treatment. This implies that as farmers use traditional methods for malaria treatment, their income increases. Traditional methods of malaria treatment such as the use of plant extracts and traditional healers attracts little or no cost to farmers. Findings from a Focus Group Discussion study on traditional methods of malaria treatment conducted by Nwakwasi et al. (2017) showed that the respondents asserted that traditional treatment for malaria was: cheaper, could be self-administered and had less chemical residue. Therefore, if such methods are effective for malaria treatment, farmers could recover from malaria infection within a short period of time to perform routine farm management activities in order to boost their productivity and income. There is a negative relationship between frequency of visit to health-care centers by the farmers and their income. This is expected because as farmers increase their visits to local clinics, private hospitals, and pharmaceutical shops for malaria treatment, their income will be reduced. Again, a negative relationship existed between distance covered to visit health-care centers and farmers’ income. This also is expected as the longer the distance a farmer travels to visit a health-care center for malaria treatment, the more the cost of transportation and this could adversely affect farmers’ income. This partly conforms with findings of Haliu et al. (2017) who stated that socioeconomic status, distance between patient’s residence and the health facility visited, incident of malaria in the last six months, level of the facility visited in the health system and availability of antimalarial drug in the health facility significantly influenced either direct cost, indirect cost or both. The additional labour cost incurred during periods of incapacitation also had a negative relationship with farmers’ income. This is in line with a priori expectations because as malaria affects farmers’ activities on their farms especially at crucial periods such as harvesting, spraying, pollination, weeding, pruning, e.t.c, labour cost tends to be higher and thus farmers’ income could be negatively affected. The days of incapacitation caused by malaria also had a negative relationship with farmers’ income. This is also expected because if farmers are absent during peak periods of farm activities, their output could be reduced because of several factors amongst which could be: disease outbreak due to untimely spraying of agrochemicals on cocoa trees, and over ripe cocoa pods could get spoilt on cocoa trees when farmers are incapacitated during harvesting periods. There could also be cases of theft when they are incapacitated for prolonged periods.
Also, from the result, at the 5% level of significance, the additional labour cost incurred by the farmers during periods of incapacitation had a significant effect on farmers’ income. This may be as a result of the labour alternatives used by the farmers especially during crucial periods of pollination and harvesting. At the 5% level of significance, the orthodox method for malaria treatment had a significant effect on farmers’ income. One reason for this could be as a result of the cost of malaria drugs and medical services (Verguet et al., 2016; Onwujekwe et al., 2010; Russel, 2004; Ayindenaba et al., 2014) posited that out-of-pocket payments for malaria treatment can impoverish some households who are already on ‘border line’ when it becomes recurrent and catastrophic in size, especially in a health system running without any mechanism for financial risk protection. Russel (2004) further stated that when the share of out-of-pocket payments is greater than 10% of the total expenditure/income, the risk of health expenditure can be catastrophic in size. At the 1% level of significance, the frequency of visit to health care facilities, total direct cost for malaria treatment and traditional method of malaria treatment had significant effects on farmers’ income. The number of days of incapacitation however did not have a significant effect on farmers’ income. This result was corroborated by a study conducted by Ajani and Ashagidigbi (2008). The study revealed that the days of incapacitation caused by malaria did not have significant effect on the income of farmers. Another study by Rwaheru (2011) had a contrary result. It showed that malaria infection and number of days lost due to malaria illness at the household level had a significant effect on agricultural crop production. This suggests the need for investigations on the extent to which malaria affects different types of farmers. The distance covered by respondents to visit health care centers did not have a significant effect on farmers’ income. This could indicate that health-care facilities in most of the communities are close to the farmers.
The regression result in Table 2 from the t-test showed that the joint effect of the malaria variables had a significant effect on the income of cocoa farmers; hence, the null hypothesis which states that the joint effect of malaria infection does not significantly affect the income of cocoa farmers was rejected and the alternate hypothesis which states that the joint effect of malaria infection significantly affects cocoa farmers’ income was accepted.
Based on the findings from the study, it was concluded that malaria affected the income of cocoa farmers in Ondo State. It was generally accepted that there should be increased frequency of advertisements on radio on strategies to prevent malaria and it should be done in local languages. They suggested that insecticide treated nets should be made available to the cocoa farmers by government and relevant non-governmental organizations. Although supply of insecticide treated nets to residents in many rural communities in Africa have been a major effort in tackling malaria by governmental and nongovernmental organizations, this finding show that there are yet some vulnerable communities having great economic potential to be reached with adequate supply of these nets for their populace.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors are thankful to Mr. Oginni for helping with data collection from the field and analysis of data obtained from respondents. The personnel of Cocoa Farmers Association of Nigeria (CFAN) who assisted with obtaining information on names and addresses of respondents are also appreciated.
REFERENCES
|
Adhanom T, Deressa W, Written HK, Getachew A, Seboxa T, Malaria.In Birhan Y, Hailemariam D, Kloos H (2006). Epidemiology and Ecology of Health and Disease in Ethiopia. 1st ed. Addis Ababa: Shama Plc. pp. 556-576. |
|
|
Ajani OIY, Ashagidigbi WM (2008). Effect of Malaria on Rural Households' Farm Income in Oyo State, Nigeria. African Journal of Biomedical Research 1:259-265. |
|
|
Ayindenaba DM, Akweongo P, Aborigo R, Awine T, Kweku AD, Asaana P (2014). Does the National Health Insurance Scheme in Ghana reduce household cost of treating malaria in the Kessena-Nankana districts? Global Health Action 7:23848. |
|
|
Bremann J, Mills A, Snow R, Steketee R, White N, Mendis K (2006). Conquering Malaria. In Disease Control Priorities in Developing Countries DT Jamison, JG. |
|
|
Chuma JM, Thiede M, Molyneux CS (2006). Rethinking the economic costs of malaria at the household level: evidence from applying a new analytical framework in rural Kenya. Malaria Journal 5(1):76. |
|
|
Drummond M (2015). Methods for the economic evaluation of health care programmes. Fourth edition.ed.Oxford, United Kingdom; New York NY, USA: Oxford University Press13:445. |
|
|
Gujarati DN (2013). Basic Econometrics Fifth edition. African Edition. Bell and Brain Ltd, Glasgow P 202. |
|
|
Hailu A, Bernt L, Wakgari D, Taye G, Eskindir L, Bjarne R (2017). Economic burden of malaria and predictors of cost variability to rural households in south-central Ethiopia. PLoS ONE 12(10):e0185315. |
|
|
Jefferey S, Pia M (2002). The Economic and Social Burden of Malaria. Insight review articles. |
|
|
Kwadwo AO, Felix, A Jifar T, Kwaw A (2009). The Linkages between Agriculture and Malaria: Issues for Policy, Research, and Capacity Strengthening. IFPRI Discussion Paper 00861:(1):9-14. |
|
|
Larg A, Moss JR (2011). Cost of illness studies: A guide to critical evaluation. (Practical Application). Pharmaco Economics 29(8):653. |
|
|
McIntyre D, Thiede M, DahIgren G, Whitehead M (2006). What are the economic consequences for households illness and of paying for health care in low-and middle-income country contexts? Social Science and Medicine 62(4):858-65. |
|
|
Mohammed BA, Matthew OA, Olugbenga AM (2018). Malaria Inicdence and Crop Productivity among Farming Hoseholds in Kabba/Bunnu Area of Kogi State, Nigeria. Journal of Agricultural Faculty of Gaziosmanpasa University 35(2):127-133. |
|
|
National Population Commision (NPC) (2006). Nigeria National Census: Population distribution by Sex, State, LGAs and Senatorial district: 2006 Census Priority Tables. P 3. |
|
|
National Population Commission (NPC), National Malaria Control Programme (NMCP), MEASURE DHS (2012). Nigeria Malaria Indicator Survey 2010' Final Report |
|
|
Nwakwasi RN, Nwachukwu I, Ifenkwe EA, Agwu EA (2017). Rural Household Attitude towards Traditional Methods of Malaria Treatment in South-East, Nigeria. Journal of Agricultural Extension 21:1. |
|
|
Oluyole KA, Ogunlade MO, Agbeniyi SO (2011). Socio-economic burden of malaria disease on Farm Income among Cocoa Farming Households in Nigeria. American-Eurasian Journal of Agricultural and Environmental Sciences 10(4):696-701. |
|
|
Onwujekwe O, Hansonk K, Uzochukwu B, Ichoku H, Ike E, Onwughalu B (2010). Are malaria treatment expenditures catastrophic to different socio-economic and geographic groups and how do they cope with payment? A study in southeast Nigeria. Tropical Medicine and International Health 15(1):18-25. |
|
|
Russel S (2004). The economic burden of illness for households in developing countries: a review of studies focusing on malaria, tuberculosis, and human immunodeficiency virus/acquired immunodeficiency syndrome. The American Journal of Tropical Medicine and Hygiene 71(2):147-155. |
|
|
Rwaheru AA (2011). The Effect of Malaria on Agricultural Production in Uganda. A Dissertation submitted to the School of Graduate Studies in partial fulfillment of the requirements for the award of a Master of Arts in Economics Degree of Makerere University. |
|
|
Verguet S, Memirie ST, Norheim OF (2016). Assessing the burden of medical impoverishment by cause: a systematic breakdown by disease in Ethiopia. BMC Medicine 14(1):164. |
|
|
World Health Organization (2012). World Malaria Report 2012. Geneva: World Health Organization. |
|
|
World Health Organization (2016). Do all mosquitoes transmit malaria? Fact sheet updated April, 2016. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


